Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2024
Barriers and Motivations for Obtaining an Anti-Inflammatory Plant-Based Diet in Patients with Crohn’s Disease: A Qualitative Interview Study
Line Birch Arvidsson1, Marie Louise Bergmann1, Mette Holst1,2,*
1Department of Clinical Sciences, Aalborg University, Denmark
2Center for Nutrition and Intestinal Failure, Aalborg University Hospital, Denmark
*Corresponding author: Mette Holst, Professor, PhD, Head of Clinical Nutrition Research, Centre for Nutrition and Intestinal Failure, Department of Gastroenterology, Aalborg University Hospital and Department of Clinical Medicine, Aalborg University, Denmark, Sdr. Skovvej 5.1, 9000 Aalborg, Denmark, Phone: +4527113236, ORCHID: 0000-0002-7458-9458; E-mail: [email protected].
Received Date: January 12, 2023
Published Date: January 25, 2024
Citation: Arvidsson LB, et al. (2024). Barriers and Motivations for Obtaining an Anti-Inflammatory Plant-Based Diet in Patients with Crohn’s Disease: A Qualitative Interview Study. Mathews J Nutr Diet. 7(1):30.
Copyrights: Arvidsson LB, et al. © (2024).
ABSTRACT
Background: Previous research indicated a positive effect of anti-inflammatory, plant-based diets as complementary to treatment in patients with Crohn’s disease, but compliance to dietary changes may be difficult to obtain. Aim: To investigate patients’ motivation and barriers to adhere to a 12-week dietary intervention with an anti-inflammatory plant-based diet. Methods: Semi-structured qualitative interviews with 11 patients with Crohn’s disease in biological therapy. The subjects investigated were “barriers”, “motivation”, and “means of support required for compliance”. Results: Patients’ motivators regarding a lifestyle change with anti-inflammatory and plant-based foods were “Belief in the significance of diet on disease”; “Wish for reduction of medical treatment”; “General health benefits” and “A supportive social network. Barriers were “An unsupportive network”; “Discussions about diet with healthcare professionals were found to be unhelpful”; “Social events” and “Expectation to long for certain foods”. Participants found they would need “Personalized guidance” and “Written information material and recipes” to comply with a plant-based anti-inflammatory diet intervention. Conclusion: Patients diagnosed with Crohn’s disease are primarily positive but need guidance and support from peers and specialists in the lifestyle change towards an anti-inflammatory and plant-based diet. The most significant obstacle was having an un-supporting network and fear of being less social.
Keywords: Patient Preference, Symptom Burden, Inflammatory Bowel Disease, Lifestyle, Nutrition, Complimentary Therapies, Patient Compliance.
INTRODUCTION
Crohn's disease (CD) is an inflammatory bowel disease that causes chronic transmural inflammation in the gastrointestinal tract. It's characterized by a recurrent pattern of relapse and remission, with symptoms such as fatigue, diarrhea, fever, abdominal pain, and anemia [1]. The incidence of CD has been increasing and expanding around the world [2]. CD is a polygenic disorder suggested to be induced by environmental factors including smoking, chronic stress, delivery mode, breastfeeding, medication, and diet. It is acknowledged that the westernization of nourishment low in dietary fiber and high in animal protein may exacerbate the development and is a significant contributor to the increasing incidence of CD, and the gut microbiota [2-7]. Medical treatment aims to reduce disease activity and maintain clinical remission [8], but despite medical advancements including biological agents, achieving long-term remission for CD is challenging [9,10]. It is therefore crucial to identify complementary prevention and treatment strategies. It has been argued that diet might be a contributing factor in the pathogenesis of CD and provide longer remission periods [8]. It is shown that plant foods may reduce inflammation in patients diagnosed with CD and could have a significant influence on the gut microbiota [8,11-14]. A plant-based diet containing various fruits and vegetables is rich in bioactive components such as antioxidants and polyphenols and a diverse array of essential micronutrients, which can have anti-inflammatory properties [8,15]. Additionally, it has been shown that an extensive variety of dietary fibers enhance the structure and function of the gut microbiome [8,16,17]. Thus, there is an indication that diets rich in anti-inflammatory and plant-based foods can be advantageous for individuals with CD, and consequently, it appears pertinent to test the feasibility of a plant-based diet intervention. Studies have shown that patients with Crohns disease (CD) are very eager to engage in physical activity where they can contribute to the effect of treatment by life-style changes [18] or modification. However, complying with a plant-based diet for a longer period of time seems more life changing and may be more challenging than engaging in physical exercise interventions.
