Previous Issues Volume 1, Issue 1 - 2016
Barriers Facing Multicultural Participants in a University Weight Loss Program: A Preliminary Study
Marcia Magnus1 and Morgan Gay1
1Department of Dietetics & Nutrition, Florida International University, Miami, Florida, USA.
Corresponding Author: Marcia Magnus, Department of Dietetics & Nutrition, Florida International University, Miami, Florida, USA, Tel: +305-348-1989; E-Mail:[email protected]
Received Date: 11 Feb 2016 Accepted Date: 23 Mar 2016 Published Date: 02 Apr 2016
Copyright © 2016 Ohta T
Citation: Magnus M and Gay M. (2016). Barriers Facing Multicultural Participants in a University Weight Loss Program: A Preliminary Study. Mathews J Nutr Diet. 1(1): 002.
ABSTRACT
The objective of this study was to examine exercise and dietary barriers, and assess the usefulness of program features among multiethnic Blacks and Hispanics who were enrolled in a university weight loss program. The intervention included two nutrition meetings, an individualized recommended daily calorie level, group exercise sessions and a recommended Biometrics meal plan. Using a longitudinal design over four 16-week semesters, an online questionnaire was administered at the mid and end-point to weight loss program participants. Among the 66 participants, 86% were female; 52% were multiethnic Hispanic (Cuban American, Mexican American, Central and Latin American), 20% were multiethnic Black (African American, Haitian American, English-speaking Caribbean American). Mean weight loss was 3.81 pounds, with no significant differences between faculty/staff (4.81 pounds), and students (2.97 pounds). There were no significant gender differences for most exercise barriers except that women were almost twice as likely to cite the boredom of exercise compared to men. There were no significant gender differences among barriers to eating right except that males were more likely to cite the difficulty of eating right as a barrier than females. On average, the “very useful” perception of the Biometrics meal plan dropped from 23% to 5% over the course of 16 weeks for all four semesters. These data suggest a need for formative evaluation to repeatedly assess the usefulness of dietary and exercise features. The cultural appropriateness of dietary recommendations prevailed as an ongoing barrier to weight loss among multicultural program participants.
INTRODUCTION
Throughout the US and the world obesity has become a very serious problem which shows no signs of abatement. Any weight loss program faces the uphill battle of identifying an approach that would aid in reducing participant dropout, promote adherence, and increase long-term adaptation of behavioral and dietary strategies that promote maintenance of weight-loss [1]. Joining an employee-based group weight loss program has been recommended to improve outcomes in the short-term and long-term due to the social support which the program offers [2]. Other barriers may include dissatisfaction with the meal plan, lack of support from spouse/family, inconvenience of shopping for or preparing food, program fees, or lack of child-care [1,3]. The purpose of this preliminary research study was to examine the barriers facing multiethnic Blacks and Hispanics who enrolled in a 16-week university weight-loss program. The hypotheses under examination included:
- Barriers to eating right and exercise vary by gender among multiethnic Blacks and Hispanics. This hypothesis was developed because there are no reports in the published literature on the barriers to weight loss among multiethnic Blacks and Hispanics.
- Average weight loss will be greater for faculty/staff than for students. In the absence of current published reports on variation in weight loss among faculty, students and staff, this hypothesis was based on previous anecdotal data which indicated that weight loss was higher among faculty/staff than for students.
- Participants' perception of the usefulness of the Meal Plan program is higher at the beginning of the program compared to the midpoint and at the end of the program. Anecdotal reports from participants indicated early satisfaction with the news of the program's Meal Plan, but this converted to disappointment by the end of the program.
- BMI will decrease and lung capacity will increase pre- to post-program. The weekly training group sessions were designed to decrease BMI and increase lung capacity.
- At the end of the program, the usefulness of some program features will be higher than others. The 16-week program offered 12 program features and it was theorized that some would be perceived as more important than others.
