Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Gastritis in Young Adults, the Evil in Disguise: A Review of Literature
Mrigakshi Borah1, Ria Biswas1, Aritra Saha2,*, Ajit Kumar Pegu3
1Junior Doctor, Department of Medicine, Assam Medical College and Hospital Dibrugarh, Assam, India
2Post Graduate Trainee, Department of General Medicine, Assam Medical College and Hospital, Dibrugarh, Assam, India
3Professor & Head, Department of General Medicine, Assam Medical College and Hospital, Dibrugarh, Assam, India
*Corresponding author: Dr Aritra Saha, Department of Medicine, Assam Medical College Dibrugarh, 786002, Assam, India; Tel: +91 9401650438; Email: [email protected]
Received Date: March 9, 2023
Publication Date: March 18, 2023
Citation: Borah M, et al. (2023). Gastritis in Young Adults, the Evil in Disguise: A Review of Literature. Mathews J Case Rep. 8(3):98.
Copyright: Borah M, et al. © (2023)
ABSTRACT
Inflammation of the gastric mucosa is known as gastritis. Gastritis can be primarily classified as acute and chronic. According to various seroprevalence studies, there is an increasing trend of gastritis among young adults. The review chiefly focuses on the various risk factors associated with it, its diagnosis, and the different treatment protocols available. Factors responsible for this are H. pylori, stress and anxiety, food habits, self-medication, and lack of awareness among young adults eventually leading to local ischaemia of the gastric mucosa, elevation of gastric pH, hypergastrinemia and hyperplasia of antral gastrin producing G-cells which bring about mucosal injury causing gastritis. Diagnosis predominantly comprises upper GI endoscopy, radiological modalities like USG and X-ray abdomen, tissue culture, histology, etc. The treatment essentially focuses on decreasing the gastric pH by means of medications such as PPI, H2 blockers, sucralfate, and anti-H. pylori regimen(s). Further comprehensive management may require pathological and radiological assistance.
Keywords: Gastritis, Young Adults, Students, Disease Awareness
INTRODUCTION
Gastritis is defined as inflammation of the stomach lining associated with mucosal injury and the duration of mucosal inflammation can be used to separate this condition from acute gastritis and chronic active gastritis [1].
In acute gastritis, there is dense infiltration of the gastric mucosa with neutrophilic leukocytes whereas in chronic gastritis chronic inflammatory cells like lymphocytes, plasma cells, and macrophages are predominant [2].
German physician, Georg Ernst Stahl in 1728 (quoted by Bock, 1974) first noted “gastritis” as the inflammation of the inner lining of the stomach; Giovanni Battista Morgagni, the Italian anatomical pathologist, described the signs of gastric inflammation and was the first to give the classical description of erosive or ulcerating gastritis; microscopic changes of the mucous membrane in gastric inflammation were described by Jones Handfield and Wilson Fox (1854) [3].
Prevalence
In India gastritis is seen in 3 out of 869 persons, with around 12,25,614 people being affected out of the entire population of the country and the male-to-female ratio of gastritis affected people is 1:1. The prevalence of gastritis is 87% in 10-19 years of age [4]. Sero-prevalence studies from Delhi, Mumbai, and Hyderabad show that by 10 years of age 50%, and by 20 years more than 80% of the population is infected with gastritis. The incidence rate of gastritis in the USA is 313,000. Worldwide prevalence is 2.7 million people [5,6].
Classification of gastritis
On the basis of duration, gastritis is mainly divided into acute and chronic gastritis [7].
Sydney classification of gastritis- [8]
I. Non-atrophic
II. Atrophic
i. Autoimmune
ii. Multifocal
III. Special forms
i. Chemical
ii. Radiation-induced
iii. Lymphocytic
iv. Non infectious
v. Eosinophilic
vi. Other infectious
vii. Collagenous
Etiopathogenesis
According to the Kyoto proposal, ABC classification where A refers to autoimmune, B to bacterial (infectious), and C to chemicals, covers the most relevant causes of gastritis apart from which other causes include, non-infectious systemic diseases like Crohn’s disease, sarcoidosis, vasculitis, allergies, eosinophilia, and celiac disease [9].
