Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2022
Vascular Lesions Treated with Laser
Aristides Arellano-Huacuja*, Dafne Arellano-Montalvo, Anja Arellano-Montalvo
Dermatological Clinic and Aesthetic Surgery of Puebla, Puebla, Mexico
*Corresponding author: Dr. Aristides Arellano-Huacuja, MD, FICS, Dermatological Clinic and Aesthetic Surgery of Puebla, Puebla, Mexico. Tel: (222)437740, Fax: (222)2377494; Email: [email protected]
Received Date: November 16, 2022
Published Date: December 15, 2022
Citation: Arellano-Huacuja A, et al. (2022). Vascular Lesions Treated with Laser. Mathews J Dermatol. 6(1):16.
Copyrights: Arellano-Huacuja A, et al. © (2022).
ABSTRACT
In 1999, we start working on the treatment of the vascular lesion. This phatology is present in the face and legs and we perform the procedure on skin types III to V mostly. With the Neodynium vascular laser source, the obtained results seem to be good even in reticular veins, telangiectasias, and small capillaries. In Hemangiomas and Nevus Flammeus we have seen excellent results.
Keywords: vascular lesions, laser treatment, aesthetic surgery, dermatology
INTRODUCTION
Over the years, various laser light systems have been used in the treatment of vascular lesions. The laser is a device that is made up of active media, whether gaseous, liquid, or solid, enclosed within a resonant cavity, limited by a pair of parallel flat mirrors, some perfectly specular and others semi-transparent [1].
Einstein was the one who for the first time suggested the bases on the controlled manipulation of light waves in the year 1917, it was not until 1960 when the first laser (Light amplification by stimulated emission of radiation) was built, and one of its main applications was in the treatment of cutaneous vascular lesions. Giving rise to the argon laser, created in 1960 by Maiman, being a continuous emission laser, with wavelengths between 488 and 514 nm [2,3].
Later, in the mid-1990s, an Intense Pulsed Light source (IPLS) was used, which uses a high-energy flashlamp system with a spectrum of variable wavelengths, ranging from 515 to 1200nm [4,5].
The most recent laser used in the treatment of blood vessels is the pulsed Nd: Yag of 1,064 nm, which emits energy up to 150j/cm2. This system is based on the deep penetration of these wavelengths to photocoagulate larger caliber vessels (especially in the lower extremities); such as reticular varicose veins, essential and secondary telangiectasias, thus replacing sclerotherapy. The laser light is selectively absorbed by the chromophore (hemoglobin) generating heat, raising the temperature above the coagulation point, causing the reabsorption of all the vascular walls [6,7].
As expected, the pathologies that involve the different kinds of veins are conditioned by the location and function of each one of them, the network of deep veins, by controlling a high percentage of blood return (approximately 80%), is associated commonly with pictures of venous insufficiency. The perforating veins sometimes suffer injuries to their valvular structures, losing the unidirectional character of their flow, so that the blood coming from the deep system refluxes towards the superficial veins, dilating them and making them varicose [8,9].
As is well known, the prevalence of venous disease in our environment is extraordinarily high. A variety of factors contribute to this, not only congenital but also acquired, such as multiple pregnancies, trauma, prolonged standing, etc. From this point of view, the conditions included in this category, like many others, show a strong participation of educational and cultural factors.
Dilated and tortuous superficial veins with incompetent valves. They are usually a problem involving the great and great saphenous veins. The highest incidence occurs after the age of 20, three times more frequent in women than in men due to the intervention of predisposing factors such as pregnancy and menopause and heredity. As well as sequelae of deep thrombophlebitis with venous recanalization [10,11].
Goal
Evaluate the results obtained with Intense Pulsed Light and Neodymium: Yag Laser in the treatment of venous insufficiency of the lower limbs as well as facial hemangiomas.
MATERIAL AND METHOD
Between October 1998 and August 2020, 5,309 patients with venous insufficiency of the lower limbs were treated, all women aged between 26 and 45 years, with the IPL with Fitzpatrick III to V phototypes, using the following filters 550 and 570, Later, in August 1999 and September 2002, the treatment with the Neodymium Laser was continued: Yag pulsed, having a female population of (90.00%) and (10.00%) males aged between 20 and 70 years [12,13].