Objectives
Accordingly, the aim of the current study was to examine the factors that participants diagnosed with CD perceive as relevant for the initiation and maintenance of lifestyle changes regarding an anti-inflammatory and plant-based diet complementary to medical treatment. The results were intended to be included into strategies to increase the feasibility of dietary change in an upcoming intervention study with a plant-based diet in the particular investigated group of participants.
MATERIAL AND METHODS
The study was designed as a semi structured qualitative interview study.
Setting
Participants were recruited via billboard notices in the treatment room where patients receive biological treatment at department of gastroenterology in a Danish University Hospital and by snowballing. Hereby one patient was recruited via a Facebook group for Crohn’s patients.
Participants
The population included in this study was patients 18 years of age or older, diagnosed with Crohn’s disease for at least six months and threated with biological medicine for at least three months. Furthermore the disease needed to be in remission or with maximum moderate activity according to Crohn's Disease Activity Index [19]. Additionally, patients had to have been diagnosed for at least 6 months ago.
Interviews
For the interviews using a semi-structured interview guide, focused on the participant’s current diet and perceptions of barriers and motivators to changing into an anti-inflammatory plant-based diet, also including the participants perception of what kind of advice and assistance could be needed along the journey. The interview guide was conducted according to Kvale & Brinkmann and thereby contained preliminary questions, exploratory questions and direct questions. To keep the interviews as open as possible, the interviewer strived to give time for the interviewee to reply to the least controlled questions. The interviews were opened by a briefing and ended with a debriefing [20].
Prior to the interviews one pilot interview was conducted with a patient who met the inclusion criteria. As only the order of the questions was slightly changed, this interview was included in the investigation. All interviews were conducted by the same one investigator and took place either in a quite undisturbed room at the outpatient clinic or online through social platforms, as decided by the individual patient. The interviews varied from 38 to 51 minutes excluding briefing and debriefing. The interviews were recorded on a digital recorder, Olympus Voice Recorder WS-811, and afterwards transferred to a computer and encrypted using the software program Encrypto 1.3.3. First, all authors listened through the interviews and took notes of meaning. Then the interviews were all transcribed verbatim.
Analysis
Data were first analyzed using Nvivo 12.2.0. A thematic analysis was conducted to identify themes of meaning across the interviews [20]. All transcribed material was read separately by the first author whom selected and pre-coded quotations of meaning. Subsequently two investigators (first and last author) compared and discussed the codes and agreed on final codes. Patterns across the codes were then collected in sub-themes, and finally main themes were identified based on the sub-themes.
Ethical statement
All participants were given written and oral information prior to giving written informed consent. The study was conducted according to the Helsinki Declaration of 2002, and participants were informed that they could withdraw from the study at any time without any consequences for actual or later treatment or other contacts. The study method is exempt from full application, due to the Danish legislation LBK nr 1083 of 15/09/2017. The analysis and reporting of this study has been done with full respect including all data.
RESULTS
Eleven participants, age 27-64 (mean 42), six females, were included in the interviews. Participants’ experience with Crohn’s varied from 2 to 26 years, mean eight years. In the 11 interviews, three main themes emerged: “Motivation”, “Need for support” and “Barriers”. Four subthemes of barriers were identified as factors that could potentially influence participants’ willingness and ability to adopt a plant-based diet and make lifestyle changes. Themes are shown in figure 1.
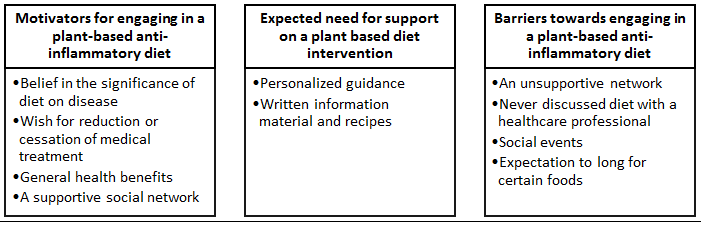
Figure 1. Themes emerged through analysis.
