Information Links
Related Conferences
Previous Issues Volume 4, Issue 1 - 2020
Faciometrics: A Practical Guide for Orofacial Harmonization
Tatiany Bertollo COZER1, Marcela Carvalho ESPALADORI2, Micena Roberta Miranda Alves e Silva2, Maria Tereza SCARDUA1
1Tereza Scardua Institute – São Paulo, SP, Brazil 2Department of Morphology, Institute of Biological Sciences, University Federal of Minas Gerais, Belo Horizonte, MG, Brazil
*Corresponding author: Marcela Carvalho Espaladori, Departamento de Morfologia, Intituto de Ciências Biologicas, Universidade Federal de Minas Gerais, CEP 31270-901, Belo Horizonte, e-mail: [email protected]
Received Date: October 29, 2020 Published Date: December 27, 2020 Copyright: Espaladori MC, et al. ©2020 Citation: Espaladori MC, et al. Faciometrics: A Practical Guide for Orofacial Harmonization. M J Derm. 04(1):14.
ABSTRACT
Faciometrics consists of making direct measurements from predefined anthropometric points that allow data to be obtained in a simple and practical way. To acquire these facial measurements, we propose the use of a specific facial ruler and following standardized references for quantitative analysis. The relationship between these measurements will guide facial interpretation. With these normative parameters, we can guide harmonization procedures and recover facial proportions, making facial features more similar to the reference. In this way, we will achieve more individualized planning that will be a more assertive approach in the proposed treatment. The purpose of this article is to describe a method that enables faciometrics using a frontal norm. A purely subjective facial analysis, which is linked to conventional planning, can also be quantified through the use of a facial ruler and then interpreted to develop effective planning in facial harmonization.
KEYWORDS: Facial Analysis; Faciometrics; Facial Ruler; Facial Harmonization
INTRODUCTION
Beauty cannot be explained by a single principle; instead, a variety of features of the human face are responsible for the perception of beauty. Among them, proportion is undoubtedly one of the main characteristics [1,2]. Thus, measuring known facial structures, their peculiarities and deviations will help in the perception of the nuances that influence individual aesthetics; this is the first step for those who are willing to perform facial procedures. Faciometrics consists of making direct measurements from predefined anthropometric points that allow data to be obtained in a simple and practical way [3,4]. In addition to the analysis of anthropometric points, the analysis of facial lines becomes relevant. These lines can be vertically and horizontally characterized by the true vertical line (TVL) because the TVL is a line parallel to the plumb line. The true horizontal line (THL), by analogy, is the line perpendicular to the TVL. Its decompositions are parameters of simple execution, which will assist in the visualization of deviations and asymmetries that are often overlooked during clinical examination [4,5].
The initial stage of facial analysis involves examining the face in frontal view. For this, a measuring instrument is used to obtain direct objective data during the clinical examination of facial morphology. Different types of rulers are available in the literature for these measurements [6]. Most of them use an extension of ten centimeters adapted to conventional rulers to measure the bizygomatic distance (Zi-Zi) [6].
The great diversity of facial analysis parameters found in the literature may, at first, represent a practical obstacle, making it difficult to apply to daily practices. In addition, there is a dearth of studies that address facial analysis in a frontal norm and that are specifically aimed at orofacial harmonization (OFH).The fact is that there is a gap in the literature of scientific parameters, with quantifiable evidence and proven applicability in clinical practice. Therefore, the purpose of this article is to describe a step-by-step method of acquiring faciometric measurements in frontal norms with the aid of a Beauty Setup® facial ruler, which will enable the quantification and interpretation of facial measures, thus guiding aesthetic procedures in orofacial harmonization.
METHOD
To collect facial measurements, the examiner must be positioned in front of the patient to be evaluated, whose head must be in a neutral position, called the natural head position. Thus, we position the THL parallel to the ground line (Figure 1). This position is a standardized, self-balancing, reproducible orientation of the head in space when the individual is focusing on a distant point at eye level [7–11]. All anthropometric points (Figure 2) must initially be precisely located through palpation. After their determination, the next step is to use the ruler.