This study was motivated by the disproportionately higher rates of overweight and obesity among Blacks and Hispanics. There are no published studies which examine weight loss barriers specifically among multiethnic Blacks and Hispanics. Few studies have explored barriers non-Whites. The university weight loss program under study was located in a county where 72.3% of homes do not speak English as a first language with the dominant ethnicities being Cuban, Mexican, Central and Latin American, and Haitian American [4]. Wang et al [5] quantified barriers to healthy eating and revealed that over the course of a 24-month weight loss program among 210 university employees (21.9% of whom were non-White), changes in BHE total and subscale scores were positively associated with changes in total energy and fat intake (P < .05) as well as weight (P < .01). The authors recommended that among multicultural program participants, planners need to assess barriers to healthy eating over the course of a weight loss program. Venditti et al (6) interviewed 1076 overweight men and women from 27 nationwide centers. Approximately 48% were non-Caucasian. Top weight loss barriers reported were: selfmonitoring (58%); social cues (58%); holidays (54%); low activity (48%); and internal cues (thought/mood) (44%). A majority of the weight loss barriers were significantly associated with younger age, greater obesity, and non-Caucasian race/ethnicity (p-values vary). Pawlak and Colby identified the barriers to eating health foods among 57 African Americans as: price, taste, not being able to find or cook healthy foods and the absence of social support. Diaz et al. [8] used focus groups among 19 Latino women and two men and revealed that most respondents explained that the heavier body preference was something that had been instilled in them since their childhood [7]. Among 15 overweight Mexican American women, Hoke et al [9] reported barriers among 15 Mexican American as: stress; lack of self-control; effort; control by others now and in the past; social influences; and cultural influences. There are no published studies weight loss barriers facing multiethnic Hispanic (Mexican, Cuban, South American) or multi ethnic Blacks (African American, Caribbean American, Haitian American, Africans from Africa). In the absence of data on dietary and exercise barriers in this population, this study was designed to assess those barriers among multiethnic Blacks and Hispanics.
METHODS
sample
The sample for this study consisted of 66 participants over a four-semester period. This was the optimal sample size based on a Wilcoxon Mann-Whitney calculation with 80% power using a Wilcoxon rank sum test, alpha = .05, and a medium/large effect size (d = .7), using sample sizes of 33 per group (faculty/ staff and students) [10]. The sample size calculation as based on the intention of this study was to compare mean weight loss among faculty/staff and students on the other hand. Faculty, staff and students at a major metropolitan university signed up for a semester-long weight-loss program. The only criterion for inclusion in the study was participation in the weight loss program. Participants' medical history and family medical history, and known diseases such as thyroid conditions, kidney disease, chronic obstructive pulmonary disease; and medication use were assessed. If patients scored in the high-risk category, a physician's clearance was required for participation in the program.
Intervention
Program components included a Biometrics meal plan, two nutrition seminars; and pre-post measurements of body weight, BMI and lung capacity. The Biometrics meal plan was developed by a team at the University of Texas Southwestern Medical Center in Dallas, TX. The meal plan follows the guidelines of the American Heart Association, the Academy of Nutrition and Dietetics and the American College of Sports Medicine. In the Biometrics meal plan, clients choose meals from Italian, seaboard, Continental, Oriental, classics and vegetarian. The two 1-hour nutrition seminars focused on Portion Distortion and Sugar Shockers. BMI was calculated based on weight and height measurements which were taken from a Detecto Eye Level Physician Scale with a height rod. In a private room, participants' height and weight were measured prior to exercise class by the personal trainer, with clothes on, and shoes off. The time of day varied according to the time of the participant's class. Fluid intake and activity level were not assessed. Lung capacity was assessed from a 3-minute step test at the beginning of the program and at the end by the participant's personal trainer prior to exercise class. Fluid intake and activity level were not measured. Recommended daily calorie level was determined by breathing into the tube of the ReeVue indirect calorimeter for 10 minutes, after fasting. All one-hour training sessions were conducted by a certified personal trainer in groups of three to seven participants for three sessions per week. The duration of each semester was 16 weeks. This study was a four-semester a longitudinal design. Approval was secured from the university's Institutional Review Board.