All cases presented spider veins, telangiectasias, reticular veins and some with tortuous veins. The parameters we used for telangiectasias were low powers, for reticular we used 110jcm2 at a single pulse with a delay of 12 ms and for veins larger than 6 mm we used 120 jcm2 double pulses and a delay of 7 ms [14,15].
RESULTS
With Intense Pulsed Light we only obtained good results in telangiectasias, however, with the Neodymium Laser: Pulsed Yag the clinical improvement presented by patients with venous insufficiency has been 80% to 85% on average, we have only had two cases of abandonment of treatment, due to presenting pain when performing it (Table 1).
Table 1. Percentage of vein clearance after treatment.
|
Type of lesion |
# patients |
% clearance |
|
Reticular veins |
4235 |
90 |
|
Telangiectasias |
1074 |
85 |
The post-treatment complications that have occurred to us are hyperpigmentation, which has resolved spontaneously and without sequelae, and hypopigmentation, which has subsided with the application of Puva therapy and exposure to the sun in a period of approximately 6 months [16-18].
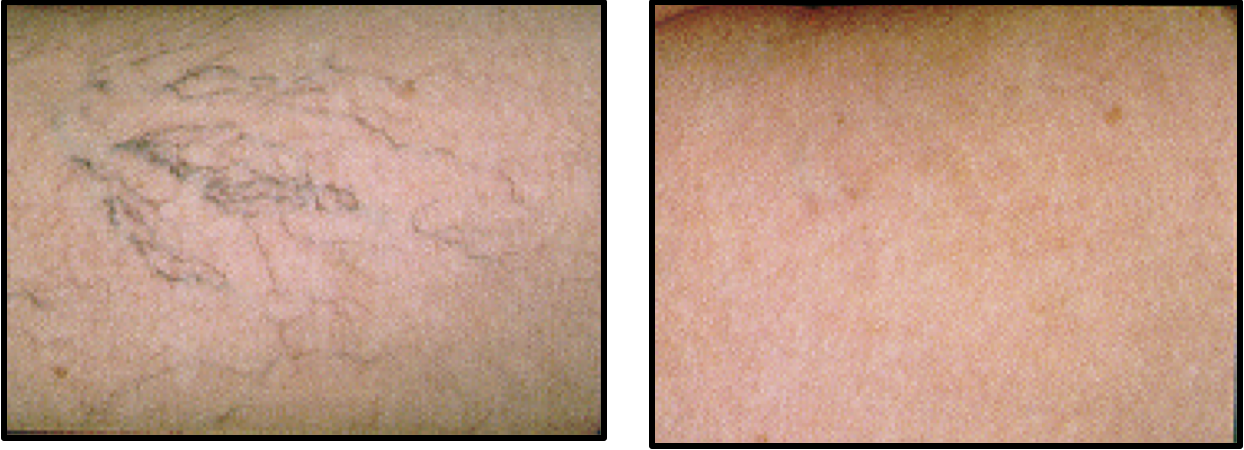
