Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2023
Late Endocarditis on Aortic Prosthesis Complicated by an Infectious Aneurysm of the Right Sinus Ruptured in the Right Atrium: A Case Report
Redha Lakehal1,*, Soumaya Bendjaballah1, Khaled Khacha2, Omar Bouhidel3, Abdelmalek Bouzid3
1Department of Heart Surgery, Faculty of Medicine, EHS Dr Djaghri Mokhtar, Constantine, Algeria
2Faculty of Medicine, Algiers, Algeria
3Faculty of Medicine, Batna, Algeria
*Corresponding author: Redha Lakehal, Department of Heart Surgery, Faculty of Medicine, EHS Dr Djaghri Mokhtar, Constantine, Algeria; Tel: +213779074720; Email: [email protected]
Received Date: January 28, 2023
Publication Date: March 17, 2023
Citation: Lakehal R, et al. (2023). Late Endocarditis on Aortic Prosthesis Complicated by an Infectious Aneurysm of the Right Sinus Ruptured in the Right Atrium: A Case Report. Mathews J Cardiol. 7(1):25.
Copyright: Lakehal R, et al. © (2023)
ABSTRACT
Introduction: Endocarditis on aortic prosthesis that we all fear as patients with heart valve prosthesis, is a rare disease less than 1% of cases. However, its evolution is very unfavorable when it occurs. The appearance of a fever, often insidious, is a sure sign of the disease. Diagnosis is based on blood cultures and echocardiography. This clinical case is an opportunity for us to recall the seriousness of this condition both for patients and for cardiac surgeons. Methods: We report the case of an adult aged 51 with two mechanical mitro-aortic prostheses implanted in 2001 presenting endocarditis on aortic prosthesis complicated by aortic leak, atrioventricular block (AVB) and stroke leaving as a sequela a hemiplegia with infectious aneurysm of the right sinus ruptured in the right atrium (RA) in cardiac decompensation with persistent fever and orthopnea despite well-conducted triple anti-staphylococcal antibiotic therapy with clinical examination: aortic systolic murmur with crackling rales. Chest X-ray: cardiomegaly, flaky opacities, transthoracic echocardiography: large aneurysm on the right coronary side fistulized in the right atrium (RA), desinsertion of the aortic prosthesis with grade IV para-prosthetic aortic leak, left ventricular (LV): 52/32 mm, an undilated right ventricular (RV), an ejection fraction (EF) at 64 %, and finally a systolic arterial pulmonary pressure (SAPP) at 68 mmHg. Positive blood cultures: staphylococcus. Intraoperative exploration: voluminous vegetation next to the exit orifice of the aorta-right atrium fistula, desinsertion of the aortic prosthesis on the peri-annular abscess and vegetation on the aortic wings, destruction of the mitro-aortic junction with the presence of a fistula aorta-right atrium. He benefited from explantation of the aortic prosthesis, vegetation sent to bacteriology, reconstitution of the aortic annulus on the right coronary-left coronary (RC-LC) side by a Dacron® patch, closure of the entry orifice of the fistula on the aortic side by separate points and reconstruction of the mitro-aortic junction with a triangular Dacron® patch, implantation of an aortic prosthesis in the annular position and finally closure of the orifice of the fistula on the auricular side with a Dacron® patch under cardiopulmonary bypass. Results: The postoperative follow-up was simple. Conclusion: We underline the major interest of the prevention and the essential treatment of any infectious heart, in particular dental, at the carriers of cardiac prostheses.
Keywords: Endocarditis, Aortic Prosthesis, Prosthetic heart, Aneurysm
INTRODUCTION
Endocarditis on aortic valve prosthesis, which we all dread as patients with prosthetic heart valves, is a rare pathology which represents less than 1% of cases [1,2]. It is the most severe form of endocarditis. The diagnosis as well as the optimal therapeutic strategy remains difficult. Its evolution is very unfavorable when it occurs. The appearance of a fever, often insidious, is a sure sign of the disease. The diagnosis is mainly based on blood cultures and echocardiography. The aortic location is characterized by the anatomical aspect of valvular and perivalvular lesions, its evolution towards myocardial failure and the high number of complications motivating the early recourse to surgery. The presentation of this clinical case is an opportunity for us to recall the seriousness of this condition both for patients and for cardiac surgeons.