Instrument
Based on a review of the published literature on barriers to weight loss in predominantly multicultural populations (Figure 1), a 17-item mid-program questionnaire and 21-item end-of-program questionnaire were developed to assess preand post-program changes and it was administered electronically using Qualtrics Labs, Inc. software, Version 23949 of the Qualtrics Research Suite. Copyright © 2011 Qualtrics Labs, Inc. http://www.qualtrics.com. Part 1 of the questionnaire assessed demographic indicators such as age, gender, university status (faculty/staff or student), ethnicity, and weight loss goals. Part 2 examined participants' perceptions of the Biometrics meal plan: its usefulness, barriers to using the meal plan, previously tried meal plans, how often the meal plan was used, and if participants would recommend the meal plan to a friend. Additional aspects of the meal plan--menu plans, shopping list, substitutions list, recipes, the advantages and barriers to implementing the meal plan--were also explored. Part 3 of the questionnaire examined exercise patterns, barriers to exercise and eating right, and how both barriers might have changed since beginning the program. An incentive of one month of free personal training was offered to the first 50 survey respondents for completing the questionnaire.
Figure 1:Barriers among Multicultural Weight Loss Participants.
| Barriers Among Multicultural Weight Loss Participants | |||
| Study | Purpose | Sample | Results |
| Wang et al., 2015, North Carolina. | Changes in perceptions of barriers to healthy eating and its impact on dietary intake and weight loss using the 22-item Barriers to Healthy Eating (BHE) scale. | N = 210 84.8% female; well-educated; 78.1% White, 21.9% Non-Whites. | The BHE total score decreased from baseline to 6 months, and increased significantly slightly from 6 to 24 months (p < .001). Changes in BHE total and subscale scores were positively associated with changes in total energy and fat intake (p < .05) as well as weight (p < .01). |
| Venditti et al., 2014, 27 nationwide centers. | Barriers and approaches used to improve adherence. | N = 1076 68% female, 48% non-White. | Top weight loss barriers reported were: selfmonitoring, social cues 58%; holidays 54%; low activity 48%; and internal cues/thought/ mood. |
| Pawlak R, Colby S, 2009, North Carolina. | Barriers regarding healthy foods. | 57 African Americans, mean age 50 years old, 58.1% were females. | The high price of healthy foods was reported as the biggest barrier to healthy eating; other barriers included healthy food being less palatable, not being able to find and/or cook healthy foods, and the absence of social support. |
| Diaz et al, 2007, Charleston SC | Experiences, attitudes and barriers to weight loss. | N = 19 Latinas, 2 Latinos who were overweight. | Mixed messages about recommended body weight from health professionals and Latino culture was a major theme. They expressed a desire for culturally appropriate nutrition education. |
| Hoke et al, 2006, New Mexico. | Explanatory factors in weight loss and health among rural Mexican American women. | N = 15, overweight Mexican American women. | Participants identified barriers to healthy eating as: stress; lack of self-control; effort; control by others now and in the past; social influences; and cultural influences. |
Statistical Analyses
The statistical analyses used in the study were parametric and non-parametric tests run using SPSS version 24. The nonparametric tests used were Mann-Whitney U, Wilcoxin Signed Rank Test, Chi Square Test, and the Friedman Test. The Parametric tests used were Independent T-test, Pearson Correlation, and Mean measurements.
RESULTS
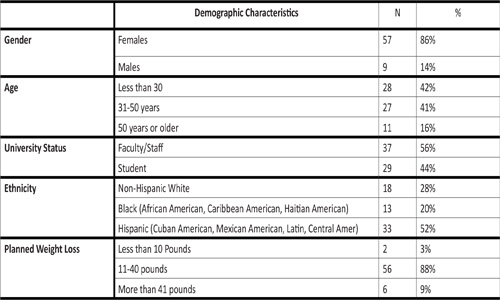
Enrollment in the university weight loss program averaged 63 participants over four semesters and survey data were derived for an average of 9 participants in each semester. The average response rate for each semester was 7%. Data from non-responders were not included in the analysis. Each semester's attendance ranged from 86 to 24. Respondents were mostly female, under age 50, 52% multi-ethnic Hispanic and 20% multi-ethnic Black, and most wanted to lose between 11- 40 pounds (Table 1).