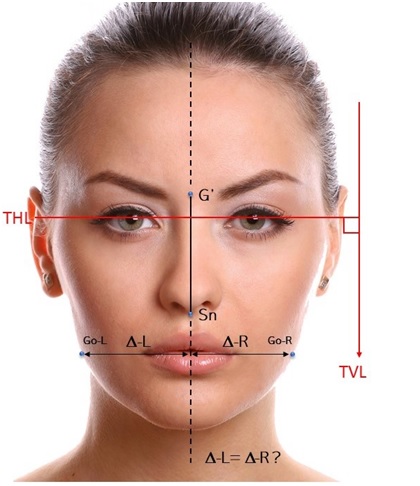
Figure 1: Facial lines.
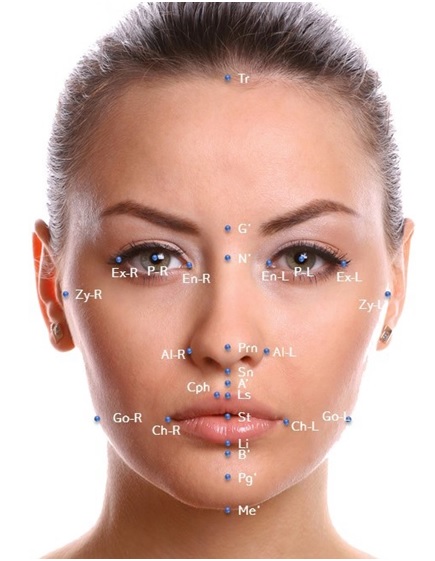
Figure 2: Anthropometric points most used in facial analysis for orofacial harmonization.
The facial ruler is a measuring instrument widely used to obtain objective data during the clinical examination of facial morphometry. In order to facilitate the clinical record of the measures enshrined in the analysis of the facial proportion without the need to adapt the caliper extensions available on the market, a manual instrument was created: the Beauty Setup® facial ruler (Figure 3).
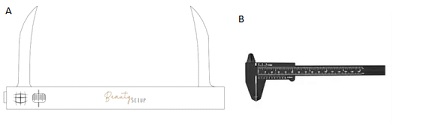
Figure 3: Illustration of the Beauty Setup ruler (A) Caliper (B).
This instrument consists of two extensive components that make it possible to take linear measurements directly on the face, as it directly reaches all anthropometric points. It has been shown to be reproducible with good interobserver agreement (kappa = 0.89). A conventional ruler with shorter speeds is located at the nasal part and does not reach the Zyghion points bilaterally. It is not possible to acquire Zy-R – Zi-L measurements directly on the patient's face in this way, and the Beauty Setup® facial ruler will make it possible to measure the linear distances between these two points [6].
Anthropometric Points
Anthropometric points are essential references for taking measurements and understanding facial morphology. The measurement of facial structures contributes to the diagnosis and establishment of adequate therapeutic conduct in OFH, in addition to facilitating communication between professionals. Knowledge of the exact location of points on the facial surface is necessary to obtain accurate and reliable measurements. [2]
Thus, the main anthropometric points for facial harmonization are shown in Table 1.
