Information Links
Related Conferences
Previous Issues Volume 6, Issue 3 - 2023
Soluble Fiber Supplementation as Treatment of Chronic Constipation in a Patient with Dolichomegacolon
Echevarría Constanza*
NP-Nutrición Personalizada, Buenos Aires, Argentina
*Corresponding author: Echevarría Constanza, NP-Nutrición Personalizada, Buenos Aires, Argentina; Email: [email protected]
Received Date: June 15, 2023
Publication Date: August 7, 2023
Citation: Echevarría C. (2023). Soluble Fiber Supplementation as Treatment of Chronic Constipation in a Patient with Dolichomegacolon. Mathews J Nutr Diet. 6(3):26.
Citation: Echevarría C. © (2023)
ABSTRACT
Constipation or chronic constipation (CC) should be considered as a complex and multifactorial disease. It is one of the most frequent gastrointestinal pathologies worldwide, and has a negative impact on patients' quality of life. Dolichomegacolon is a rare pathology characterized by a colon twice, or even three times, the normal size, both in diameter and length. It causes pain and chronic constipation in patients with this disease. Symptomatology that worsens over the years. We present the case of a 42-year-old woman diagnosed with dolichomegacolon and recurrence of her constipation after left hemicolectomy. The implementation of hygienic-dietary measures with the addition of soluble fiber supplementation resulted in favorable evolution.
Keywords: Constipation, Dolichocolon, Megacolon, Soluble Fiber
Abbreviations: CC: chronic constipation; NSAIDs: non-steroidal anti-inflammatory drugs; BSS: Bristol Stool Scale; Rx: x-ray; VCC: Video colonoscopy; BMI: Body Mass Index; RR: relative risk
INTRODUCTION
Constipation or chronic constipation (CC) should be considered as a complex and multifactorial disease. It is one of the most frequent gastrointestinal pathologies worldwide, and has a negative impact on patients' quality of life.
The average prevalence in adults in the general population is 16 % and up to 33.5 % in older adults [1].
It is defined as unsatisfactory defecation (sensation of incomplete evacuation), resulting from infrequent bowel movements, or with difficulty of expulsion (sensation of anorectal obstruction and need for manual maneuvers to facilitate evacuation), or both. However, this term is also used to describe a variety of symptoms, including hard stools, excessive straining, bloating and abdominal pain. [2].
According to its origin, CC can be primary or secondary. Primary constipation is the consequence of multiple pathophysiological alterations, the most important of which are altered colonic regulation of stool movement, together with lack of coordination of the anorectal neuromuscular apparatus and dysfunction of the brain-gut axis. While secondary constipation is caused by multiple causes, such as drugs (opioids, calcium channel blockers, NSAIDs), neurological disorders (Parkinson's disease), or metabolic diseases (diabetes, hypothyroidism) and even anatomical problems (anorectal and colonic diseases) [3].
It is important to remember that the act of defecating is complex; it involves neuromuscular structures that must be coordinated, and is influenced by water content and stool volume, fiber intake, gut microbiota, and psychological and behavioral disturbances.
The primary diagnostic approach should focus on the specific symptoms of CC, evaluate medications that could be its cause, as well as exclude organic disease and alarm symptoms.
It is also important to collect information on bowel habits. Stool form or the Bristol Stool Scale (BSS) is a method that has been found to be the most reliable instrument for assessing colonic transit compared to symptoms [4].