Table 1: Barriers among Multicultural Weight Loss Participants.
There were no significant gender differences for most barriers to exercise (Table 2).
Table 2: Weight Loss Participants' Perceptions of Minor, Medium and Major Barriers to Exercise by Gender
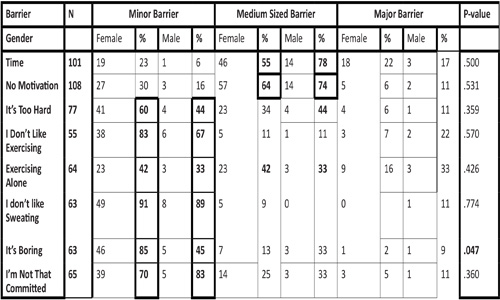
However, an independent-samples t-test revealed a significant gender difference to the reported boredom of exercise (p < .05). Approximately 85% of females and 45% of males described the boredom of exercise as a minor barrier, and 13% of females and 33% of males described it as a medium-sized barrier. The relationship between barriers to eating right and gender were assessed using an independent samples t-test (Tables 3, 4).
Table 3: Weight Loss Participants' Perceptions of Minor, Medium and Major Barriers to Eating Right by Gender-Part 1.
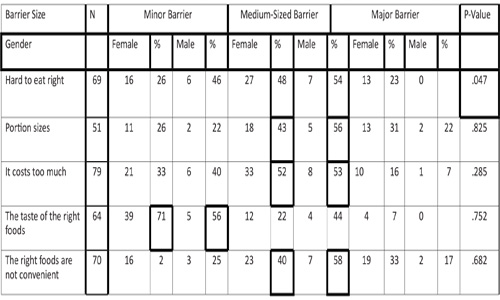
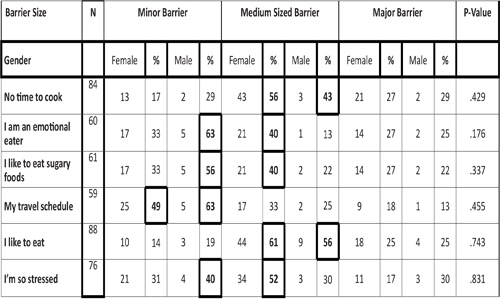
Table 4: Weight Loss Participants' Perceptions of Minor, Medium and Major Barriers to Eating Right by Gender-Part 2.
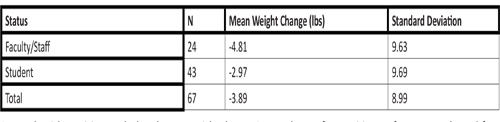
There was no significant gender difference in barriers to eating right except for the difficulty of eating right with M = 1.56 (males), 1.18 (females); SD = .726 (males), .434 (females), t (62) = 2.156, p =.047. Approximately 46% of males and 26% of females described the difficulty of eating right as a minor barrier. Approximately 23% of females and no males described the difficulty of eating right as a major barrier. A Mann-Whitney test indicated that the mean weight change for 67 participants was -3.89 ± 8.99 pounds (Table 5). The Mann-Whitney test revealed a U = 493 z = -.294, p = .769 therefore no significance was found between mean weight change and university status (faculty/staff versus students). An additional Mann-Whitney test was used to differentiate between faculty and staff weight change revealed that there were no statistically significant differences in weight loss among faculty and staff members (U=29, z= -1.668, p = .095). A Pearson correlation test results showed a weak positive correlation between age and weight change, Pearson, r = .14, n = 66, p = .22. A Mann-Whitney U test revealed no significant difference between weight change and gender with U= 483 z = -.584 and p = .559.
Table 5: Mean Weight Change among Faculty/Staff and Students.