Additionally, strategies have been identified to ensure participant retention in the intervention, as well as potential barriers that could reduce participation. The conclusions on the findings resulted in 3 main themes and 10 sub-themes.
Motivators for engaging in a plant-based anti-inflammatory plant-based diet
Belief in the significance of diet on disease
A significant proportion of participants believed that nutrition could affect their disease. Some patients conducted dietary experiments on their own, while others learned of patients who discontinued medication after modifying their diet. A recurrent motif in the interviews was that patients firmly hold the belief that diet can exert an influence on their disease, and that it can lead to discontinuing medication, lowering the dosage, or mitigating symptoms.
"I believe that there are some things that are more inflammatory than others" (Interview 1)
"I'm very interested in what I can eat and maybe… not get cured, but at least keep it in remission and be comfortable" (Interview 10) The patients express a strong conviction about the impact of nutrition on CD and articulate a belief that certain foods are more inflammatory than others. Furthermore, they have a preconception about the anti-inflammatory and plant-based diet as a diet that can be beneficial towards their disease. Based on the quotes, it can also be interpreted that the patients may have limited knowledge about what this form of diet entails and what foods are suitable, which aligns with the theme of their desire for information before the start of the experiment. One patient discusses plant-based food as a lifestyle change to make in case of flare-ups.
" I'm quite sure that if I get a flare up as bad as I've had it for the last six months. Then I would definitely switch to 99 percent plant food. I will do that. And then stop eating beef. I will try that myself. I want to. Because I have faith that it works. I have that” (Interview 2)
She elucidates that she is of the opinion that a plant-based diet would affect her disease positively in case she experiences flare-ups again, thereby inspiring her to adopt the lifestyle change.
"There are some drug-free people out there who only follow a plant-based diet. But I also think that it helps some people and some it doesn't. But that is also what is so exciting to see. If there is a difference” (Interview 7)
"I have experienced that if I am very, very strict with my diet, I can do well without my medicine" (Interview 3)
The citations above indicate that these patients are entirely convinced that a diet can have a positive impact on CD, and some of them have tried changing their diets themselves and experienced favorable results. However, the quotes also suggest that adhering to such a diet can be challenging, as a patient described it as “strict”.
Overall, this theme reveals that the patients themselves believe that their diet has an impact on their perceived disease. However, it also highlights that adhering to a diet can feel restrictive for them.
Wish for reduction or cessation of biological treatment A considerable number of respondents conveyed a belief or aspiration that the nutritional intervention might play a role in the possibility to reduce or discontinue biological treatment, making stepping down or discontinuing medication a significant incentive for patients with CD in relation to this intervention. “(…) one big thing that would convince me to participate. Of course, if I could stop taking Infliximab. I’ve been taking Infliximab for about 14 years now. So… that’s a long time with a compromised immune system” (interview 5)
Another participant expressed similar sentiments, stating willingness to do whatever it takes to recover from illness and stop taking medication.
“I will do whatever it takes for me to recover from illness so that I can get off medication. For me, it’s important to get off medication” (interview 1)
This highlights the importance of discontinuing medication for patients and their belief that they themselves can take action to improve their condition and reduce their reliance on medication and thus hospital connection.
Health benefits "Health benefits" emerged as a significant motivator for patients with CD to make lifestyle changes. Several interviewees identified the potential health benefits of plant foods as a key motivator for their participation in a research study or lifestyle change, believing that this change could enhance their overall health.
"It's improving health, that’s for sure. You know… health in general (...)” (interview 3)
Another participant expressed that she would be motivated to participate if she believed that it could have a positive effect on her psychical health, particularly in relation to CD and Attention deficit hyperactivity disorder (ADHD).
“What could be motivating for me was if there was something to gain in relation to my physical health. I think… in relation to my Crohn disease or to my ADHD. That there is a health benefit jumping into this and that I can see that there is some data” (interview 4)
Additionally, it was noted that this participant would be further motivated if data supported her own positive experiences with the lifestyle change. These findings suggest that the potential health benefits of a dietary intervention may be an important factor in motivating patients with CD to make this change.