31 female patients. Leg spiders. 3 sessions IPL filter 570 nm 35 -50 j/cm T1 3.5 - D1 40 – T2 3.5. Skin type III
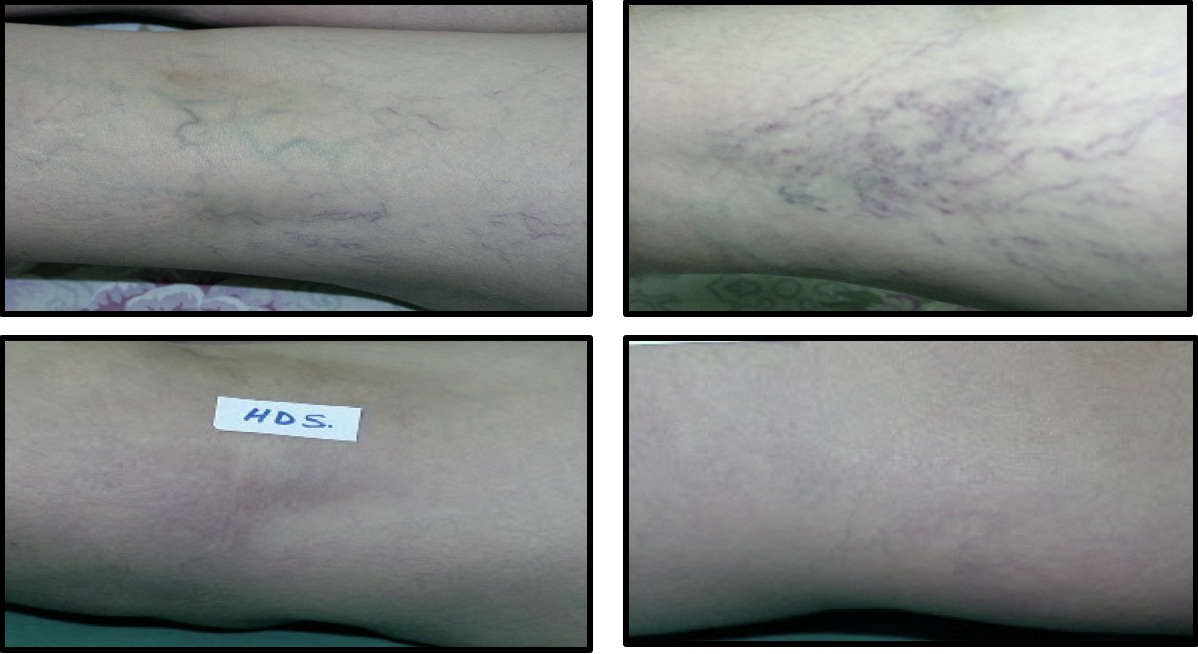
56 years old woman with reticular veins and telangiectasias. Skin type III. DL 1064 nm. 6 sessions 110 j/cm2 double pulse T1 15 D1 30 T2 15

44 years old woman with telangiectasias. Skin type III. 4 sessions DL 1064 nm 110 – 115 j/cm2 T1 12 1 pulse

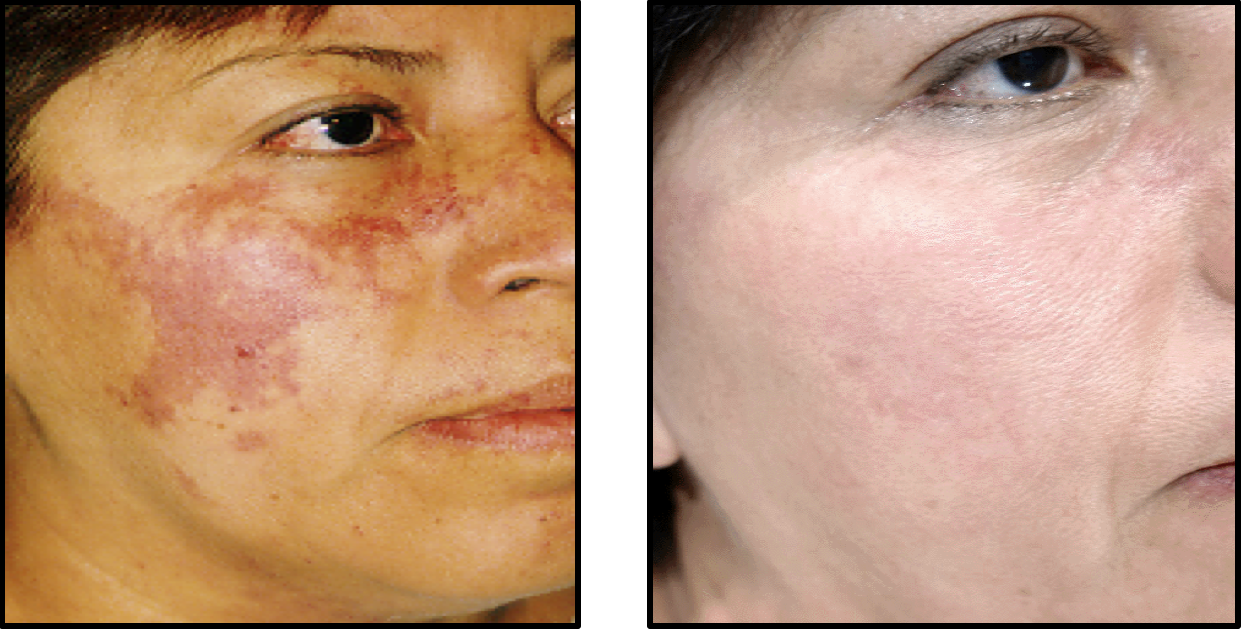
45 female patients. Port wine stain. Skin type IV 10 sessions IPL/VL filter 570-590 nm 36 –55 j/cm T1 3.0 D1 20 T2 3.0 DL 6 sessions 1064 nm 100 – 130 j/cm T1 16
45 female patients. Port wine stain. Skin type IV 10 sessions IPL/VL filter 570-590 nm 36 –55 j/cm T1 3.0 D1 20 T2 3.0 DL 6 sessions 1064 nm 100 – 130 j/cm T1 16
CONCLUSIONS
The therapy used for the treatment of venous insufficiency of the lower limbs with the Neodymium Laser is an outpatient treatment that does not need rest, just take care of the sun so as not to tan and be able to carry out the treatment, the improvement obtained in the first session has been 30% on average and in the third session 70% improving the symptoms presented in the first sessions such as pain, foot edema, numbness, and temperature changes.