|
Points |
Initials |
Description |
|
Trichion |
Tr |
A point at on the hairline in the midline of the forehead |
|
Glabella |
G´ |
Most prominent midpoint between eyebrows |
|
Endocanthion |
En |
Inner commissure of palpebral fissure (left and right) |
|
Exocanthion |
Ex
|
Outer commissure of palpebral fissure (left and right) |
|
Pupil |
P |
The black circle in the center of the iris. |
|
Nasion |
N´ |
The midline point of the nasal root and nasofrontal region. |
|
Pronasale |
Prn |
Most prominent midpoint of nasal tip |
|
Nasal Alare |
Al
|
Most lateral point of alar contour (left and right) |
|
Zyghion |
Zy
|
The point of the most lateral soft tissue overlying the zygomatic arch (left and right). |
|
Subnasale |
Sn |
Midpoint of columellar base at junction of upper lip |
|
A´ |
A´ |
The point on the midline of greater concavity in the facial contour of the upper lip, between the subnasale point and the upper lip. |
|
Crista Philtri |
Cph |
The point at each elevated margin of the philtrum just above the vermilion line |
|
Labiale superius |
Ls |
The midpoint of the vermilion line of the upper lip |
|
Stomion |
St |
Midpoint of the labial fissure between gently closed lips |
|
Cheilion |
Ch |
Lateral extent of labial commissure (left and right) |
|
Labialeinferius |
Li |
The midpoint of the lower vermilion line |
|
Gonion |
Go
|
The most lateral point on the mandibular angle (gonial angle). Its location is close to that of the bony gonion. (left and right) |
|
B’ |
B´ |
The point on the midline with greater concavity on the facial contour of the lower lip, located between the lower lip and the soft chin. It is the deepest point of the mentolabial fold. |
|
Pogonion |
Pg′ |
The most anterior midpoint of the chin. |
|
Mento |
Me′ |
The lowest point on the midline of the soft tissue of the chin. This is the lowest point in the measurement of facial height. |
Facial Lines
In addition to the analysis of anthropometric points, it is important to evaluate facial lines. These lines can be vertical and horizontal, and their decompositions are parameters of simple execution, which will assist in the visualization of deviations and asymmetries that are often overlooked during clinical examination [5,12].
One way to detect asymmetries is to measure the distances (Δ) of any pair of points of interest (left and right) in relation to the facial midline. In a symmetrical face, this line will extend through the nasal dorsum and apex to the midpoint of the chin (soft tissue pogonion). The facial midline is parallel to the true vertical or plumb line (Figure 1).
Horizontal reference lines can be constructed by connecting reference points bilaterally.
• Interpupillary line (Line that passes through the pupils)
• Commissure line passing through cheilion-R and cheilion-L.
Ideally, these horizontal lines should be parallel, and they allow us to assess whether they are perpendicular to the facial midline. In this way, it will be possible to visually identify asymmetries that, on clinical examination, sometimes go unnoticed.
MEASUREMENTS
An adequate facial evaluation requires a qualitative and quantitative analysis of the face by a professional. Qualitative analysis allows for an initial and subjective assessment. Conversely, quantitative analysis allows us to adopt a systematic operational form in an objective way with the aid of measurements that will serve as references to provide balance and facial aesthetics [12].
Quantitative facial analysis should be a standardized procedure, with the objective of collecting data and obtaining information regarding the current situation that allows adequate planning for the desired changes. Therefore, these data are not lost, and it is crucial that the analysis be systematized and coordinated.
After obtaining the data, they can be analyzed in two ways: absolute or relative; this analysis will establish proportions between the measurements, which will be compared with those commonly presented in the literature, thus enabling a more careful analysis of the face.
Numerical and proportional measurements between facial structures can be performed during the first contact with the patient through direct linear measurement with the facial ruler in a frontal orientation. These measurements are:
Facial height (Trichion-Mento)
Facial width (Zy-R – Zy-L)
Measure (Go-R – Go-L)
Interpupillary measurement
Interrelationbetween facial thirds
Facial fifths
Figures 4 and 5 illustrate the acquisition of important facial measurements during the first contact with the patient. The greatest facial height is measured by the distance between the anthropometric points Tr-Me shown in Figure 4 (A). The greatest facial width, also called the bizygomatic distance, is measured by the distance between the anthropometric points Zy-R (Zy -right) – Zy-L(Zy-left),as shown in Figure 4 (B). The biogonion distance is measured by the distance between the Go-R (Go-right) – Go-L (Go-left) anthropometric points, as shown in figure 4 (C).
