Information Links
Related Conferences
Previous Issues Volume 8, Issue 6 - 2023
Foreign Body Complications in the Oro-Facial Region
Mahmuda Akhter1,*, Jewel Rana2, AKM Erfanul Hoque3
1Oral & Maxillofacial Surgery Department, Bangabandhu Sheikh Mujib Medical University, Bangladesh
2Resident, Oral & Maxillofacial Surgery Department, Bangabandhu Sheikh Mujib Medical University, Bangladesh
3Oral & Maxillofacial Surgery Department, BIHS General Hospital, Bangladesh
*Corresponding Author: Dr. Mahmuda Akhter, MS, FCPS, FICD, Oral & Maxillofacial Surgery Department, Bangabandhu Sheikh Mujib Medical University, Bangladesh; Email: [email protected]
Received Date: March 23, 2023
Publication Date: April 29, 2023
Citation: Akhter M, et al. (2023). Foreign Body Complications in the Oro-Facial Region. Mathews J Case Rep. 8(6):106.
Copyright: Akhter M, et al. © (2023)
ABSTRACT
Study Design: A case report. Objective: To identify the problems and solutions of the treatment of foreign body trauma in the maxillofacial region. Methods: Two cases of foreign body trauma patients include physical examination findings, radiological images and follow-up was documented to find out the after effect of residual part and treatment outcomes. Result: Both patients received treatment immediately after injury. But few months later complications arise due to the remnant of foreign body. In case of first patient location was not suitable for USG and radiology also unsuccessful to notice the presence of foreign body. In case of 2nd patient need further treatment after initial management. Conclusion: Causes for the remnant of foreign body during first steps of management are bleeding, proximity to the vital structures, and hiding in the spaces created by multiple fascia layers in the oro-facial region and causes late complications like swelling, trismus, discharging sinuses, etc. Radiological imaging sometimes fails to detect the presence and position of remnants. So further treatment is very difficult for the surgeon.
Keywords: Retromolar trigon, Trismus, Orofacial region, Foreign body
INTRODUCTION
Impaction of foreign bodies in the maxillofacial region is not uncommon [1]. Most common cause for foreign bodies in the tissue of oral cavity is trauma. Glass, metal and wood are the most common among the reported foreign bodies in the head neck area [2]. Approximately one-third of all foreign bodies has been missed during initial examinations and management in the emergency department [3]. Because of complex anatomical structures and vulnerable organs like vascular, nervous, auditory and visual systems. Sometimes part of foreign body hides in the deeper tissue without any immediate clinical presentation.
Late diagnosis of foreign body in the maxillofacial region is not easy because of asymptomatic condition for a time period [4]. Reasons of asymptomatic period are size, nature, position of the object into deeper facial tissues, and radiographically invisibility of the objects. All these issue causes challenges for the late diagnosis, isolating and removing the remnant of foreign bodies. This hidden foreign body usually incites a chronic inflammatory reaction and may progress to a grievous source of infections [5].
Here are two interesting cases of the foreign body remnant in the orofacial region after initial management with late complications.
CASE REPORT- 1
A11-year-old boy referred from ENT out-patient department with the complaints of a right cheek swelling with gradual reduction of mouth opening for six months and it was painful when he tries to open his mouth. Due to difficulties in taking foods, he had to shift liquid diet from solid. He gave the history of traumatic impaction of a bamboo stick in the right lower face along the right angle of the mouth and he underwent surgery one year back. On examination a scar mark approximately one cm below the right angle of mouth was found. Mouth opening was 7mm (Figure 1). On palpation, intra -orally a thick fibrotic band felt near the right retromolar trigone. Trismus limits adequate intra–oral examinations. Orthopantomogram imaging reveals no significant causes. Contrast CT scan of the maxillofacial region had been done to delineate the swelling. It reveals a diffuse ill–defined soft tissue swelling in the right infra – temporal region involving the adjacent pterygoid muscles and Para–pharyngeal region with the loss of fat plane (Figure 2). Body, alveolar process and ramus of mandible show normal bony density and cortical thickness (Figure 3). Interpretation recommends a right para–pharyngeal abscess without any evidence of foreign body. But there was no history of pus discharge or discharging sinus.