OBSERVATION
We report here the case of a 51-year-old adult man with both mechanical mitro-aortic prosthesis implanted in 2001 presenting endocarditis on aortic prosthesis complicated by acute pulmonary edema, complete atrioventricular block (AVB) and stroke leaving as sequelae hemiplegia with persistent fever and orthopnea despite well-conducted anti-staphylococcal antibiotic therapy.
The patient presented with NYHA functional class III, heart failure without associated angina. Clinical examination revealed a systolic aortic murmur with crackling rales at both lung bases.
The chest X-ray revealed cardiomegaly with cardiothoracic index at 0.60 associated with bilateral pulmonary fluffy opacities.
The electrocardiographic examination showed a regular sinus rhythm.
Transthoracic echocardiography (TTE) revealed multiple vegetations on the collar with almost complete desinsertion of the aortic prosthesis with para-prosthetic aortic leak grade IV, left ventricular (LV) at 52/32 mm, non-dilated right ventricular (RV), ejection fraction (EF) at 64%, shortening fraction (SF) at 40%, and finally a systolic arterial pulmonary pressure (SAPP) at 68 mmHg.
The blood count revealed inflammatory anemia associated with hyperleukocytosis. Blood cultures were positive for Staphylococcus aureus. The sedimentation rate was 93 mm in the first hour. The renal assessment was correct.
Intraoperative exploration revealed on the one hand, multiple vegetations on the aortic collar with almost complete desinsertion of the aortic prosthesis, and on the other hand a ventriculo-aortic disjunction on periannular aortic abscess.
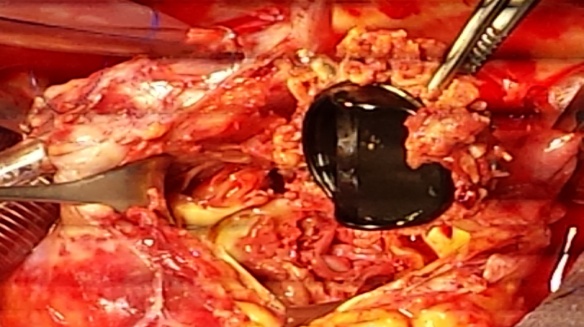
Figure 1: Intraoperative view showing endocarditis on a disinserted mechanical aortic prosthesis.

Figure 2: Intraoperative aspect showing the exit orifice of the Aorta-Right atrium fistula.
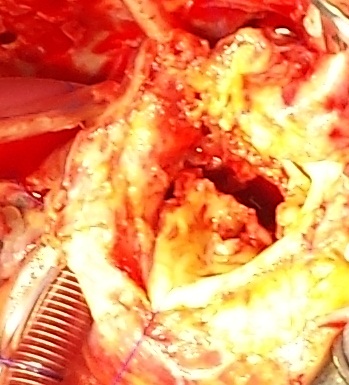
Figure 3: Intraoperative view after explantation of the mechanical aortic prosthesis.
The patient benefited from explantation of the aortic prosthesis (Figures 01, 03). The vegetations were sent to the microbiology laboratory for analysis.
The mitro-aortic junction was reconstructed with a Dacron® patch and an aortic prosthesis was implanted using the Gandjbakhch technique under cardiopulmonary bypass (CBP). (Figure 04).

Figure 4: Intraoperative aspect after explantation of the aortic prosthesis and reconstitution of the aortic annulus.
Finally, closing the orifice of the fistula on the auricular side with a Dacron® patch under CBP. Respectively, the durations of CPB, aortic clamping and circulatory support were 148, 112 and 29 minutes.
RESULTS
The immediate postoperative follow-up was simple. The stay in the intensive care unit was 48 hours, with an intubation duration of 16 hours. The total postoperative hospital stay was 22 days. Finally, with regard to anti staphylococcal antibiotic therapy, it was spread over 40 postoperative days.
DISCUSSION
Despite progress in terms of hospital hygiene, prevention and management of heart disease, infective endocarditis is still frequently encountered; its incidence does not seem to have been reduced over the past 20 years [1,2].
From a microbiological point of view, in most series, staphylococcus and streptococcus are the two most frequently encountered pathogens with no statistically significant difference [2-5]. It is a serious condition with a two-month mortality rate close to 15 to 20% in the most recent surgical series [2,3].