A supportive social network The interviews revealed that the participants attach significance to the role of family and friends in their capacity to sustain a lifestyle change. The participants accord high value to having a supportive network of friends and family who endorse the intervention, as it aids them in staying motivated and optimistic towards the intervention.
“My husband also talked about, that he might like to... So, he doesn't want to completely, but that he might agree to it, and then it might be that they (the family) cook some meat on the side. And I told my sister, and she said that she was in on it too. So, it's cool to have such support, where I think, well, we could also. when we're together like that, that's what we're thinking about too. So, I think that in that way we are also in a... Also, my older sister and things like that, we are in a period where we are very concerned about that” (interview 3)
The participants highly value the willingness of their families to partake in the intervention by consuming the same food as the participants. This would give them a sense of support and would also reduce the intricacy of the treatment. The participants hold the belief that family support could serve as a facilitator that would augment their motivation to comply with this complementary treatment intervention. One of the rationales for the importance of family support to patients is due to logistical reasons. If the entire family is committed to consuming the same food as the participants, it would be much more convenient to participate in this intervention. This is because the family would not have to prepare multiple dishes simultaneously, and the participants would feel more supported and encouraged.
Expected need for support on a plant-based diet interventions
Written information material and recipes
Another factor investigated in this study was the requirements for a successful implementation of the intervention. One of the facilitators identified by the patients was the provision of shopping lists.
“Having lists that can tell me what to buy… Yes, that would be a good thing.” (Interview 6)
The citation indicates the necessity of shopping lists as a form of guidance. The citation below supports the need to have shopping lists as guidance and additionally, the interviewee explains that having recipes would make it easier to implement the lifestyle change in their everyday life.
“(…) I think recipes and shopping lists. Because you don't know what you can get. You don't necessarily know what exists. And stuff like that. So, I think that is also a good idea" (Interview 8)
This clarifies the importance of providing written information materials to participants due to their lack of knowledge and experience with anti-inflammatory and plant-based diets.
Overall, the participants demonstrate a lack of knowledge regarding the diet, emphasizing the importance of providing detailed and feasible information. It is therefore necessary to ensure that the patients learn everything from the beginning and are well-informed, which includes providing materials such as shopping lists and recipes.
"(…) help with recipes - suggestions for what to do. I could borrow a vegetarian cookbook from the library, but it's just the impracticalities of getting it done, buy it and prepare the food. That's where it sometimes gets stuck. In other words, a bit like a meal plan. So that you can be prepared and buy the ingredients all at the same time” (Interview 10)
The participants express a desire for not only recipes, but also inspiration for meals throughout the day.
"Well, at least I should have some guidance. Someone must tell me about it. And give me some ideas for what I could do. In other words, on a day, not only what you can have for dinner, but also what you must have for breakfast and lunch. At least someone should introduce me to it, I think. I read a bit about it myself and I researched, but then cookbooks cost money, and that kind of thing. And then I don't bother (laughs)” (Interview 7)
The interviewee emphasizes the importance of guidance, and the citation highlights a concern from the patient after researching the area; it has been challenging to find relevant material. This knowledge is significant for the intervention as it may be necessary to provide participants with guidance, inspiration for meals, and resources such as food blogs to seek additional information and inspiration for anti-inflammatory cooking.
This theme demonstrates that introducing shopping lists, recipes, guidance, and cooking courses may contribute to a better implementation of the dietary changes.
Barriers towards engaging in a plant-based anti-inflammatory diet
This main theme covers the findings that may have a negative impact on patients’ compliance regarding the intervention. These findings are important to be aware of in the context of a research study, as they may have a negative impact on participants' persistence and attitude.
An unsupportive network As previously described, a supportive network can act as a facilitator, but it was also found that a lack of support can have a negative effect and thus act as a barrier to the intervention. The family can be perceived as a barrier regarding the intervention if they are unwilling to adopt the anti-inflammatory and plant-based diet, as this can pose a challenge to maintaining motivation and lead to patients feeling like a burden. Additionally, if the family must prepare multiple dishes for every meal due to varying preferences, it can become a time-consuming task.
"(…) then it would mean that I would have to prepare something different for myself and something else for the rest of the family for every meal. So that would be a bit of a hassle…”
Interviewer: “Your family wouldn't be joining you in this, or?”