So based on the history of foreign body trauma six months ago, trismus, CT scan report planning was surgical exploration under general anesthesia. A submandibular modified lip splitting incision on the right side was given to avoid the injury of mental nerve. Dissection protocol had been followed to preserve the marginal mandibular nerve. Full thickness mucoperiosteal flap was elevated from baccal side of mandible to approach the infra-temporal space. A bamboo stick about 3 cm length was found in the infra-temporal space (Figure 4). Per-operatively, the foreign body bed was smooth.
Post – operatively patient’s mouth opening improved significantly. After one year follow-up, patient’s mouth opening is 40mm (Figure 5), Intra-oral mucosa is normal colour and texture (Figure 6), and angle of lip is also in normal anatomical position (Figure 7).

Figure 1: Eleven-year–old boy with limitations of mouth opening, which is about 7 mm. Swelling and scar mark of right cheek.
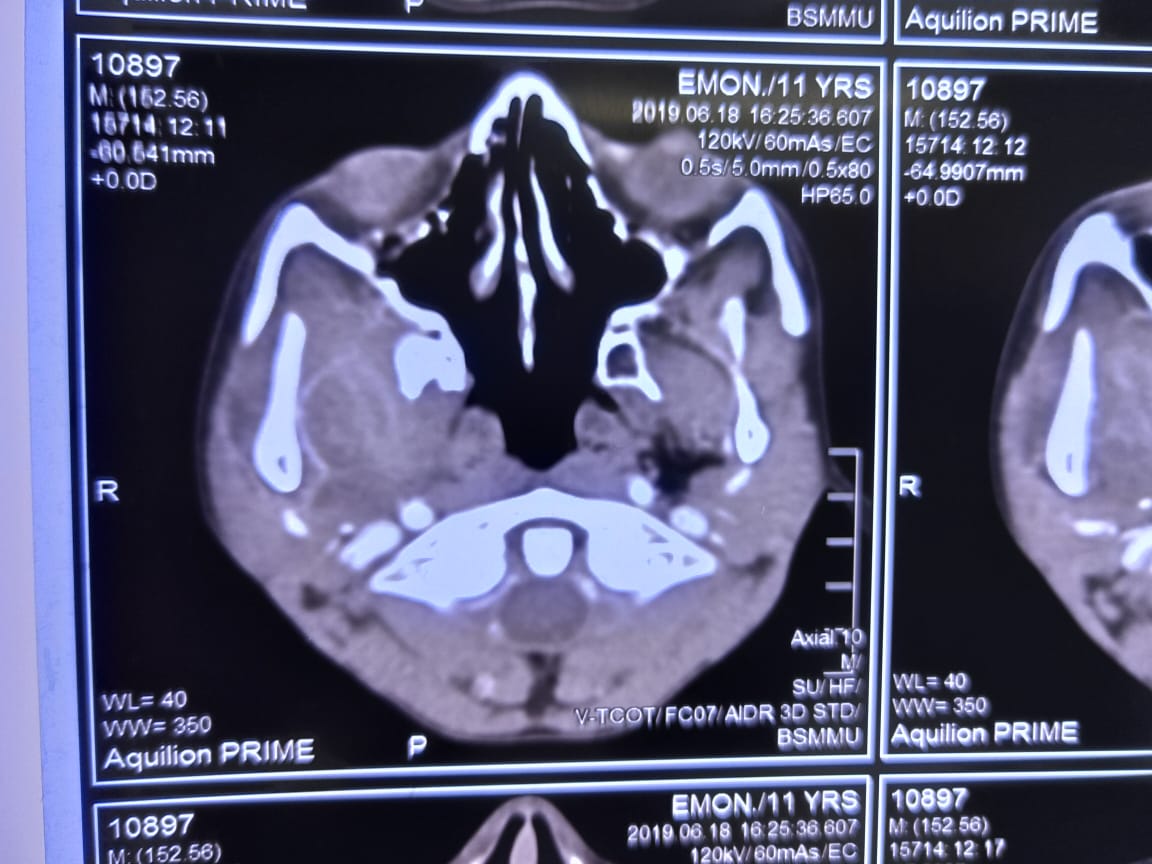
Figure 2: Axial view of the maxillofacial CT scan shows a diffuse ill-defined soft tissue swelling in the right infra-temporal region involving the adjacent pterygoid muscles and Para–pharyngeal region with the loss of fat plane.