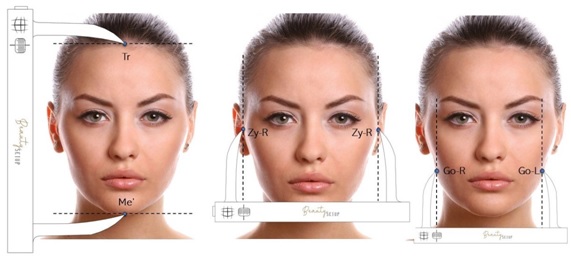
Figure 4: (A) Greater facial height: measure taken between the anthropometric points (Tr-Me 'Tríquio-Mento). (B) Greater facial width. Measure taken between anthropometric points Zy-R - Zy-L bizygomatic distance. (C) Measurement taken between the anthropometric points Go-R - Go-L bigonian distance.
Another reference used as a parameter to predict the measurement of the greatest facial width is related to the interpupillary distance, as shown in figure 5 (A), which must correspond to 50% of the bizygomatic width. [13] However, attention should be paid to variations between intercanthal widths for different ethnic groups, [12] which would be directly related to interpupillary changes. Therefore, the Tr-Me facial distance is a measurement mainly used to assess the greatest facial height. The acquisition of these measurements is an important step in diagnosis and planning. The relationship between them will assist in the interpretation and facial reading of each patient since, in view of an established normative parameter, it is possible to recover facial proportions and make them more similar to the reference, [14] through OFH procedures. As such, there is a greater likelihood of achieving facial balance, considering that the proportion between facial measurements is the guiding premise of these plans.
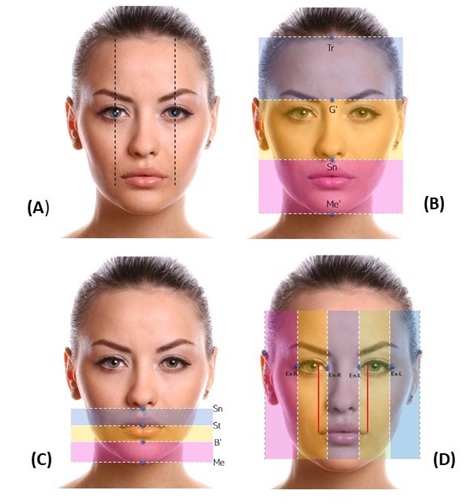
Figure 5: (A) Interpupillary distance. (B) Interrelation between facial thirds. (C) Subdivision of the lower third. (D) Facial fifths.
Interpretation of Facial Proportions
A face with adequate proportions is acceptable, although it is not always beautiful. In the 16th century, Albrecht Dürer explained that although the concept of facial beauty is fundamentally subjective, the evaluation of facial proportions can be carried out objectively. Individuals can vary considerably from the norms of the population but, with the knowledge of the average proportions, a clinician will be able to detect where the differences occur [5].
The proportionality of the facial thirds (Figure 5B) is a very important parameter for facial harmony. Vertically, the face can be divided into thirds of balanced sizes: the upper facial third—from Tr (hairline) to G´, the medium facial third— from G´ to Sn, and the lower facial third—from Sn to Me soft tissue. Vertical proportionality is found when the three-thirds are approximately the same size. [12,14–18].
The facial thirds can be adequately measured with the ruler, placing their rods at the reference points of each third, allowing us to measure and correlate them and making it possible to identify whether there is a deviation in any of these regions. It is noteworthy that it is not always possible to clearly diagnose the presence of a metric change with only a visual observation of the patient's face. Therefore, when positioning the instrument's stems as bulkheads at the ends of the thirds, a better visualization of possible disproportions is noted. In some cases, digital analysis of the patient's frontal photo contributes greatly to this end. This issue will be covered in future studies, including the lateral standard.
More attention should be paid to variations, including those in the lower third of the face, due to the specific repercussions that happen to the soft tissue. For example, especially when the lower third is reduced in cases of loss of the vertical dimension, the aesthetic impact on aging will be negatively increased [14]. The lower facial third can be further subdivided into three other regions, as shown in figure 5 (C) and described below.
• Upper lip (1/3): from the subnasale to the stomion (lip embrasure).
• Lower lip (1/3): from the stomion to the mentolabial groove.
• Chin (1/3): from the mentolabial groove to the chin, defining an ideal proportionality of 1:2 between the height of the upper lip and the height of the lower lip and chin.
