Previous Issues Volume 4, Issue 1 - 2019
Splenogonadal Discontinuous Fusion as a Transoperative Finding in Inguinal Hernia Surgery in children (Granado´s Hernia). Clinical case
Francisco José Granados Navas1, Michelle Castro2, Guillermo Padrón Arredondo3
1 Pediatric surgeon, Department Pediatric Surgery of General Hospital Playa del Carmen, Q. Roo. México.
2 Pathologist, Department Pediatric Surgery of General Hospital Playa del Carmen, Q. Roo. México.
3 General surgeon, Department Pediatric Surgery of General Hospital Playa del Carmen, Q. Roo. México.
Corresponding Author: Francisco José Granados Navas, Pediatric surgeon, Department Pediatric Surgery of General Hospital Playa del Carmen, Q. Roo. México. CP. 77732
Received Date: Feb 25, 2019 Published Date: May 10, 2019
Copyright © Granados Navas FJ
Citation: Granados Navas FJ. (2019) Splenogonadal Discontinuous Fusion as a Transoperative Finding in Inguinal Hernia Surgery in children (Granado´s Hernia). Clinical case. Mathews J Case Rep 4 (1): 44.
ABSTRACT
Introduction: The first references about splenogonadal fusion were described by Boestrom in 1883 and Pomer in 1889. Its incidence is unknown but it is considered according to Montes and Prada in about 160 reported cases.
Clinical case: A 3-year-old boy with no perinatal history of importance and who consults for volume increase in the left inguinal region. Physical examination shows a visible mass, not painful on palpation, soft, not attached to deep planes with reduced hernial content. The clinical diagnosis of left inguinal hernia is established and scheduled for surgery. The histopathological report explains in the macroscopic description a vermiform tubular tissue of 7 cm in length and thickness of 1.3 cm of rubberized consistency compatible with splenic ectopic tissue.
Discussion: Has been reported a case in a 6-year-old boy who presented clinically as a strangulated left inguinal hernia and this case was a continuous splenogonadal fusion, but our case was a discontinuous splenogondal fusion. Our case is the first one reported in a child with a palpable mass in the inguinal region, similar to an inguinal hernia that can be reduced with inguinal plasty with a biopsy that reported splenic tissue. It is suggested that it be called Hernia de Granados.
KEYWORDS: Discontinuous Splenogonadal Fusion; Spleen; Ectopic Tissue; Child; Inguinal Hernia.
INTRODUCTION
The first references about splenogonadal fusion were described by Boestrom in 1883[1] and Pomer in 1889[2]. Its incidence is unknown but it is considered according to Montes[3] and Prada[4] in about 160 reported cases. Putschar and Manion[5] were the first differences in the continuous forms of the discontinuous forms of the condition. Petrick[6] in 1988 reported the largest series of this pathology with 87cases. Although it can appear in both sexes, it is much more frequent in men (ratio of 9: 1 or 15: 1, according to the consulted reference); clinically manifests as testicular or pratestic tumor being diagnosed during cryptorchidism or a hernia surgery inguinal as was our case. In the Carragher study[7] of 123 cases reported 71 (56%) corresponded to continuous splenogonadal fusion and 52 cases (44%) of discontinuous splenogonadal fusion.
Its presentation ranges from birth to 82 years of age, with the male sex and the left side predominating with a ratio of 18:1. His etiopathogenesis is unknown and lies in the proximity of both the splenic and gonadal tissues as well as the mesonephric duct during gestational development, making reference to the moment of rotation of the embryonic gastrointestinal structures (primitive stomach), and the mesogastric structures bringing the spleen to a left lateral position, maintaining an almost direct relationship with the ipsilateral kidney and the developing gonadal crest, remaining intimately united until week 8 and it is believed that it is here where splenogonadal fusion occurs[8].in 71 eases or 56 percent.
CLINICAL CASE
A 3-year-old male with no perinatal history of importance for the current condition and who consults for volume increase in the left inguinal region. Upon interrogation, the mother reports that from birth she presents this mass in the inguinal region and had been diagnosed as an inguinal hernia. Three months before consulting, there was an increase in volume, pain and color change, so he consulted the emergency department, which valued it and referred to it as a pediatric surgery service for this hospital.
Physical examination shows a visible mass, not painful on palpation, soft, not attached to deep planes with reduced hernial content, not incapacitating to that of ambulation. The clinical diagnosis of left inguinal hernia is established and scheduled for surgery.
During surgery, a tubular structure is observed, rounded at the tip, vermiform and elongated in the distal part of a reddish brown color with a soft and smooth consistency protruding through the hernia sac. We proceed to remove the structure found and send it to pathology and continue with the inguinal plasty ending without incidents or accidents (Figures 1, 2, 3 and 4). The patient is released to his home and post-operative follow-up with the pediatric surgery service.
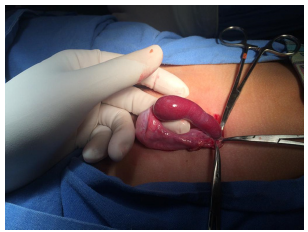
Figure 1: Discontinuous splenogonadal fusion

Figure 2: Discontinuous splenogonadal fusion
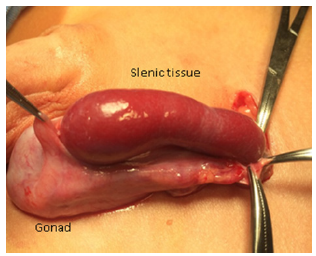
Figure 3: Discontinuous splenogonadal fusion

Figure 4: Discontinuous splenogonadal fusion. Hernia sac.