Generally, gastric mucosa takes about 3-6 days to renew itself by cellular proliferation and specialization which is genetically determined; however, whenever various exogenous and endogenous factors cause suppression of this regenerative process, the developing young cells become defective and more susceptible to pathological stress and ultimately die due to atrophic changes leading to achlorhydria and achylia due to loss of the normal glandular apparatus of the mucosa [8].
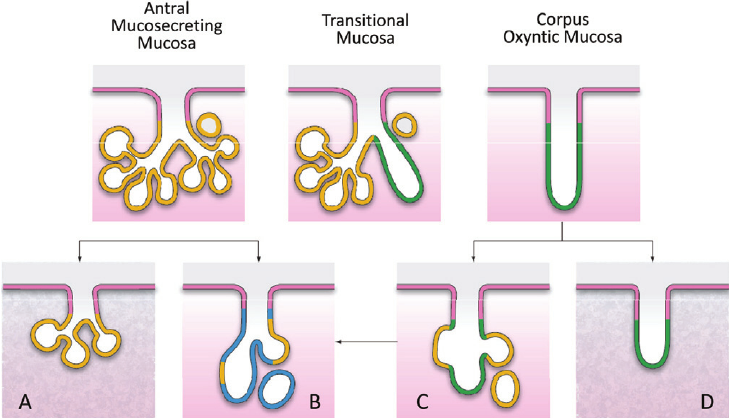
Figure 1: Normal and atrophic glandular units in the stomach. Different types of gastric native mucosa are shown at the top (the yellow line indicates mucosecreting antral glands; the green line indicates oxyntic glands; in between, the transitional mucosa shows both oxyntic and mucosecreting commitment). Atrophic changes occurring in the different types of the gastric mucosa are also shown: (A) Shrinkage of an antral glandular unit coexisting with fibrotic lamina propria; (B) Intestinal metaplasia of antral (mucosecreting) gland (blue line indicates IM); (C) Metaplastic “antralization” of oxyntic gland (pseudopyloric metaplasia = yellow line); (D) Shrinkage of an oxyntic glandular unit, partially replaced by fibrotic lamina propria. Pseudopyloric metaplastic glands may further undergo internalization (C → B) [38]
According to recent studies of gut-brain-axis, there is a bidirectional relationship between the gut and the nervous system where the gut microbiota networks with the CNS by regulating brain chemistry and influencing neuro-endocrine systems linked with anxiety, response to stress and memory function [10] The gut-brain axis forms a dense neuronal network connecting the gut with CNS via the spinal and vagal system, Hypothalamic-pituitary-adrenocorticoid axis, TRH-containing nerve fibres and capsaicin-sensitive nerves [11].