Figure 1: Bristol Stool Scale
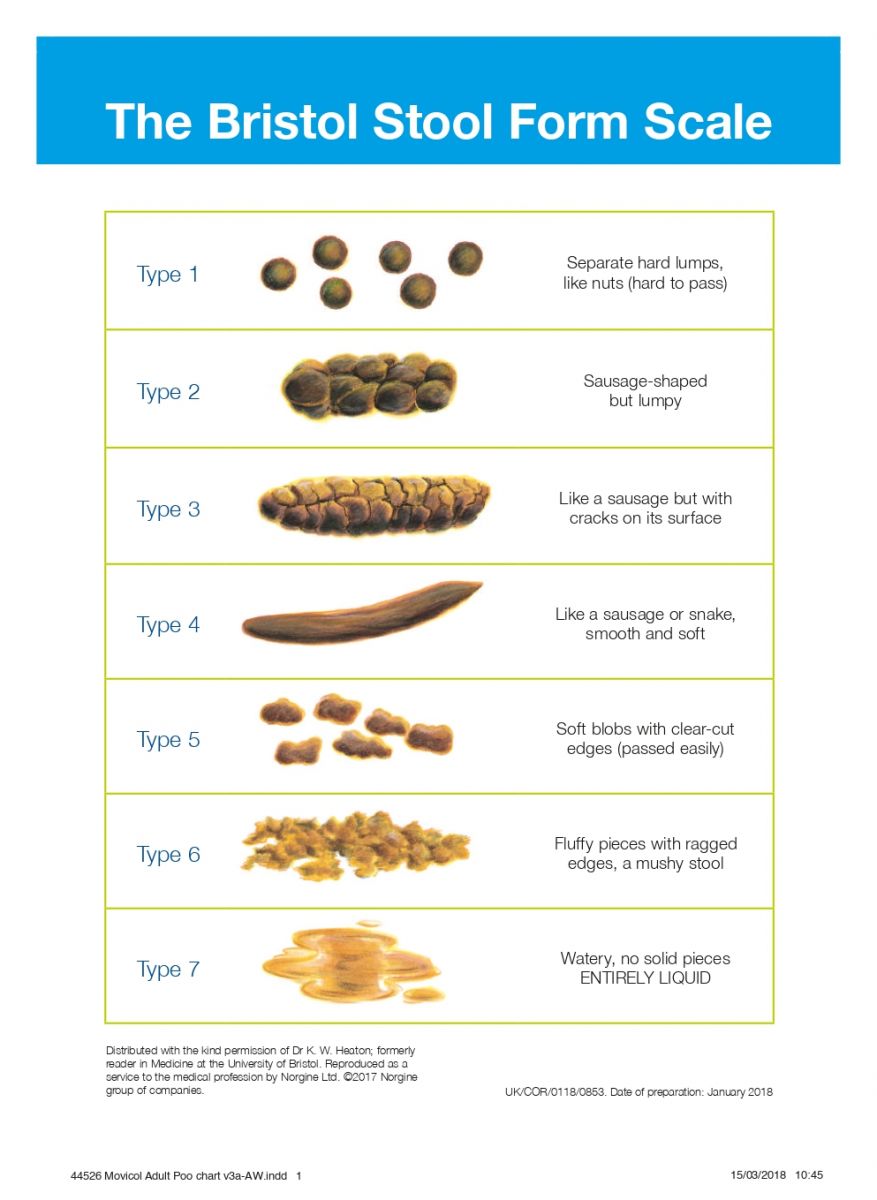
Figure 1: Type 1: separate hard lumps, difficult to pass, type 2: sausage-shaped, but lumpy; type 3: like a sausage but with cracks on its surface; type 4: like a sausage or snake, smooth and soft; type 5: soft blobs with clear cut edges; type 6: fluffy pieces with ragged edges, a mushy stool; type 7: watery, no solid pieces, entirely liquid, diarrhea.
No single diagnostic test provides a complete description of defecation, so a combination of these is generally used to assess structure, motor and sensory functions.
Advanced diagnostic studies of colon, rectal, and anal function are recommended in patients with chronic constipation and in those who have failed first-line treatments.
CASE REPORT
We present a 42-year-old woman referred by her gastroenterologist for having chronic symptomatic constipation that significantly affects her quality of life. She reports having temporarily stopped working and limited her social events. Pursuant to the anamnesis, it is known that she has been a smoker until a few months ago and that she has no other clinical history of importance. She started her consultations for chronic constipation in 2010. At that time, and due to lack of response to first-line treatments, she was indicated to undergo a colonic transit time test, which reported "obstruction of the outflow tract with moderate slow transit in general.
Diagnosis: Dolichomegacolon”.