“Not if it involves smoothies and such, no. They would eat some, but they certainly wouldn't want to switch to a completely plant-based diet” (Interview 5)
Although a considerable number of interviewees are confident that their families would endorse the lifestyle modification and possibly adopt the same dietary habits as the participants, not all interviewees share this conviction, which could impede their sustained involvement in the intervention. Furthermore, the existence of non-compliant foods, such as meat and dairy products, in the household could provoke temptation for the participants, thereby constituting another potential obstacle to the intervention.
“What could also be difficult is if my boyfriend is sitting there eating one delicious burger after another, and I have to eat something different. So, it would be nice if he wanted to be a part of the project also, maybe” (Interview 7)
One patient however experience that her husband does not believe that the diet can have a beneficial effect.
"My husband, for example, thinks it's nonsense. He doesn't think you can eat your way out of it. And my surgical colleagues, doctors, don't believe it, and the medical gastroenterologists don't really believe it either" (Interview 1)
It is suggested that it is crucial for the participants that their immediate surroundings are either actively engaged in the project or, at the very least, supportive of it. This is because it can be less arduous if family and friends are involved, and participants are not enticed by specific kinds of food. Furthermore, it can foster a sense of recognition and encouragement for the patients' endeavors.
Discussions about diet with healthcare professionals were found to be unhelpful
It became clear throughout the interviews that many patients never discussed nutrition with healthcare professionals in relation to their disease. When one of the interviewees asked about diet, she received this answer:
"Well, you just have to think a little about the diet. Eat healthy. Yes, you just must eat healthy food. Eat lots of greens and you'll be fine”. “Okay. But vegetables aren't just vegetables, are they? Soo..."(Interview 4)
The patient is experiencing a lack of help or information regarding diet and is somewhat frustrated by it. This experience of not receiving help or feeling alone regarding dietary questions is echoed in the interviews, with many participants stating that they have neither spoken to a dietitian, or another specialist nor been referred to one.
“I mean... I haven’t actually sat down with a nutritionist or anything. But they have noticed that my B12 and iron levels are low, and you know. Made plans to address it. But I'm not in danger of being underweight like many Crohn's patients are, so there hasn’t been a pressing need to... you know...” (Interview 5)
Another patient has experienced some guidance regarding the diet but has also noted a lack of research in the field. As a result, the advice he received conflicted with other sources and he finds that there has been a considerable amount of “pseudoscience” around the topic.
“When I was diagnosed, the recommended way to control my condition was to consume no more than 40 grams of fat. However, there has been a lot of conflicting advice on what to do and what not to do. There is also a lack of research on the subject. While there is plenty of anecdotal evidence from people sharing their experiences, I have been missing solid guidance” (Interview 8)
The interviewee explains that he lacked solid, scientifically documented knowledge to relate to in connection with his disease and diet.
Based on the interviews, patients have not received the dietary treatment or guidance that they have felt the need for. This may be due to it being deprioritized, but also because there has not been much scientific documentation in the field, as explained by one patient.
Although patients have not received much guidance regarding nutrition, they have nonetheless perceived that healthcare professionals hold opinions or biases regarding the importance and effects of diet on their disease. Many patients report that their doctors have told them that they do not believe that an anti-inflammatory diet can have an impact on the disease.
"I have asked several times if I could I do something myself. And then I have been told by the doctors that they do not believe in eating an anti-inflammatory diet, but I could try. The only thing they told me to keep in mind was to eat lactose-free. So, I drink lactose-free milk” (Interview 1)
"If the patients ask, many of the doctors say:” Well, it doesn't matter" (Interview 3)
One participant attempted to seek feedback from the nurses regarding nutrition, but experienced skepticism about plant-based diets based on bad experiences from other patients. Additionally, he/she felt, that the nurses generally do not have the resources or interest to seek out information about a plant-based diet.
“(…) I got the answer (in the bed ward) that the patients the nurse has met, who have changed their diet come in with deficiency states. The nurses have neither the time, knowledge nor interest. I have searched and asked but have not received an answer. Have stated to the nurse that you do not get guidance on diet and your entire lifestyle and relationships. Got the answer that they have neither time nor money" (Interview 10)
It appears challenging to seek advice from healthcare professionals as they lack knowledge and are not interested in nutrition and its relevance to their patients. Nevertheless, healthcare professionals are not the only ones who are skeptical about dietary changes for patients with CD.