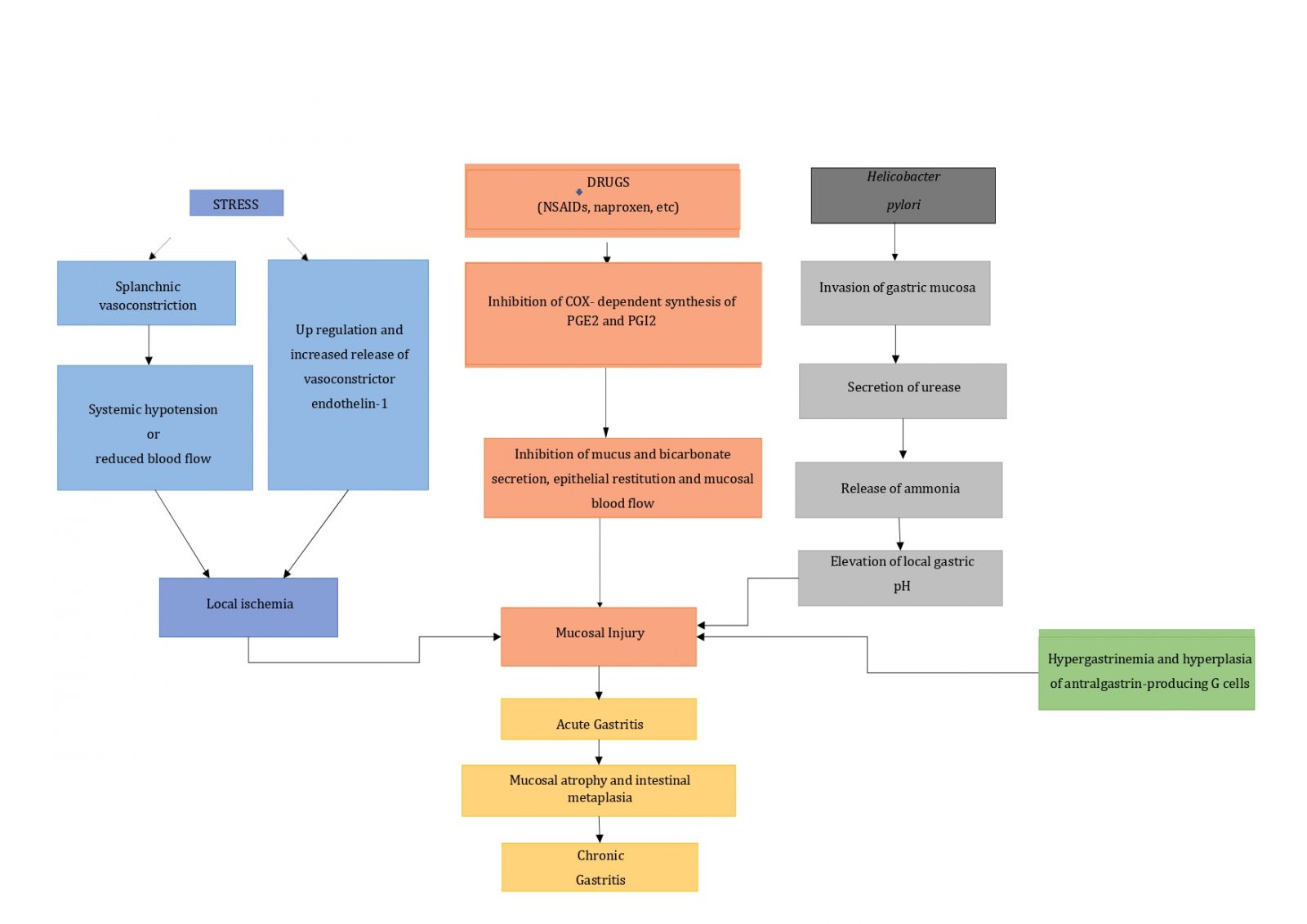
Figure 2: Pathogenesis of gastritis [12].
Clinical features
Clinical features of gastritis include epigastric pain or discomfort, nausea and vomiting, abdominal distention, postprandial fullness, feeling too full too soon during a meal, loss of appetite, weight loss, unusual feeling in throat, and abdominal cramps [13,14].
Diagnosis
Diagnosis of gastritis is mainly made on the basis of endoscopic findings via upper gastrointestinal endoscopy, along with USG and X-ray abdomen [15]. Diagnostic testing for H. pylori can be divided into endoscopic and non-endoscopic techniques which could be direct like- tissue culture, histology, or detection of bacterial antigen in the biopsy tissue or stool, or indirect like a urease breath test, antibody response to the disease [1].