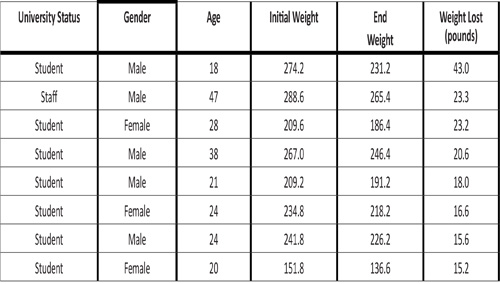
Among the eight participants who lost the most weight, there were five males and three females, seven were students, and mean weight loss over 16 weeks was 21.9 pounds (Table 6). Among the top five participants, four were male, and four were students.
Table 6: Characteristics of Participants Who Lost the Most Weight.
Satisfaction with the Biometrics Meal Plan varied significantly throughout the program (Table 7). The Wilcoxon signed rank test revealed a p-value of .001 and z=-3.20: a significant reduction in usefulness of the meal plan over the course of each 16-week semester. Approximately 30% of the participants described the biometrics program as "very useful" at the midpoint of the program, while only 14% indicated that it was "very useful" at the end of the program. The change in usefulness responses was consistent over the course of the four semesters. A Mann-Whitney U test revealed no significant difference in barriers associated with the biometrics meal plan from mid-program to end-of-program (Table 8). Participants repeatedly struggled with barriers over the course of the 16- week semester. There were no statistically significant differences in barriers between faculty/staff and students.
Table 7: Usefulness of the Biometrics Meal Plan throughout the Program (N = 88).
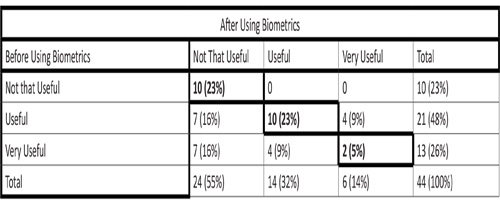
The participants who chose the same answer before and after using Biometrics are bolded P = .003.
Table 8: Changes in Mean Usefulness Ratings of Biometrics Meal Plan. (1: Very Useful, 2: Useful, and 3: Not that Useful)
.jpg)
A Friedman test on participants' perceptions of the usefulness of different program features revealed significant differences (p = .000) with the personal training sessions being very useful (Figure 2). The least useful features were the winning prize, and the meeting to log calories.
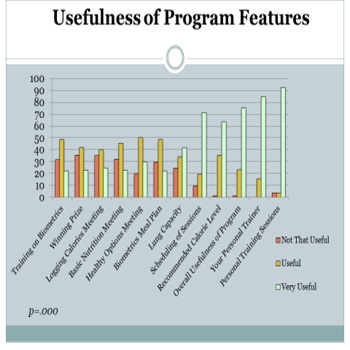
Figure 2: Usefulness of different programme features
A Chi-square test revealed there was no significant difference in the number of previous diets between the number of previous diets between students and faculty/staff. Due to the small number of male program respondents, it was not possible to test that hypothesis that women, students, and those with larger weight loss goals, those who had tried more diets in the past lost more weight than men, faculty/staff, and those with smaller weight loss goals and those who had tried fewer diets. A Student's T-test revealed statistically significant changes in BMI with a M = 31.7 (pre) and M = 31.1 (post), mean change = .63, t(75) = 4.14, p = .00. A similar test for lung capacity also revealed significant difference between pre- and post-program scores M = 126 (pre), M = 112 (post), mean change = 13.6, t(18) = 3.67, p = .002. Approximately 53% of men and 52% of women in this study cited the high cost of healthy foods as a barrier. Since Blacks and Hispanics earn 30% less than Whites, a culturally sensitive weight loss program for these populations would offer multiple recommendations on how to spend less on food and enjoy tasty healthy foods.