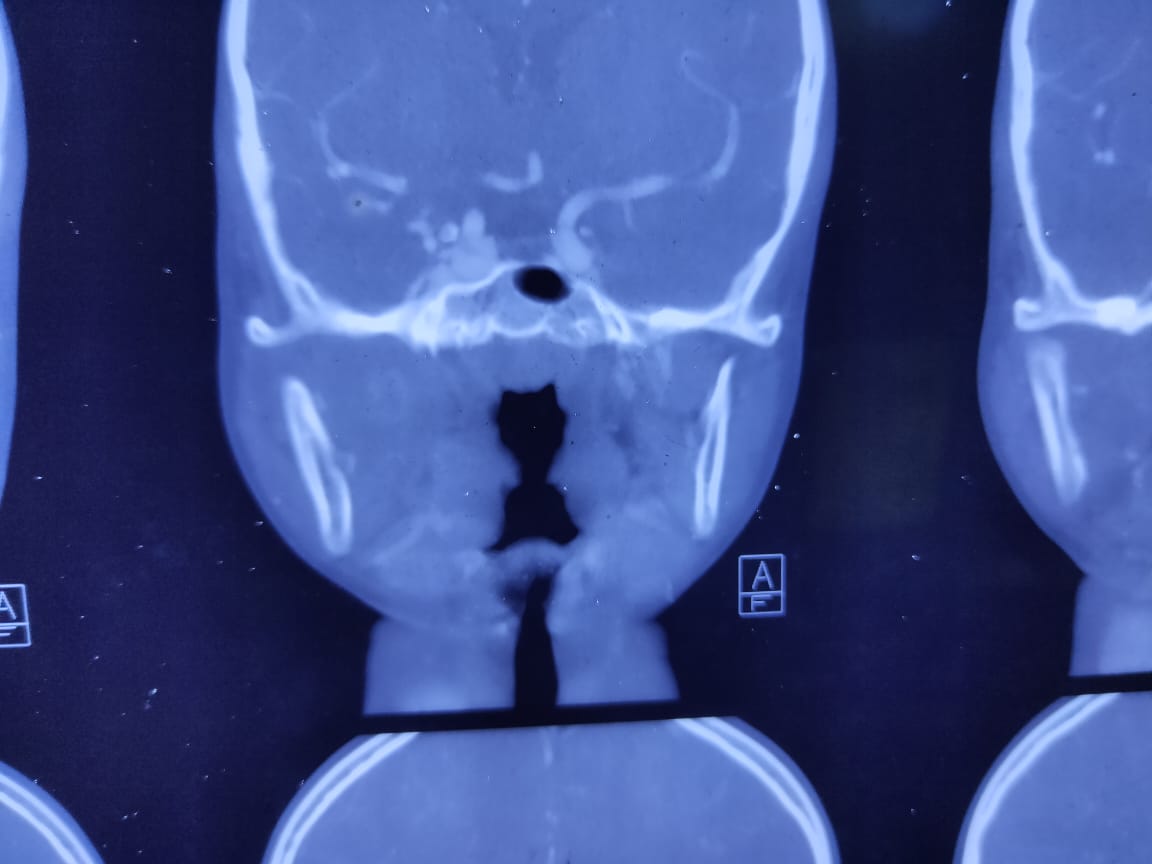
Figure 3: Coronal view of the maxillofacial CT scan shows a diffuse ill-defined soft tissue swelling in the right infra-temporal region involving the adjacent pterygoid muscles and Para–pharyngeal region with the loss of fat plane. Mandible and alveolar processes and ascending ramus show normal bony density and cortical thickness.