Treatment
Initially, in the early days, treatment of gastritis mainly involved only surgical methods – Billroth type I and type II gastrectomy, which was followed by the blind biopsy era following the development of endoscopy [16]. However, in modern times the main treatment of gastritis involves the use of medications that reduce stomach acid like proton pump inhibitors (PPIs), H2- blockers, and sucralfate [17]. The first-line treatment for H. pylori eradication is the triple therapy regimen, which includes a standard dose proton pump inhibitor, clarithromycin, and amoxicillin for 14 days [18].
Why is it important in students?
As the prevalence of gastritis is very high in India and is mostly attributed to modifiable factors, it is crucial for students to have a thorough knowledge of gastritis so as to prevent the progression of gastritis among themselves and also to educate the society to prevent the development and advancement of gastritis [19].
Possible factors influencing gastritis in young adults?
• Helicobacter pylori infection
• Stress and anxiety
• Food habits
• Self-medication
• Lack of awareness
Helicobacter pylori infection
Helicobacter pylori is a major pathogenic factor for gastritis, gastric ulceration, and gastric malignancies [4]. H. pylori infection is also important in initiating and promoting step of the gastric carcinogenesis cascade - a series of mucosal changes for intestinal metaplasia, dysplasia, and adenocarcinoma [20]. H. pylori gradually damages the gastric mucosa causing severe atrophy and intestinal metaplasia which are risk factors for gastric cancer, thus because of the increased prevalence rate of atrophy in the young adult group, eradicating H. pylori at an age younger than 20 years may reduce the risk of gastric cancer [14].
Owing to changing epidemiologic conditions, changing resistance patterns with therapeutic implications, and now knowledge about the indications for pathogen eradication, the medical management of H. pylori is a dynamic process in need of periodic assessment [21]. During the 90s, the Standard Triple Therapy including a proton pump inhibitor, clarithromycin, and amoxicillin or metronidazole was used; in a recent systemic review, Bismuth Quadruple Therapy containing two antibiotics, tetracycline, and metronidazole has been put forward along with the implementation of Probiotics to improve the eradication regimen and decrease antibiotic side effects [22].
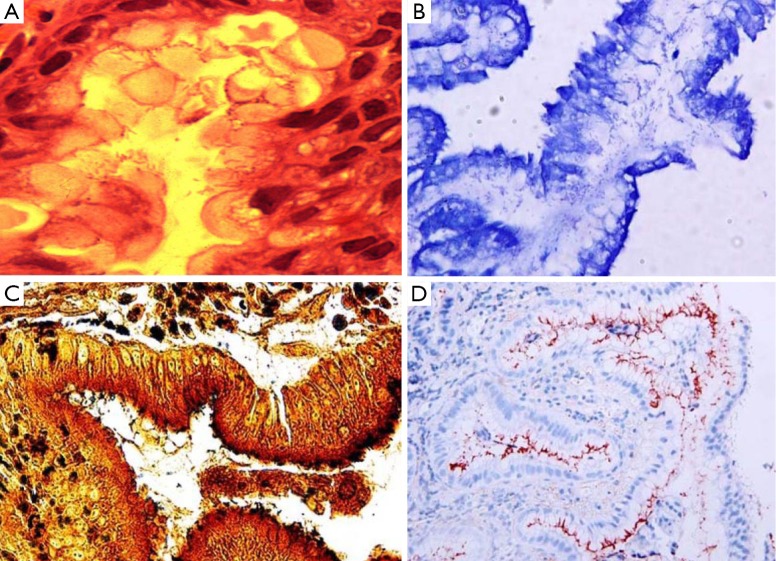
Figure 3: The spiral-shaped Helicobacter pylori organisms are present in (A) hematoxylin and eosin stain (×1,000), (B) Giemsa stain (×400), (C) Warthin-Starry silver stain (×100) and (D) immunohistochemical stain (×400) [37].
Stress and anxiety
Stress can be defined as an undue, inappropriate, or exaggerated response to a situation [23]. Anxiety can be defined as an emotion characterized by feelings of tension, worried thoughts, and physical changes like increased blood pressure [24].