DISCUSSION
Despite the incentive of one-month of free personal training for the first 50 survey respondents, the 7% response rate to the electronic Qualtrics questionnaire and the 30% return the final weigh-in represent limitations to the study. Of the 195 program participants for over the four semesters of the program, 75% were repeat participants. Many respondents indicated that they had already completed the questionnaire in earlier semesters and were reluctant to complete additional questionnaires in subsequent semesters. The incentive was described as minimally useful. It may be beneficial for future researchers to attend the initial sign-up and explain that they will be sending electronic questionnaires at the middle and end points for each semester. Participants' medical history and family medical history were screened and physician clearance was required for enrolment in the weight loss program. While diseases such as thyroid conditions, kidney disease, chronic obstructive pulmonary disease; and certain medications represent confounding factors for weight loss, there is no reason to believe that these conditions exacerbated or reduced weight loss. Due to adequate physician monitoring, none of the participants were excluded from the program by their physicians.
Hypothesis 1-Barriers to eating right, and exercise vary by gender-was rejected. This study showed that participants struggled throughout the program because they liked to eat certain foods, and that they had difficulty finding time to cook healthy meals. Future studies could offer a cooking class for busy participants. The cultural inappropriateness of the meal plan constituted an additional barrier to eating right loss among these multicultural participants, as has been demonstrated among Mexican American women [9].
Hypothesis 2-Average weight loss will be greater for faculty/ staff than for students was accepted. Faculty and staff lost an average of 4.81 pounds, compared to 2.97 pounds for students, although the difference was not statistically significant.
Hypothesis 3-Participants' perception of the usefulness of the Meal Plan program is higher at the beginning of the program compared to the midpoint and at the end of the program-was accepted. The decline in usefulness of the Biometrics Meal Plan proved to be a valuable finding. The "very useful" perception of the Biometrics meal plan dropped from 23% to 5% over the course of 16 weeks. Informal interviews indicated that participants were happy to hear that they would receive a meal plan, until they discovered that it did not respond to their cultural norms. Program participants reported that the recipes were too time-consuming, hard to prepare, were not "good go-to meals" and were culturally inappropriate (“We don’t eat meatloaf!”). The decline may also have been due to its minimal emphasis on multi-ethnic Hispanic and African American, Caribbean American and Haitian American foods. Although the Biometrics Meal Plan was developed in Pennsylvania, the program participants were 52% multi-ethnic Hispanic and 20% multi-ethnic Black. The meal plan was not adapted to meet the dietary norms of the target population. Considering that ethnic foods are main predictors of nutrient intake levels among ethnic populations (Magnus and Enogieru, program planners are advised to conduct formative evaluation of the dietary component of weight loss programs especially among non-Whites [11].
Hypothesis 4-BMI will decrease and lung capacity will increase from pre- to post-program--was accepted because the mean change in BMI was -.63, and lung capacity (assessed as heart rate during a 1-minute step test) decreased on average by -14 bpm. Many participants did not attend the final weigh-in because they reported that they weighed themselves at home. This could be because they did not lose the amount of weight they set out to lose, or because they did not want to come in for the weigh-in when they could do it from their home. Hypothesis 5-At the end of the program, the usefulness of some program features will be higher than others-was accepted. The most useful Biometrics Meal Plan feature was the “personal recommended calorie level” and this did not vary from mid-program to end-of-program. The most useful program feature was the "personal training sessions" and least useful feature was "training on the Biometrics meal plan". Similar to data among Whites from Burke et al [1], these multicultural program participants expressed more dissatisfaction with dietary program features compared to the exercise program features. This study did not assess weight misperception (expressed as underestimation of weight category) which was documented by Paeratakul in 31.7% of healthy weight adults, 38.1% of overweight adults, and 8.1% of obese adults among 17,270 multiethnic adults who were sampled from the 1999-2006 National Health and Nutrition Examination Survey [12]. Dorsey showed a higher prevalence of weight misperception among overweight and obese men and women, racial and ethnic minorities, men; and among both men and women who have lower education levels [13]. Since Chang and Christakis showed that self-perception of overweight may have more impact on one's decision to lose weight than actual weight status, planners of weight loss programs may need to be assess and respond to the extent of misperception in their target populations [14]. This is especially true among populations who have cultural tolerance to and preference for obesity-Mexican American women and African American women [13]. They are more satisfied with their bodies at higher weights than Whites. Future researchers may need to conduct formative evaluation repeatedly on weight misperception and to assess how weight loss varies with weight perception. Although there is no evidence to support the theory, it is possible that observer bias could have affected measurement of weight, height and lung capacity because these indicators were measured by the personal trainer of each participant. Future studies may need to adopt strategies which reduce observer bias. Similarly, in this study, fluid intake was not monitored for weight and lung capacity measurements. Future studies may wish to acquire this information in an effort to account for this confounding variable.