The fifth rule, shown in figure 5(D), in turn, is a practical and convenient guideline used to analyze transverse proportional facial relationships. According to this rule, the ideal face can be divided transversely into five equal parts, each approximately equal to the width of the eye, and the width of the base is approximately equal to the intercanthal width. It is worth noting that the inherent ethnic variation in the width of the alar base must be taken into account in diagnosis and treatment planning. [12,19] Another important aspect is that the width of the mouth at rest is approximately equal to the distance between the medial margins of the iris, [5] serving as a reference point adopted to verify whether the width of the mouth is in the desired proportion.
Within the lower third, exposure of the incisors and the interlabial interval are important in assessing face balance. Passive lip sealing reduces the impact of dental or skeletal discrepancies on the face; therefore, it is an important factor to be evaluated [20].
When the height of the upper lip is normal, the exposure of the upper incisors in relation to the upper lip provides an important indication of the vertical position of the maxilla. Therefore, the patient should be evaluated with the mandible in the resting position and with the lips at rest. The ideal dentolabial relationship occurs when the upper lip, at rest, covers approximately two-thirds of the crowns of the incisors, with an exposure of 2-4 mm of the upper incisors, in the presence of the normal height of the upper lip. Women tend to have significantly greater upper incisor exposure compared to men. [12,20] This characteristic is directly related to the youthful appearance of a smile and is expected to decrease throughout life (by stretching of the upper lip due to the maturation and aging processes of the tissues).
An interlabial space greater than 4.0 mm is usually indicative of ineffective lip sealing. Excessive exposure of the upper incisors at rest may be due to vertical maxillary excess and/or supraeruption of the upper incisors [21].
Conversely, in cases with vertical maxillary deficiency, a lower exposure of the upper incisors is observed in relation to the upper lip at rest. In these cases, with the mandible and lips in the resting position, the gingival margins of the upper incisors should be positioned above the lower margin of the upper lip. There is little or no display of teeth during a smile, giving the smile an aged appearance. The adequate interlabial spacing cannot be greater than 2-3 mm. Thus, there is a gradual reduction in exposure of the upper incisor at rest with increasing age. This gradual reduction in exposure is often accompanied by increased exposure of the lower incisor, both at rest and in motion [5,22].
In view of the above information, it is relevant that these measures should be evaluated prior to harmonization procedures, such as lip filling. For faces with vertical defects of the jaws and little exposure of incisors, a lower volume of filling material should be planned since the increase in lip volume further corroborates lower dental exposure, both at rest and when smiling, which is a characteristic of aging. Consequently, treatment alternatives must be offered to the patient first, such as an increase in clinical crowns, facets, or surgeries, including orthognathic or lip lift. Conversely, for more vertical patients where there is no passive lip sealing, lip filling associated with menthol and mentolabial groove favors elevation of the lower lip, thus promoting an improvement in lip posture. It is worth mentioning that these alternatives are associated with the degree of expressiveness of the disproportions. More serious cases should be diagnosed in advance and referred for surgeries, such as orthognathic surgery [5,21].
Practical guide for facial analysis and planning
This work proposes a sequence of eight steps as a service protocol to collect the basic information for good planning and facial analysis dedicated to OFH procedures. All measurements were performed using the Beauty Setup® facial ruler.
- Identification of anthropometric points and the assessment of vertical and horizontal lines (Figure 6).
Step 1: Identify the main anthropometric points used in OFH.
Step 2: The natural position of the head is the reference of choice for taking measurements. The facial midline passes through points G´ and Ls.
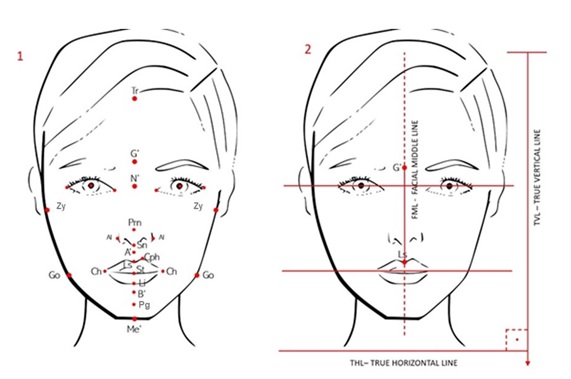
Figure 6: Illustration of steps 1 and 2.