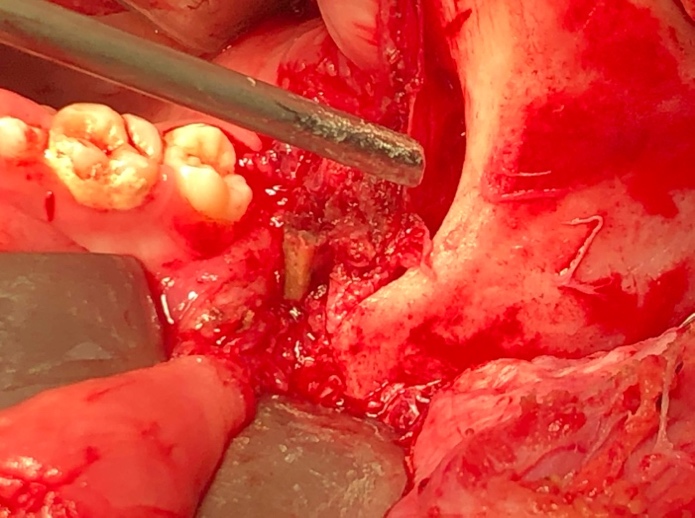
Figure 4: Per-operative picture of foreign body, located in the infra temporal fossa.
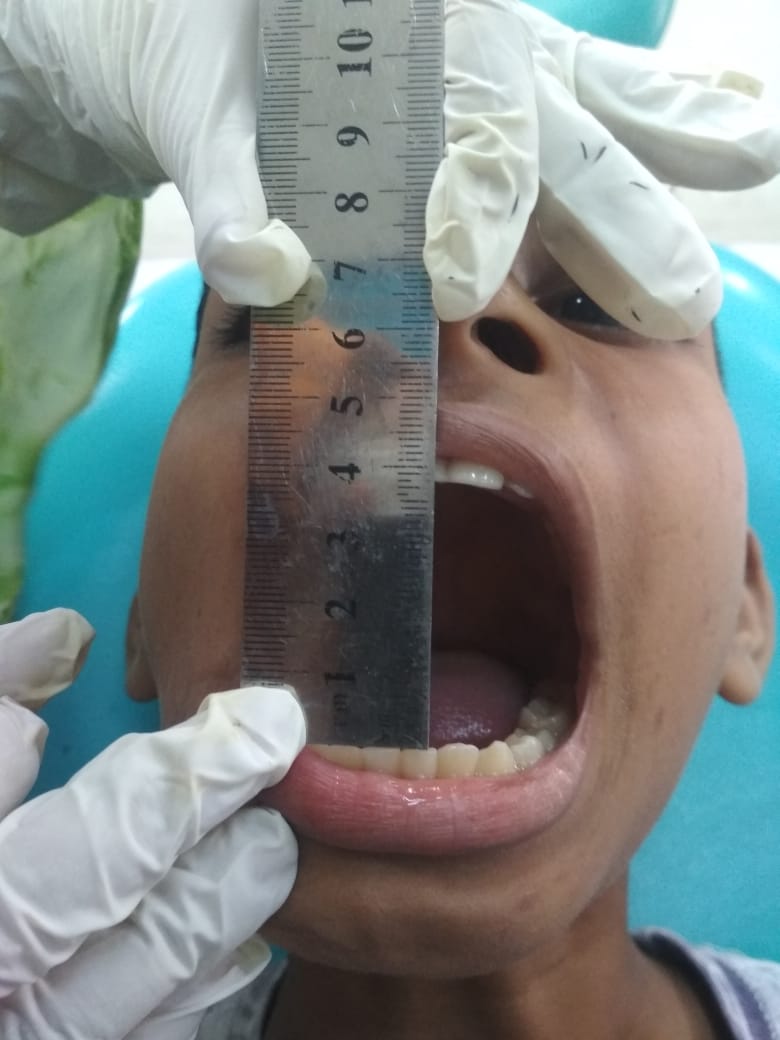
Figure 5: After one year follow-up, patient’s mouth opening is 40mm.

Figure 6: After one year follow-up, Intra-oral mucosa is normal colour and texture.

Figure 7: After one year follow-up, angle of lip is also in normal anatomical position.