Furthermore, the quote supports the patients' experience that healthcare professionals are not a particularly great support for patients when it comes to nutritional therapy and advice regarding diet. This might suggest that patients themselves may encounter resistance, lack of knowledge, and insufficient support from their surroundings when attempting to make changes to their diet.
Social events Another significant finding was that social settings such as restaurant visits, travel, parties, vacations, and work could act as barriers to maintaining motivation and adherence to the intervention.
"There are some rituals that will be difficult to shelve, right? For example, for the next four days, to go out with friends to restaurants in the evening, and then sit and drink water and eat beans..." (Interview 2)
The interviewee expresses skepticism towards the diet and has preconceived notions about what is allowed to eat and what is not in the intervention. Additionally, besides the social arguments, the person's prejudices about the diet also appear to be a barrier towards the patient, which could suggest low motivation for participation. Another patient perceives the diet as problematic because the majority of people around them eat differently.
“My problem is whether I can be persistent. Because I really think it could.. So.. it's difficult. Because when the majority of people eat something else, I think it's difficult to have to... In other words, eat something completely different from them. Also, at work. But I think it's very exciting. So, if I lived alone for three months and didn't have to see any people - then I would easily be able to handle it. I kind of think it's those who are around you. But if I locked myself in a room for three months, it might well be” (Interview 7)
The interviewee's comments indicate the significant importance of the social setting and the value they attach to the meal community. While the person expresses excitement about the project, eating a different diet than people in their environment will be a significant barrier.
"No, that's what I think too, so you have to take something (food) of your own with you. But these are also some of the things you look forward to when you go to events like a graduation party. That there is good food. So, I think it's a bit difficult. It might be possible. Yes. But it is difficult. And I think that's also why there are many who don't do it" (Interview 7)
The interviewee anticipates that it will not be possible to participate in social gatherings and obtain food if they are not eating in the usual way. Additionally, it appears that the interviewee will have to compromise since she looks forward to the food that will be served at parties.
Expectation to long for certain foods Another discovery that has been revealed as a barrier is that several participants are unequivocally convinced that they will experience a sense of longing for some of the foods they are accustomed to consuming.
"Then I also think that if you have to cut out eggs and dairy products, then... I think that would be difficult. It's not because... I don't drink milk, but I mean, for example, I like cheese and yogurt, you know" (Interview 8)
The informant expresses that it will be difficult to abstain from specific comestibles, and in the following quote, the informant continues to explain that they will resent being unable to consume meat or chicken during the intervention.
"Even though I would hate not being able to eat a good steak or a delicious piece of chicken or something, I also know that it would probably do something really good for my overall sense of health. I think so" (Interview 8)
Thus, although it will be challenging to abstain from certain comestibles, the interviewee also recognizes some benefits of this project, which may outweigh the loss of familiar foods. Therefore, emphasis on the positive aspects of the research project may be necessary to motivate participation throughout the project period. Another participant also expresses that it may be difficult to limit food intake to certain food groups.
Interviewer: “What do you think would be the most difficult?”
Interviewee: “Hmm, something like, what’s it called… When you crave something delicious. And you can’t just take it. I think. Candy and alle these things. I mean, just going to the fridge and taking something” (Interview 7)
The interviewee envisions that they won't be able to easily grab something tasty from the fridge, and they will miss eating candy. Even though participants will miss certain comestibles, it is also expressed that they do not wish to consume substitute products.
"I know that there are plant-based alternatives, but it just doesn't taste the same. I feel that plant-based alternatives that try to imitate something they're not rarely work very well. So, if you're going to eat plant-based, you shouldn't eat plant-based versions of meat or cheese. Because it doesn't make sense. Not to me" (Interview 8)
Here, the interviewee expresses an opinion that substitute products cannot replace either meat or dairy products. This knowledge is essential as it provides insight that it will not have a positive effect on patients' mindset to consume products that resemble something they are not.
DISCUSSION
Studies show that it could be challenging to adopt health goals, despite most people desiring to lead healthy lifestyles. If individuals are not focused on the consequences of their lifestyle or do not feel vulnerable, they may be less willing to change their habits [21].