-Height, bizygomatic, and bigonion measurements (Figure 7).
Step 3: With these measurements, relations 1 and 2 are calculated by comparing them with the suggested references, [5] in addition to obtaining the interpupillary measurement. [13]
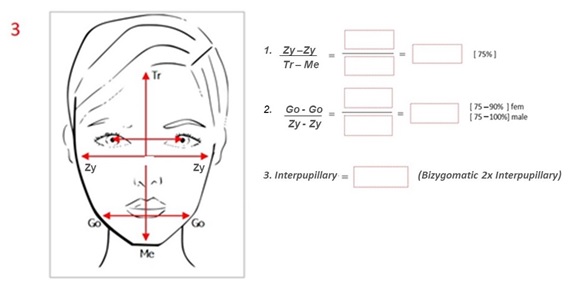
Figure 7: Illustration of step 3 and the values found in this step.
-Measurement of the upper, middle, and lower thirds (Figure 8).
Step 4: Calculate the proportions of the Tr-Me height in each third to obtain items 4, 5, and 6.
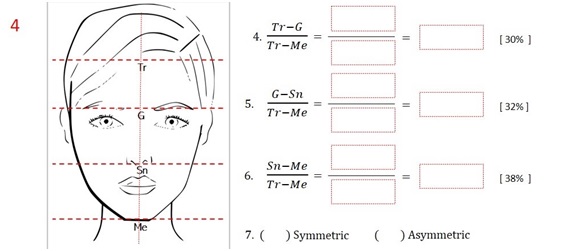
Figure 8: Illustration of step 4 and the values found in this step.
-Lower third of the face (Figure 9).
Step 5: Measure the lower third of the face, including the upper lip, lower lip, chin, and height of the vermilion lip.
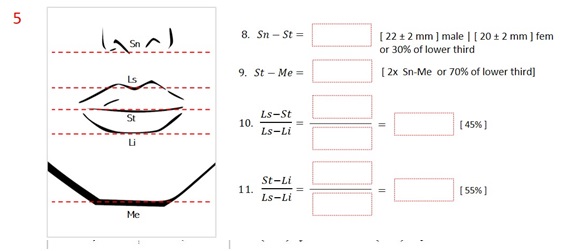
Figure 9: Illustration of step 5 and the values found in this step.
-Transverse relations (Figure 10).
Step 6: Measure the widths of the nasal base and the mouth.
- The width of the nasal base should match the intercanthal distance.
-The width of the mouth should coincide with the medial limbus of the iris in a cross-sectional evaluation.
- Degree of exposure of the upper incisor at rest and when smiling (Figure 10).
Step 7: Exposure of the upper incisor at rest is considered normal when between 2 and 4mm.
Step 8: Dynamics of the smile. Exposure of the upper incisor during a smile is considered normal when it exposes 3/4 of the crown of the upper incisor to 2mm of gum.

Figure 10: Illustration of steps 6 to 8 and the values found in these steps.
Relationship between measures
The relevant indicator of global facial shape is the relationship between vertical facial height and facial width, which is an important measurement to be verified before performing filling procedures [5,12]. The bizygomatic facial width represents the distance between the anthropometric points Zy-R and Zy-L, and it is considered the greatest width of the face.
It is noteworthy that, in a balanced face, the bizygomatic facial width (Zy-R- Zy-L) corresponds to approximately 70-75% of the physiognomic facial height (trichion-mento) [5,12]. In that context, when using this reference during individual planning, this possibility can be identified and the optimal place for volumizing with fillers can be chosen. Therefore, checking this relationship is of great value, in addition to being easy to perform, as it allows us to infer the proportional relationships in each patient beforehand, directing the planning and execution of a more assertive treatment. That is, shorter faces require less volumizing in the zygomatic region in relation to medium, or longer faces.