The case was interpreted as acquired Dolichomegacolon secondary of chronic use of laxatives and antispasmodics. Due to the lack of symptomatic improvement, the obstruction due to fecal impaction and the persistence of intense pain, in the month of June 2010 they performed left colectomy.
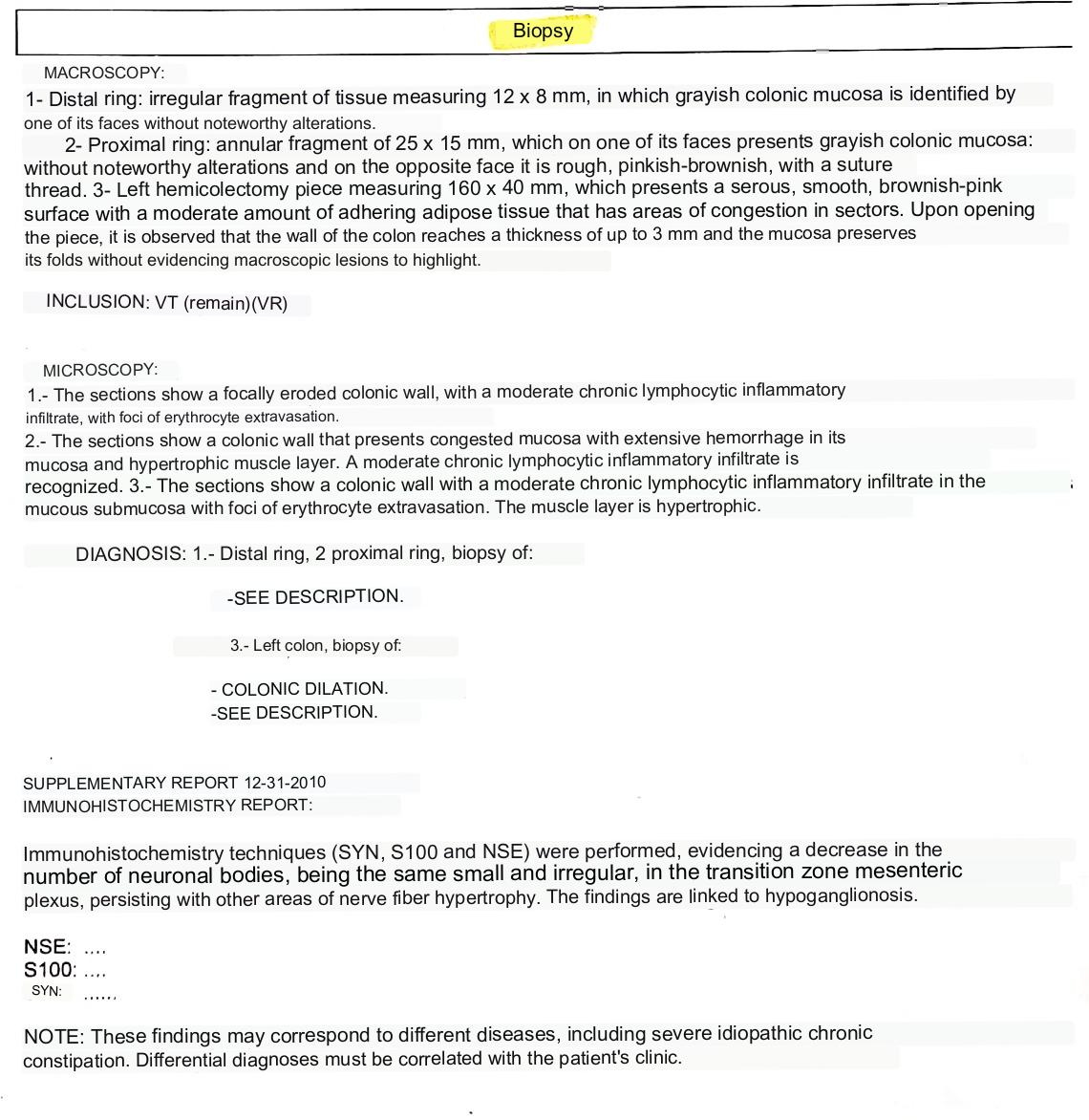
Figure 2: Biopsy.