Homeostatic digestion can be disrupted by altered pH which eventually results in dysregulation of the gastric environment which is aggravated by physiological stress leading to inflammation of the stomach resulting in stress-induced gastritis, whose initial stage of development is decreased mucosal resistance from toxic radicals leading to atrophy of gastric mucosa, acid-pepsin ulceration, and increased acid secretion [25]. Erosive gastritis is commonly aggravated by stress resulting from long-term illness and irritants like drugs [26]. Stress and anxiety have become an imperative part of students’ academic life due to various internal and external expectations placed on their shoulder which includes personal inadequacy, fear of failure, interpersonal difficulties with teachers, teacher-pupil relationship, and inadequate study facilities [27]. According to a study conducted by the German National Health Interview and Examination Survey, gastritis seemed to be associated with an increased incidence of mood and anxiety disorders among the general population [28]. Stress can be adequately managed by the students through class scheduling- making flexible schedules and eradicating load [29]. In order to manage stress, students should rely on problem-focused and emotion-focused coping methods, notably developing time management skills, avoiding procrastination and goal-setting behavior; along with allowing time for proper sleep and leisure activities [30].
Food habits
Majority of the young adults suffering from chronic gastritis have factors such as eating too fast, irregular mealtimes, eating leftover food, high intake of sugar and salt, excessive consumption of alcohol, and smoking as significant factors in aggravating the symptoms [31]. Excessive intake of fatty, sugary, spicy dishes and binge drinking of alcohol can lead to episodes of acute gastritis [7]. Concentrated carbohydrates stimulate osmoreceptors retarding stomach deflation; fatty foods retard gastric emptying and high purine-based foods raise acid secretion [32].
Epidemiological studies suggest that circadian dysfunction, skipping breakfast, and frequent night binging lead to increased risk for Gastrointestinal symptoms such as stomach ache and nausea [31].
Thus, cessation of alcohol, smoking, anti-inflammatory drugs, spicy food, dietary modification, and maintaining regularity in meals can prove to be sufficiently beneficial [7].
Self-medication
Self-medication is defined by World Health Organization (WHO) as “the use of drugs to treat self-identified symptoms or use of prescribed drug continuously or intermittently for chronic or recurrent diseases without periodic consultation with health care provider” [33].
Various clinical manifestations due to undue intake of drugs include nausea, vomiting, epigastric discomfort, heartburn, bloating, dyspepsia, hematemesis, and melena. Injudicious and excessive intake of over-the-counter medications is another important aiding factor [34]. The use of NSAIDs, especially in patients with H. pylori infection can cause the chance of gastric and duodenal ulcers [35].
One of the root causes of self-medication is a lack of knowledge of consultation with physicians which can be prevented by making the public aware of Self-medication and strict monitoring of easy availability of over-the-counter drugs [33]. Spreading awareness about the various deleterious effects of self-medication among the population and the execution of proper policies and actions are urgently needed to prevent self-medication [36].
Lack of awareness
Adolescents have an average level of knowledge of gastritis and its consequences, with sex and demographic characteristics being the major influencers on gastritis prevalence among late adolescence [37]. The major demographic variables included Age, Gender, Educational status of mother and father, occupational status of mother and father, monthly family income, previous knowledge, and source of information [6].
Factors like peer pressure and newly found freedom give a gate to achieve lifestyle changes through alcoholism, smoking, tobacco, and excessive and frequent intake of fast foods which influence the occurrence of gastritis [5].
A study conducted among 2nd year B.Sc. nursing students revealed that 40% of the subjects had inadequate knowledge, 56.6% had moderately adequate knowledge and only 3.4% had adequate knowledge about gastritis [19].
How to solve this? [5,19]
- Identification of high-risk behaviour and lifestyle pattern.
- Screening for signs and symptoms of gastritis Spreading awareness about the risk factors and its adverse effects on health via organised campaigns in TV, radio, press and other media.