The time to treatment by surgery represents an important prognostic data. The place of surgery in the active phase of infective endocarditis is increasingly important, it represents half of clinical cases in Europe [1,6,7]. Infectious endocarditis on a prosthesis is a formidable complication of valve surgery (12 to 35% of cases of infective endocarditis). It is caused by the fixation of an infectious agent on the endocardium of the insertion zone of a mechanical prosthesis (ring) or on the leaflets of a bioprosthesis.
Infectious endocarditis on a prosthesis is associated with a poor prognosis. Indeed, reading the literature highlights an overall intra-hospital mortality rate varying between 20 and 40% [8]. According to Habib et al. [9], the risk factors influencing mortality in infective endocarditis on prosthesis are mainly: age, comorbidities, persistent bacteraemia, and infective endocarditis with staphylococcus aureus, heart failure, abscess, complications brain, septic shock, renal failure, mediastinitis and finally infective endocarditis on early prosthesis. Indeed, the mortality in the literature is particularly high in infective endocarditis on early prosthesis varying between 40 and 75% and it is linked to invasive micro-organisms which cause abscesses and valvular destruction, hence a large number of cardiac complications [10,11]. Regarding our clinical case, it is important to emphasize the late onset.
CONCLUSION
Aortic infective endocarditis is a formidable pathology with more frequent and earlier complications than in other valve involvement. These complications are dominated by heart failure, which is the main indication for early surgery. Early diagnosis and medico-surgical management with resection of all infected tissues are the best guarantees of a good result in the short and medium term. The patient must be informed of the vital importance of optimal management of infective endocarditis, and of its potential seriousness if this is not followed rigorously. Carriers of valvulopathies at risk must be warned of the possibility of infective endocarditis, and of the need for rapid consultation in the event of fever or deterioration in general condition. It is important to explain the role of possible gateways, in particular to encourage the patient to regularly consult a dentist or an Otorhinilaryngologist specialist. It should be remembered that the antibiotic treatment must be scrupulously followed until its term.
REFERENCES
- Steckelberg JM, Melton LJ 3rd, Ilstrup DM, Rouse MS, Wilson WR. (1990). Influence of referral bias on the apparent clinical spectrum of infective endocarditis. Am J Med. 88(6):582-588.
- Rohmann S, Seifert T, Erbel R, Jakob H, Mohr-Kahaly S, Makowski T, et al. (1991). Identification of abscess formation in native-valve infective endocarditis using transesophageal echocardiography: implications for surgical treatment. Thorac Cardiovasc Surg. 39(5):273-280.
- Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, et al. (2009). Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and the International Society of Chemotherapy (ISC) for Infection and Cancer. Eur Heart J. 30(19):2369-2413.
- Danchin N, Retournay G, Stchepinsky O, Selton-Suty C, Voiriot P, Hoen B, et al. (1999). Comparison of long term outcome in patients with or without aortic ring abscess treated surgically for aortic valve infective endocarditis. Heart. 81(2):177-181.
- Durack DT, Lukes AS, Bright DK. (1994). New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med. 96(3):200-209.
- Massoure PL, Kéreun E, Chevalier JM, Rigollaud JM, Bire F, Clémenty J, et al. (2005). Severity of aortic ring abscess complicated by cardiac conduction abnormalities. Ann Cardiol Angeiol (Paris). 54(3):132-137.
- Arnett EN, Roberts WC. (1976). Valve ring abscess in active infective endocarditis. Frequency, location, and clues to clinical diagnosis from the study of 95 necropsy patients. Circulation. 54(1):140-145.
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, et al. (2015). 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 36(44):3075-3128.
- Habib G, Thuny F, Avierinos JF. (2008). Prosthetic valve endocarditis: current approach and therapeutic options. Prog Cardiovasc Dis. 50(4):274-281.
- Chastre J, Trouillet JL. (1995). Early infective endocarditis on prosthetic valves. Eur Heart J. 16:32-38.
- Anguera I, Miro JM, San Roman JA, de Alarcon A, Anguita M, Almirante B, et al. (2006). Periannular complications in infective endocarditis involving prosthetic aortic valves. Am J Cardiol. 98(9):1261-1268.