In the context of the research project involving a nutrition intervention for patients with CD, this can possibly affect patient compliance. Patients who feel that their disease is relatively under control and who generally feel well may be less motivated than those who experience discomfort and several flare-ups. As the planned intervention targets patients in remission or moderate disease at the most, it may be relevant to be aware of the fact that some patients may feel physically well despite their disease and, therefore, have lower motivation.
The abundance of conflicting health information is another factor that could potentially hinder people from adopting a lifestyle intervention. Mann et al., 2013 suggest that the abundance of conflicting health information can be overwhelming for individuals and can serve as a barrier to their lifestyle change and that most patients with CD base their diet and lifestyle on self-experience and give up many foods [22]. This finding is important to be aware of and possibly communicate to the participants, so they do not lose motivation or come across unverified and pseudoscientific evidence, which could potentially be harmful.
Another factor that is relevant to behavioral changes within psychology is that individuals do not engage in lifestyle changes that they cannot identify with [21].This research is essential to consider in relation to recruiting participants for a research project concerning a nutrition intervention, as it indicates that participants must be able to identify with the intervention and be positively inclined towards the change it requires to participate. Therefore, it seems important to recruit patients who have a genuine desire to participate if the intended effects are to be achieved and to minimize dropout rates.
Strengths and limitations of the study
In this study we interviewed 11 participants about their individual perceptions. These cannot and are not intended to be generalizable in all CD patients or their experiences. Furthermore, all participants are patients in almost remission by biological therapy, in a well-developed country with plenty of access to healthcare, medication and food. This it is not generalizable to all countries.
CONCLUSIONS
This study has identified findings that can be utilized in the implementation of an anti-inflammatory plant-based intervention as complementary to medical treatment for patients with chronic inflammatory bowel disease. The study has identified both barriers and facilitators that can impact patients' attitudes and adherence to a complementary treatment intervention.
It seems important to deal with and handle these barriers and facilitators to the highest possible extent, in order to carry out an intervention successfully with the best compliance. Research shall reveal the influence on implementation of these findings.
ACKNOWLEDGEMENTS
The authors thank participants for their willingness to share perceptions and the healthcare staff at department of gastroenterology for helping with access to participants.
DECLARATIONS OF INTEREST
None.
DATA AVAILABILITY STATEMENT
The transcribed data that support the findings of this study will be made available on request. Data are in Danish language. Voice recordings are not available due to ethical restrictions.
FUNDING STATEMENT
Funding for salary to the PhD student / research assistant in this study was provided by the Aage and Johanne Louis-Hansen Foundation J.nr. 20-2B-7892.
ETHICS APPROVAL STATEMENT
The study was conducted according to the Helsinki Declaration of 2002, and participants were informed that they could withdraw from the study at any time without any consequences for actual or later treatment or other contacts. The study method is exempt from full application, due to the Danish legislation LBK nr 1083 of 15/09/2017. The analysis and reporting of this study has been done with full respect including all data.
PATIENT CONSENT STATEMENT
All participants were given written and oral information prior to giving written informed consent.
AUTHOR STATEMENT
MB: Design and data collection, revision. LA: Transcription, formal analysis, and writing- original draft, revision. MH: Conceptualization, design, methodology, project administration, transcription, secondary analysis, writing-and editing. All authors agreed on the final edition of the manuscript.
REFERENCES
- Gajendran M, Loganathan P, Catinella AP, Hashash JG. (2018). A comprehensive review and update on Crohn’s disease. Disease-a-Month. 64(2):20-57.
- Chiba M, Morita N. (2023). Incorporation of Plant-Based Diet Surpasses Current Standards in Therapeutic Outcomes in Inflammatory Bowel Disease. Metabolites. 13(3):332.
- Ananthakrishnan AN, Bernstein CN, Iliopoulos D, Macpherson A, Neurath MF, Ali RAR, et al. (2018). Environmental triggers in IBD: A review of progress and evidence. Nat Rev Gastroenterol Hepatol. 15(1):39-49.
- David LA, Maurice CF, Carmody RN, Gootenberg DB, Button JE, Wolfe BE, et al. (2014). gut microbiome. Nature. 505(7484):559-563.
- Levy M, Kolodziejczyk AA, Thaiss CA, Elinav E. (2017). Dysbiosis and the immune system. Nat Publ Gr. 17(4):219-232.