REFERENCES
- Kienie A, Hibst R. (1997). Optical parameters for laser treatment of leg telangiectasias. Laser Med Surg. 20(3):346-353.
- Goldman MP, Eckhouse S. (1996). Photo thermal sclerosis of leg veins. Dermatol Surg. 22(4):323-330.
- Sonden A, Swenson B, Raoman N, et al. (2000). Laser induced shock wave endothelial cell injury. Laser Med Surg. 26(4):364-375.
- Dover JS, Sadick NS, Goodman MP. (1999). The role of laser and light sources in the treatment of the veins. Dermatol Surg. 25(4):328-335.
- Reisfeld PL. (2000). Blue in the skin. J Am Acad Dermatol. 42(4):597-605.
- Adrian RM. (1998). Treatment of leg telangiectasias using a long-pulse frequency-doubled neodymium: YAG laser at 532 nm. Dermatol Surg. 24(1):19-23.
- Bernstein EL, Kornbluth S. Brown DB, Black J. (1999). Treatment of spider veins using a 10-millisecond pulse duration frequency-doubled neodymium YAG laser. Dermatol Surg. 25(4):316-320.
- Massey RA, Katz BE. (1999). Successful treatment of spider leg veins with a high-energy long pulse frequency doubled neodymium: YAG laser (HELPG). Dermatol Surg. 25(9):677-680.
- Cisneros JL, Del Rio R, Palou J. (1998). Sclerosis, and the Nd: YAG Q-switched laser with multiples frequency of telangiectasias, reticular veins and residual pigmentation. Dermatol Surg. 24(10):1119-1123.
- Goldman MD, Fitzpatrick RE. (1990). Pulse-dye laser treatment of leg telangiectasias with and without simultaneous sclerotherapy. J Dermatol Surg Oncol. 16(4):338-344.
- West TB, Sister TS. (1998). Comparison of the long pulse dye (5590-595nm) and KTP (532 nm) laser in the treatment of facial and leg telangiectasias. Dermatol Surg. 24(2):221-226.
- Hohenleutner V, Walther T, Wenig M, Baumier W, Landthaler M. (1998). Leg telangiectasias treatment with a 1.5 ms pulse dye laser, ice cube cooling of the skin 595vs. 600 nm–preliminary results. Lasers Med Surg. 23(2):72-78.
- Bernstein EF, Lee J, Lowery J, et al. (1998). Treatment of spider veins with the 595nm pulsed dye laser. J Am Acad Dermatol. 39(5 Pt 1):746-750.
- Alora MB, Stern RS, Arnot KA, Dover JS. (1999). Comparison of 595 nm long pulse (1-5 msec) and ultra-long pulse (4 msec) lasers in the treatment of leg veins. Dermatol Surg. 25(6):445-449.
- Reichert D. (1998). Evaluation of the long pulse dye lasers for the treatment of leg telangiectasias. Dermatol Surg. 24(7):737-740.
- Hsia J, Lowery JA, Zelickson B. (1997). Treatment of leg telangiectasias using a long-pulse dye laser at 595 nm. Lasers Med Surg. 20(1):1-5.
- Goodman MA, Martin DE, Fitzpatrick RE, Ruiz-Esparza J. (1990). Pulse dye laser treatment of telangiectasias with and without sub therapeutic sclerotherapy. J Dermatol Surg Oncol. 16(4):338-344.
- Green D. (1998). Photo thermal removal of telangiectasias of the lower extremities with Photoderm VL Flash lamp as a new treatment possibility for vascular skin lesions. Dermatol Surg. 24:743-748.