Macroscopy
- Distal ring: irregular fragment of tissue of 12 x 8 mm, with grayish colonic mucosa with no significant alterations on one side.
- Proximal ring: annular fragment of 25 x 15 mm, with grayish colonic mucosa with no significant alterations on one side and the opposite side is rough, pinkish brown with suture thread.
- Left hemicolectomy piece measuring 150 x 40 mm, with serous, smooth, pinkish brownish surface with moderate amount of adherent adipose tissue with areas of congestion in sectors. At the opening of the specimen, it is observed that the colon wall reaches a thickness of up to 3 mm and the mucosa preserves its folds without showing macroscopic lesions to highlight.
Inclusion: VT (remain) (VR)
Microscopy
- Sections show a focally eroded colonic wall with a moderate chronic lymphocytic inflammatory infiltrate with foci of erythrocyte extravasation.
- Sections show a congestive mucosa colonic wall with extensive hemorrhage in the mucosa and a hypertrophic muscular layer. A moderate chronic lymphocytic inflammatory infiltrate is recognized.
- Sections show a colon wall with a moderate chronic lymphocytic inflammatory infiltrate in the mucosa and submucosa with foci of erythrocyte extravasation. The muscular layer is hypertrophic.
Diagnosis: 1 distal ring, 1 proximal ring, biopsy of: see description.
3. Left colon, biopsy of: colonic dilatation, see description.
Supplementary report 12/31/2010 Immunohistochemistry report
Immunohistochemistry techniques were performed (SYN, S100 and NSE) showing a decrease in the number of neuronal bodies, being small and irregular in the mesenteric plexus of the transition zone, persisting with other areas of hypertrophy of nerve fibers. Findings are related to hypoganglionosis.
NSE S100 SYN
Note: these findings may correspond to different diseases, including idiopathic severe chronic constipation. Differential diagnoses should be correlated with the patient's clinical history.
Dolichomegacolon is a rare pathology characterized by a colon twice, or even three times, the normal size, both in diameter and length. It causes pain and chronic constipation in patients with this disease. Symptomatology that worsens over the years.
EVOLUTION
- March 2011: consultation to the emergency department for bloating, abdominal pain and decreased stool frequency. Abdominal X-ray: "abundant colonic debris". Indicated treatment: polyethyleneglycol.
- 2014: new consultation to the emergency department for bloating, abdominal pain and decreased stool frequency. Abdominal X-ray: "abundant colonic debris". Indicated treatment: lactulose.
- Video colonoscopy (VCC) in 2015. Normal study. Colectomy scar. Hemorrhoids. Indicated treatment: Trimebutine+ simethicone.
- July 2016: complete blood test without particularities. Antibodies for celiac disease: negative. Normal thyroid function. Normal glycemia.
- At the first consultation in this center (December 2021) she mentions bowel movements every 5-6 days, without blood, Bristol 1-2. Epigastric pain, nausea and abdominal distension.
- Family history: married, no children. Currently on leave from work for anxiety disorder. Sedentary, emotionally labile. Significant impairment of her quality of life. Very much family support. Chronic fatigue.
- Medication: Flouxetine 20mg, clonazepam 0.5. Under psychiatric follow-up. Currently without laxatives. She mentions no response to 30 days of otilonium bromide. She uses polyethylene glycol as a "rescue" laxative in case of more than 7 days without bowel movement.
- Nutritional evaluation: usual weight (up to 6 months ago) 62kg. Height 1.67m. Current weight 59kg. BMI 21.1kg/m2 (normal), Decrease of 4.8% of her usual weight in 6 months (not significant). High fiber intake pattern. She skips some meals due to a feeling of fullness. Recognized lactose intolerant.
- Initial behavior: diet low in insoluble fiber and with moderation in fermentable carbohydrate intake was indicated with the aim of controlling symptoms of abdominal discomfort. Hygienic dietary measures were suggested for a better defecation habit: Light physical activity and consumption of at least 2 liters of water per day. Fractionated intake: 4-6 meals.