- Mueller NT, Bakacs E, Combellick J, Grigoryan Z, Dominguez-Bello MG. (2015). The infant microbiome development: Mom matters. Trends Mol Med. 21(2):109-117.
- Singh RK, Chang HW, Yan D, Lee KM, Ucmak D, Wong K, et al. (2017). Influence of diet on the gut microbiome and implications for human health. J Transl Med. 15(1):73.
- Antoniussen CS, Rasmussen HH, Holst M, Lauridsen C. (2021). Reducing Disease Activity of Inflammatory Bowel Disease by Consumption of Plant-Based Foods and Nutrients. Front Nutr. 8:733433.
- Vester-Andersen MK, Vind I, Prosberg MV, Bengtsson BG, Blixt T, Munkholm P, et al. (2014). Hospitalisation, surgical and medical recurrence rates in inflammatory bowel disease 2003-2011-A Danish population-based cohort study. J Crohn’s Colitis. 8(12):1675-1683.
- Hilligsøe M, Eriksen ND, Jacobsen MH, Kaagaard LH, Vinter-Jensen L, Rasmussen HH, et al. (2018). Is body composition related to efficacy of biological treatment with TNF-Α inhibitors in patients with crohn’s disease? Clin Nutr. 37(1):S234.
- Haghighatdoost F, Bellissimo N, Totosy De Zepetnek JO, Rouhani MH. (2017). Association of vegetarian diet with inflammatory biomarkers: A systematic review and meta-analysis of observational studies. Public Health Nutr. 20(15):2713-2721.
- Holt EM, Steffen LM, Moran A, Basu S, Steinberger J, Ross JA, et al. (2009). Fruit and Vegetable Consumption and Its Relation to Markers of Inflammation and Oxidative Stress in Adolescents. J Am Diet Assoc. 109(3):414-421.
- Ock KC, Chung SJ, Claycombe KJ, Song WO. (2008). Serum C-reactive protein concentrations are inversely associated with dietary flavonoid intake in U.S. adults. J Nutr. 138(4):753-760.
- Saraf-Bank S, Esmaillzadeh A, Faghihimani E, Azadbakht L. (2015). Effect of non-soy legume consumption on inflammation and serum adiponectin levels among first-degree relatives of patients with diabetes: A randomized, crossover study. Nutrition. 31(3):459-465.
- Stromsnes K, Correas AG, Lehmann J, Gambini J, Olaso‐gonzalez G. (2021). Anti‐inflammatory properties of diet: Role in healthy aging. Biomedicines. 9(8):1-28.
- Grosse CSJ, Christophersen CT, Devine A, Lawrance IC. (2020). The role of a plant-based diet in the pathogenesis, etiology and management of the inflammatory bowel diseases. Expert Rev Gastroenterol Hepatol. 14(3):137-145.
- Lo CH, Lochhead P, Khalili H, Song M, Tabung FK, Burke KE, et al. (2020). Dietary Inflammatory Potential and Risk of Crohn’s Disease and Ulcerative Colitis. Gastroenterology. 159(3):873-883.e1.
- Geisler L, Ubbesen N, Søndergaard J, Jørgensen LQ, Sam T, Christensen T, et al. (2020). Clinics in Gastroenterology Eight-Weeks Individualized Exercise Program Targeted for Patients with Crohn ’ s Disease : A Feasibility Study. Clin Gastroenterol. 2(1):17-21.
- Best WR, Becktel JM, Singleton JW, Kern F. (1976). Development of a Crohn’s Disease Activity Index. Gastroenterology. 70(3):439-444.
- Kvale S, Brinkmann S. (2015). Interview. In: 3rd edn. København, Denmark: Hans Reitzels Forlag. p. 440.
- Mann T, De Ridder D, Fujita K. (2013). Self-regulation of health behavior: Social psychological approaches to goal setting and goal striving. Heal Psychol. 32(5):487-498.
- Guida L, Di Giorgio FM, Busacca A, Carrozza L, Ciminnisi S, Almasio PL, et al. (2021). Perception of the Role of Food and Dietary Modifications in Patients with Inflammatory Bowel Disease: Impact on Lifestyle. Nutrients. 13(3):759.