- Educational programmes to stop high-risk behaviour like smoking, alcohol consumption, fast food, and spicy foods.
- Arrangement of special classes and periodic assessments.
DISCUSSION AND CONCLUSION
Gastritis is the inflammation of the stomach. It includes various clinicopathological entities. It may occur suddenly (acute gastritis) or appear slowly over time (chronic gastritis). Common signs and symptoms include nausea, vomiting, the feeling of fullness, burning ache or pain in the upper abdomen, etc. After a thorough literature review, we conclude that the main factors causing gastritis in young adults are H. pylori infection, stress, and anxiety, irregular food habits with inappropriate food choices, and drug abuse. Various modes of diagnosis include careful history taking, tests for H. pylori, and other investigations like endoscopy and X-ray of the abdomen.
Treatment of gastritis should focus on specific causes as well as a comprehensive development of healthy lifestyle choices. Medications used to treat gastritis include antibiotic regimens for H. pylori eradication, medication that blocks acid production and promotes healing, and medications that reduce acid production and neutralise stomach acid. Lifestyle and home remedies can include a proper diet at regular intervals, a proper sleep-wake cycle, avoiding alcohol and excessive oily and sweet foods, and steady physical activity in a graded pattern.
REFERENCES
- Watari J, Chen N, Amenta PS, Fukui H, Oshima T, Tomita T, et al. (2014). Helicobacter pylori associated chronic gastritis, clinical syndromes, precancerous lesions, and pathogenesis of gastric cancer development. World J Gastroenterol WJG. 20(18):5461–5473.
- Sleisenger and Fordtran’s. (2022). Gastrointestinal and Liver Disease.
- Laszlo I, Cseko K, Czimmer J, Mozsik G. (2022). Diagnosis of Gastritis – Review from Early Pathological Evaluation to Present Day Management. In: Mozsik G, editor. Current Topics in Gastritis.
- Kuntoji SB, Naik AA, Suhas SD. (2020). A prospective study of proportion of Helicobacter pylori infection in patients presenting with dyspeptic symptoms in S. Nijalingappa Medical College and H.S.K. Hospital, Bagalkot. Int Surg J. 7(8):2685–2690.
- Gv P, Sp S, M N, Begum F, Tt S, Gv P. (2013). Knowledge and Factors Influencing on Gastritis among Distant Mode Learners of Various Universities at Selected Study Centers Around Bangalore City With a View of Providing a Pamphlet. Sch J App Med Sci. 1(2):101-110.
- Sreelatha DM, Sushma R, Rani DPS. (2021). A Comparative Study To Assess The Knowledge On Gastritis Among Male And Female Undergraduates In Selected Areas Of Chittoor. Int J Creative Research Thoughts. 9(1):13.
- Azer SA, Akhondi H. Gastritis. (2022). In: StatPearls. Treasure Island (FL): StatPearls Publishing; Chronic gastritis:37.
- Wirth HP, Yang M. (2016). Different Pathophysiology of Gastritis in East and West? A Western Perspective. Inflamm Intest Dis. 1(3):113–122.
- Appleton J. (2018). The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health. Integr Med Clin J. (4):28–32.
- Sgambato D, Capuano A, Sullo MG, Miranda A, Federico A, Romano M. (2016). Gut-Brain Axis in Gastric Mucosal Damage and Protection. Curr Neuropharmacol. (8):959–966.
- NIH. (2022). Symptoms & Causes of Gastritis & Gastropathy | NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases.
- Hojo M, Nagahara A, Kudo T, Takeda T, Ikuse T, Matsumoto K, et al. (2021). Endoscopic findings of Helicobacter pylori gastritis in children and young adults based on the Kyoto classification of gastritis and age‐associated changes. JGH Open. 5(10):1197–1202.
- Muszyński J, Ziółkowski B, Kotarski P, Niegowski A, Górnicka B, Bogdańska M, et al. (2016). Gastritis – facts and doubts. Przegla̜d Gastroenterol. 11(4):286–295.