The histopathological report explains in the macroscopic description a vermiform tubular tissue of 7 cm in length and thickness of 1.3 cm of rubberized consistency compatible with splenic ectopic tissue without significant histopathological alterations or associated with gonadal tissue or mesonephric derivatives.
DISCUSSION
Although it is more common in men, these splenogonadic fusions can also occur in women. Srinivasa, et al.[9], reported a case in a 6-year-old boy who presented clinically as a strangulated left inguinal hernia, which was also resolved in our case of inguinal hernia. His case was a continuous splenogondal fusion, but our case was a discontinuous splenogondal fusion.
Recently, a theory has been proposed about this fusion associated with cryptorchidism due to an abnormal development of the suspensory cranial ligament of the testicle causing colonization of the anomalous ligament by splenic cells. Many times it can be confused with testicular tumor such as rhabdomyosarcoma as well as metastasis or lymphomas due to the great similarity and that ends unnecessarily in an orchiectomy or in the best cases with a complete approach, tumor markers and radiodiagnosis studies[10].
Continuous splenogonadal fusion may present with abdominal symptoms, and cases of intestinal obstruction may occur when the union cord is in an intraperitoneal situation or appears within the clinical picture of cryptorchidism. This continuous form is associated in 20-30% of cases with other types of congenital malformations such as cryptorchidism, peromelia, micrognathia, spina bifida, craniosynostosis, hypoplastic lung, anorectal malformation, among others. The anatomical region where presents more is in left hemiescroto with 30% of cases[11]. The inclusion of this diagnosis in the approach of all patients with inguinoscrotal masses in the pediatric age allows taking diagnostic measures of medical and surgical approach, as well as suspecting it so as not to end unnecessarily with the resection of an organ.
Discontinuous fusion exists when there is no relationship between the spleen and the gonad as in our case. Llarena Ibarguren, et al.[12], report a case of discontinuous splenogonadal fusion in a 23-year-old man on the right inguinal side Abokrecha, et al.[13], describe another case of discontinuous splenogonadal fusion in an 18-month-old child with both undescended testicles performing left orchidopexy plus incisional biopsy that formed the diagnosis. Splenogonadal fusion is a rare congenital anomaly and pediatric surgeons should be vigilant about this entity to avoid unnecessary surgeries such as orchiectomy.
Diebold J, et al.[14], in the same way he described another case of discontinuous splenogonadal fusion in an 81 years-old male.
In this review, we found only two references about discontinuous splenogonadal fusion, the first in a young adult and the second in an 18-month-old boy with no testes in the scrotum. Our case is the first one reported in a child with a palpable mass in the inguinal region, similar to an inguinal hernia that can be reduced with inguinal plasty with a biopsy that reported splenic tissue. Because this case is the first in your class it is suggested that it be called “Granados´s hernia.”
REFERENCES
1. Boestrom E (1883) Demonstration eines Praparates von Verwachsung der MilZ mit dem linken Hoden. Gellschaft deutscher Naturforscher und Artze Verhandlungen der 56 Versammlung. Freiburg 149.
2. Pommer G (1887/89) Verwachung die linken dryptorchischen Hondens und Nebenhodens mit der Milz in einer Missgeburt mit zahireichen Bildungsdefecten. Ber. D. Naturn-ned 9: 144.
3. Montes J, Tagle R, Navarro M, Iriarte C, et al. (2005) Fusión esplenogonadal. Reporte de 1 caso. Rev Chil Urol 70: 75.
4. Prada A, Vázquez JL, Montero M, Muguerza R, et al. (2006) Bazo ectópico supernumerario intraescrotal: fusión esplenogonadal discontinua. An Ped 64: 277- 9.
5. Putschar WG and Manion WC (1956) Congenital absence of the spleen and associated anomalies. Am J Clin Pathol 26(5): 429-70.
6. Petrick P (1988) Spleen in the scrotum. Am J Surg Path 12: 414.
7. Carragher AM (1990) One hundred years splenogonadal fusion. Urology 35(6): 470-71.
8. Vuong PN, Vaury P, Galet B and Baviera E (1989) Accesory spleen on the left ovary. Discussion on its pathogenesis. J Gynecol Obstet Biol Reprod (Paris) 18: 753-55.
9. Srinivasa Rao R Ch, Radhakrishna V, Rao N, Rakshit S (2018) Torsion of a Splenule in a Case of Splenogonadal Fusion Mimicking a Strangulated Inguinal Hernia. J Indian Assoc Pediatr Surg 23(2): 100–102.
10. Martín Martín S, García Lagarto E, Egea Camacho J and Fernández Del Busto E (2010) Fusión esplenogonadal. Presentación de un caso y revisión de la literatura médica. Actas Urol Esp 34(3): 288- 303.
11. Fernández Fernández JA (2002) Fusión esplenogonadal continua. An Esp Pediat 56: 373-4.
12. Llarena Ibarguren R, Añibarro Laca E, Pérez-Irezabal Pindado JC and Ibañez Calle MT (2008) Fusión esplenogonadal. Arch Esp Urol 61(3): 445-48.
13. Abokrecha A and Almatrfi A (2017) Discontinued Splenogonadal Fusion and Bilateral Empty Scrotum in an 18-Month-Old Boy. Eur J Pediatr Surg Rep 5:e1–e3.
14. Diebold J, Le Blaye O, Le Tourneau A and Marichez P (1990) Intraescrotal supernumerary spleen. A long silent case of discontinuous splenogonadal fusion. Ann Pathol 10: 174-6.