CONCLUSION
The United States non-White population is expected to increase to 50% by 2050. To help program participants overcome dietary and exercise barriers to weight loss, planners of weight loss interventions among multiethnic Blacks and Hispanics need to identify dietary and exercise barriers and offer multiple recommendations on overcoming barriers. During the 16-week weight loss program, mean weight loss among faculty/staff was 4.81 pounds, and 2.97 pounds for students, although these were not statistically significant. These data suggest that there are no gender differences in barriers to eating right and exercise among multiethnic Blacks and Hispanics. It is also important for planners to use formative evaluation to repeatedly assess the usefulness of program features especially the cultural appropriateness of dietary recommendations. In this way, less useful features could be eliminated from the intervention, and more useful features could be emphasized.
REFERENCES
- Burke LE, Steenkiste A, Music E and Styn MA. (2008). A descriptive study of past experiences with weight-loss treatment. J Am Diet Assoc. 108(4), 640-647.
- Rigsby A, Gropper DM and Gropper SS. (2009). Success of women in a worksite weight loss program: Does being part of a group help? Eating Behav. 10(2), 128-130.
- French SA, Neumark-Sztainer D, Story M and Jerffery RW. (1998). Reducing barriers to participation in weight-loss programs in low-income women. J Am Diet Assoc. 98(2), 198-200.
- United States Census Bureau. Version current 11 March 2013.
- Wang, J, Ye L, Yaguang Z and Burke L. (2015). Impact of Perceived Barriers to Healthy Eating on Diet and Weight in a 24-Month Behavioral Weight Loss Trial. Journal of Nutrition Education and Behavior. 47(5), 432-436.
- Venditti E, Wylie-Rosett J, Delahanty L, Mele L, et al. (2014). Short and long-term lifestyle coaching approaches used to address diverse participant barriers to weight loss and physical activity adherence. International Journal Of Behavioral Nutrition & Physical Activity. 11(1), 1-23.
- Pawlak R and Colby S. (2009). Benefits, barriers, self-efficacy and knowledge regarding healthy foods: perception of African Americans living in eastern North Carolina. Nutr Res Pract. 3(1), 56-63.
- Diaz VA, Manious III AG and Pope C. (2007). Cultural conflicts in the weight loss experience of overweight Latinos. International Journal of Obesity. 31(2), 328-333.
- Hoke MM, Timmerman GM and Robbins LK. (2006). Hispanic Health Care International. 4(3), 143-151.
- Erdfelder E, Faul F and Buchner A. (1996). GPOWER: A general power analysis program. Behavior Research Methods, Instruments, & Computers. 28(1), 1-11.
- Magnus M and Enogieru J. (2014). Ethnic Adequacy of Consumer Nutrient Databases. International Journal of Nutrition and Dietetics. 2(2), 115-129.
- Paeratakul S, White MA, Williamson DA, Ryan DH, et al. (2002). Sex, Race/Ethnicity, Socioeconomic Status, and BMI in Relation to Self-Perception of Overweight. Obes Res. 10(5), 345-350.
- Dorsey RR, Eberhardt MS and Ogden CL. (2009). Racial/ Ethnic Differences in Weight Perception. Obesity. 17(4), 790- 795.
- Chang VW and Christakis NA. (2003). Self-perception of weight appropriateness in the United States. Am J Prev Med. 24(4), 332-339.