- Siurala M. (1991). The Story of Gastritis. Scand J Gastroenterol. 26(186):1–3.
- NIH. (2022). Treatment of Gastritis & Gastropathy | NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases.
- Evidence-Based Guidelines for the Treatment of Helicobacter pylori Infection in Korea 2020.
- Hemavathy V, Devi TV. A study to assess the knowledge on gastritis among 2nd year B.Sc nursing students in Sree Balaji College of Nursing. Int J Appl Res. Chennai:3.
- Liu KSH, Wong IOL, Leung WK. (2016). Helicobacter pylori associated gastric intestinal metaplasia: Treatment and surveillance. World J Gastroenterol. 22(3):1311–1120.
- Fischbach W, Malfertheiner P. (2018). Helicobacter pylori Infection. Dtsch Arzteblatt Int. 115(25):429–436.
- Goderska K, Agudo Pena S, Alarcon T. (2018). Helicobacter pylori treatment: antibiotics or probiotics. Appl Microbiol Biotechnol 102(1):1-7.
- Familoni O. (2008). An overview of stress in medical practice. Afr Health Sci. 8(1):6–7.
- Americal Psychological Association. (2022). Anxiety.
- Megha R, Farooq U, Lopez PP. (2022). Stress-Induced Gastritis. In: StatPearls [Internet]. Treasure Island (FL): Stat Pearls Publishing.
- Gastritis - Digestive Disorders. MSD Manual Consumer Version.
- Vakil N. (2023). Gastritis. MSD.
- Reddy KJ, Menon KR, Thattil A. (2018). Academic Stress and its Sources Among University Students. Biomed Pharmacol J. 11(1):531–537.
- Goodwin RD, Cowles RA, Galea S, Jacobi F. (2013). Gastritis and mental disorders. J Psychiatr Res. 47(1):128–132.
- Yasmin H, Khalil S, Mazhar R. (2020). Covid 19: Stress Management among Students and its Impact on Their Effective Learning. 4(2):10.
- Dyson R, Renk K. (2006). Freshmen adaptation to university life: depressive symptoms, stress, and coping. J Clin Psychol. 62(10):1231–1244.
- Li Y, Su Z, Li P, Li Y, Johnson N, Zhang Q, et al. (2020). Association of Symptoms with Eating Habits and Food Preferences in Chronic Gastritis Patients: A Cross-Sectional Study. Evid Based Complement Alternat Med. 2020:5197201.
- Choi MK, Kang MH, Kim MH. (2015). Dietary intake assessment and biochemical characteristics of blood and urine in patients with chronic gastritis. Clin Nutr Res. 4(2):90–96.
- Paudel S, Aryal B. (2020). Exploration of self-medication practice in Pokhara valley of Nepal. BMC Public Health. 20(1):714.
- Philpott HL, Nandurkar S, Lubel J, Gibson PR. (2014). Drug-induced gastrointestinal disorders. Frontline Gastroenterol. 5(1):49–57.
- Metanat M. (2015). Self-Medication With Analgesics and Helicobacter pylori Infection. Int J High Risk Behav Addict. 4(2):e26155.
- Saha A, Marma KKS, Rashid A, Tarannum N, Das S, Chowdhury T, et al. (2022). Risk factors associated with self-medication among the indigenous communities of Chittagong Hill Tracts, Bangladesh. PLOS ONE. 17(6):e0269622.
- Silwal S, Acharya A, Baral B, Devkota A, Subedee A, Paudel U. (2021). Knowledge Regarding Gastritis among Late Adolescence in Central Nepal. Marsyangdi J. 2(1):81–93.
- Lee JY, Kim N. (2015). Diagnosis of Helicobacter pylori by invasive test: histology. Ann Transl Med. 3(1):10.
- Rugge M. (2011). Normal and atrophic glandular units in the stomach.