CASE REPORT- 2
A 33-year female patient, reported in the OPD of the Oral and Maxillofacial Surgery department of Bangabandhu Sheikh Mujib Medical University (BSMMU) with the complaints of diffuse swelling of the right side of the face and pus discharged from the right side of nose for last 20 days( Figure-8). She had a history of trauma to the right side of nose by a Organic stick in an arable land about 29 days back. A cut injury was found about 5 mm above the ala of right side of nose. Wound was treated in the local hospital under the coverage of antibiotics.
On 3rd POD Day, pus discharged from the sutured margins. Then on 10thpost operative day abscess was drained and removed a tiny foreign body approximately 3mm X 7mm X 2mm from the area. Oral antibiotics were taken for another 5 days.
Even after the second intervention of taking out the foreign body, pus discharging was not stopped. Rather, she developed a painful, gradually increasing swelling in right middle 3rd of face. For that reasons she was referred to the department of Oral and Maxillofacial Surgery of Bangabandhu Sheikh Mujib Medical University (BSMMU) Dhaka.
On examination, diffuse swelling of right middle third of face about 6cm X6cm in diameter with tenderness, shiny, firm consistency was noted. But no changes of overlying skin color. Intraoral aspiration, blood-stained pus found. She was otherwise healthy. No relevant systemic diseases were found.
Imaging failed to find out any abnormalities. USG of the swelling reveals an intramuscular irregular thick walled an-echoic area (measuring about 5.13cm x 1.85cm x 3.75cm) with a foreign body within the area (Figure-9). Which was suggesting abscess. A sinus track found from abscess to the skin along the ala of right side of nose.
Under local anesthesia intraoral vestibular incision was given (Figure-10). Entering the abscess, two separate foreign bodies (parts of jute stick measuring 2cm x 1cm x 5mm and 1cm x 3mm x 2mm respectively) was found (Figure-11). Further exploration was done to ensure the removal of all foreign bodies. a drain tube was placed intraorally. Wound closed by 3.0 poly-galactine suture material.
5th POD, swelling was subsided (Figure-12). The drain tube, sutures was removed. In one month, three months and six months follow up there was no history of pain or pus discharge.

Figure 8: A 33-year female Patient, reported with the complaints of diffuse swelling of the right side of the face and pus discharged from the right side of nose for last 20 days.
.jpg)
Figure 9: USG of the swelling reveals an intramuscular irregular thick walled an-echoic area (measuring about 5.13cm x 1.85cm x 3.75cm) with a foreign body within the area.

Figure 10: Under local anesthesia intraoral vestibular incision was given to explore the foreign bodies.
Figure 11: Per operatively, two separate foreign bodies (parts of jute stick measuring 2cm x 1cm x 5mm and 1cm x 3mm x 2mm respectively) were found.
Figure 12: On 5thpost operative day, swelling was subsided.
DISCUSSION
The masticator spaces are a complex area in the maxillofacial region. Masticator space pathology includes inflammatory conditions of odontogenic origin, lympho-vascular malformations, as well as benign and malignant tumours.6Odontogenic infections and benign/malignant tumors are the usual differentials among pathologies that may occur in this region with the complaints of a swelling and trismus. Trismus is the main symptom of foreign body in the infra – temporal and retromolar region [7,8].
One third foreign bodies have been skipped during initial management [9]. The diagnosis of a foreign body can be achieved by a combination of history, clinical examinations, and imaging techniques. The potential space of orofacial region filled with loose connective tissue and remnant of foreign bodies in these spaces can remains without any immediate presentation but causes chronic inflammatory reaction and late clinical presentations. Most of the time late clinical presentation due to this remnant causes diagnosis dilemma [10]. Sometimes the presence of a foreign body can’t be confirmed by any investigations, even by radiological imaging. With the history of traumatic injuries, surgical repair, buccal swelling and Trismus after few weeks to months, leads to the suspicion of a reactive complications of residual of foreign body. In this situation surgical exploration mostly help to evaluate and correct the clinical ailments. Plastic, wooden and bamboo materials are not identifiable by radiological images, moreover deeper impaction in the spaces makes it more invisible. CT scan sometimes reveals gas bubbles images in the presence of bamboo/wooden foreign bodies in the soft tissues. CT scan of the case no-1 reveals the same in infratemporal space and the foreign body was removed from medial side of the angle of mandible. Though asymptomatic period for a certain time and migrating characteristics of a foreign body creates some confusion, but history of trauma is the guideline to lead us to the successful result. After few months of the trauma, the residual wood or bamboo pieces becomes denser than muscles in the fatty layer which may be misdiagnosed as an usual or normal tissue plane in the CT scan. Due to the indistinct character of the foreign body in the radiological images, contributory history of a trauma and nature of an injurious agent is the key points to avoid future hazardous consequences.