- The aim of the treatment was to correct intestinal alterations, improve symptoms and the patient's quality of life. Comprehensive management should be considered, including hygienic and dietary measures, which include: doing exercise (improves intestinal transit and constipation symptoms), adopting a correct posture (favors the opening of the anal rectum angle) and performing a pushing maneuver without excessive effort, as well as taking advantage of the moments of greater colon motor activity (e.g. upon awakening or after food intake), and the consumption of 1.5 to 2 liters of water per day.
- At the control visit, the patient reported marked symptomatic improvement, less distension, but continued with bowel movements every 5 days, Bristol 2. It was suggested the incorporation of a soluble fiber supplement (60 % partially hydrolyzed guar gum + 40 % inulin) in an initial dose of 5g/day diluted in 250-300ml of water or juice (non-fractionated intake).
The consumption of fiber, through food rich in fiber (kiwi, flax) or supplements, can accelerate intestinal transit, since it is known that the increase in volume in the formation of the bolus stimulates colonic peristalsis. In addition, the fluid retention caused by soluble fiber is useful to improve the consistency and promote the stool evacuation. The potential therapeutic effects, low cost, safety profile and other potential health benefits of dietary fiber justify its increased intake as an initial treatment.
After 4 weeks, the patient reported adequate tolerance and acceptance of the supplemented fiber resulting in a marked improvement in bowel habit, achieving daily, effortless bowel movements, Bristol 4. She continued with psychological support and showed improvement in her mood. She resumed scheduled physical activity 2 to 3 times a week.
Most available guidelines recommend a diet rich in fiber, with a recommended intake of at least 25-30 g per day. Systematic reviews support the recommendation to increase dietary fiber intake and, in particular, soluble fiber to improve symptoms in patients with constipation [1].
A meta-analysis evaluating seven controlled clinical trials showed that 77 % of patients who received fiber supplementation responded to therapy, increasing stool frequency and achieving softening of stool consistency, compared to 44 % of patients who received placebo (relative risk -RR- of success =1.71, p= 0.003) [5].
However, it is very important to mention that in some patients, dietary fiber or supplements may aggravate the symptoms associated with constipation, such as bloating and flatulence, so the recommended dose will depend on the tolerance of each patient.
CONCLUSION
Dolichomegacolon is a predominant pathology in early stages of life. Clinical suspicion in adult patients requires precise knowledge and understanding of the disease because its presentation is usually exceptional. Although the etiopathogenesis of dolichomegacolon in these cases is poorly understood, it is accepted that the use of different psychotropic drugs play a prominent role. Advances in diagnosis and treatment have led to the availability of multiple therapeutic options to provide greater relief of symptoms and a better quality of life for patients.
It must not be forgotten that all surgical procedures have a certain morbi-mortality and that conventional strategies (hygienic dietary measures) have demonstrated therapeutic effectiveness and should be recommended for all patients as a first-line intervention.
Soluble fiber supplementation was helpful in the management of constipation in this patient.
REFERENCES
- García-Zermeño KR, Remes-Troche JM. (2021). Constipación crónica. Conceptos actuals desde la fisiopatología hasta el tratamiento. Acta Gastroenterol Latinoam 51(1):14-28
- Scott SM, Simrén M, Farmer AD, Dinning PG, Carrington EV, Benninga MA, et al. (2020). Chronic constipation in adults: Contemporary perspectives and clinical challenges. 1: Epidemiology, diagnosis, clinical associations, pathophysiology and investigation. Neurogastroenterol Motil. 2020:e14050.
- Rao SS, Rattanakovit K, Patcharatrakul T. (2016). Diagnosis and management of chronic constipation in adults. Nat Rev Gastroenterol Hepatol. 13(5):295-305.
- Lewis SJ, Heaton KW. (1997). Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 32:920-924.
- Christodoulides S, Dimidi E, Fragkos KC, Farmer AD, Whelan K, Scott SM. (2016). Systematic review with meta-analysis: effect of fibre supplementation on chronic idiopathic constipation in adults. Aliment Pharmacol Ther. 44:103-116.