Beside adverse clinical outcomes, undetected foreign bodies may also result in medicolegal consequences if the patient takes legal action [11,12].
CONCLUSION
Emergency management of trauma of maxillofacial regions sometimes fails to assess the consequences in the primary health care centers of the rural area or hospitals due to the other associated complications like bleeding, soft tissue injury, head injuries and other vital structures injury. Inadequate training, manpower, under-facilities also worsen the management in these centers. Remnant of foreign body may be a consequence of these limitations. So, reporting with swelling, trismus and other suggestive symptoms after a latent period of initial management of trauma should be evaluated correctly and manage carefully and thoroughly.
Sometimes foreign bodies are not obvious in the imaging investigations. Foreign body may migrate to the different tissue plane making diagnosis dilemmas. If need CT scan, MRI should be advised to find out every piece in the orofacial soft tissues. So, we should be meticulous to handle the foreign body to avoid grave consequences and future morbidity for the patients.
DECLARATION OF CONFLICT OF INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FOOTNOTES
Informed Consent -Written consent was obtained from the patients whose identifiable images were included in this study. Consent was also obtained from patients for the use of their deidentified case information.
IRB Statement -The Ethical Committee exempted the approval for this article, because it is a case report and the patients had signed the informed consent for the publication of their data.
Eggers G, Haag C, Hassfeld S. (2005). Image-guided removal of foreign bodies. Br J Oral Maxillofac Surg. 43:404-409.
Levine MR, Gorman SM, Young CF, Courtney DM. (2008). Clinical characteristics and management of wound foreign bodies in the ED. Am J Emerg Med. 26:918–922.
Krimmel M, Cornelius CP, Stojadinovic S, Hoffmann J, Reineri S. (2001). Wooden foreign bodies in facial injury: a radiological pitfall. Int J Oral Maxillofac Surg. 30:445–447.
Ebner F, Tolly E, Tritthart H. (1985). Uncommon intraspinal space occupying lesion (foreign body granuloma) in the lumbosacral region. Neuroradiology. 27:354-356.
Manthey DE, Storrow AB, Milbourn JM, Wagner BJ. (1996). Ultrasound versus radiography in the detection of soft tissue foreign bodies. Ann Emerg Med. 28:7-9.
Fernandes T, Lobo JC, Castro R, Oliveira MI, Som PM. (2013). Anatomy and pathology of the masticator space. Insights Imaging. 4:605–616.
Purohit JP, Kumar G, Singh PN. (1996). An unusual foreign body in infratemporal fossa. Indian J Otolaryngol Head Neck Surg. 48(4):323–324.
Thakur JS, Chauhan CGS, Diwana VK, Chauhan DC. (2007). Trismus: an unusual presentation following road accident. Indian J Plast Surg. 40(2):202–204.
Anderson M, Newmeyer WL, Kilgore ES. (1982). Diagnosis and treatment of retained foreign bodies in the hand. Am J Surg. 144:63-65.
Lee DA, Oh YS. (2007). Unusual, delayed presentation of a nail gun injury through the skull base. Laryngoscope. 117(6):977–980.
Bettman JW. (1990). Seven hundred medicolegal cases in ophthalmology. Ophthalmology. 97:1379–1384.
Kaiser CW, Slowick T, Spurling KP, Friedman S. (1997). Retained foreign bodies. J Trauma. 43:107–111.