A large width represents the distance between the anthropometric points Go-R and Go-L; this width is measured from the soft tissue overlying the most lateral point of each mandibular angle (soft tissue). In the classic literature, values between 70-75% of the bizygomatic width are found as a reference for this measurement, suggesting a trapezoidal shape of the face with a bizygomatic width greater than the bigonion width [5,12].
These aspects generate a paradigm shift in relation to the current precepts of beauty, considering that the bigonion distance has become increasingly accentuated in relation to the bizygomatic distance. Recent studies have indicated this tendency in men whose phenotype called “power face” is related to modern facial morphologies that present a relationship between bigonion width and bizygomatic width greater than 81% [23,24]. Contemporary opinions point to a desire for a more pronounced mandibular angle, which may reach a similar proportion between the bizygomatic and bigonion widths for those looking for a masculine and weighted facial appearance. [23–26].
For Arnett and Bergman, [1,2] the exposure of the upper incisors during the smile corresponds to three quarters of the crown height and up to 2 mm of the gum, with exposure being higher in women than in men. This variation in the exposure of teeth when smiling is related to the lip length, the vertical maxillary length, the anatomical length of the crown, and the mobility of the lips when smiling. The evaluation of the degree of exposure of the upper incisor, which may be associated with the vertical position of the anterior part of the maxilla and/or upper teeth, must take into account the upper lip height. Lip height, also called lip length, must be assessed with absolutely linear measurements compared to population norms and by the ratio between the upper and lower lips. Upper lip height comprises the measurement from the subnasale point (Sn) to the point of the upper stomion (Sts), presenting, on average, different values between Caucasian women (20 ± 2 mm) and men (22 ± 2 mm) [5,21].
In relation to the cutaneous part of the upper lip, which corresponds to the distance from the Sn to the Ls, young and harmonious faces always exhibit a short cut height of approximately 9 to 14 mm [22]. Another important aspect to be evaluated is the vermilion of the lips, with the vermilion of the upper lip being less exposed than that of the lower lip. That is, the proportion of the vermilion of the upper lip corresponds to 45% of its total volume, while the proportion of the vermilion of the lower lip is 55%. The correct understanding of these proportions prohibits unsightly outcomes such as “duck mouth” or “fish mouth” during aesthetic procedures that fill the lips [21].
CONCLUSION
Currently, different resources are used to perform facial analysis. The substantial evolution of technology has contributed greatly to advances in computer techniques that produce results that are increasingly attractive and desired. However, direct facial analysis through careful clinical examination remains the primary means of examining the face, in addition to being the most accessible, viable, and least costly resource.
Performing a plan in facial harmonization based on faciometrics parameters and facial proportions makes it possible to develop skills to discern individual characteristics, ensuring more natural and predictable results; planning also increases the accuracy of aesthetic perception. Individualized planning allows the identification of strategic areas of the face with or without the need for volumizing, which will assist in assertiveness and in the optimization of the volume of material to be used.
The systematization of direct facial analysis makes it possible to adopt established references from the literature during a clinical examination in a practical and objective way. Having a well-grounded protocol, combined with easy access to tools, allows faciometrics to be incorporated into clinical practice in a simple and uncomplicated way.
REFERENCES
- Arnett GW. and Bergman RT. (1993). Facial keys to orthodontic diagnosis and treatment planning. Part I.American Journal of Orthodontics and Dentofacial Orthopedics. 103:299–312.
- Arnett GW. and Bergman RT. (1993). Facial keys to orthodontic diagnosis and treatment planning-part II. American Journal of Orthodontics and Dentofacial Orthopedics. 103:395–411.
- El-mangoury NH. and Mostafa YA. (1996). Faciometrics: A new syntax for facial feature analysis.The International Journal of Adult Orthodontics & Orthognathic Surgery;11: 71-82.
- Farkas LG and Deutsch CK. (1996). Anthropometric determination of craniofacial morphology.American Journal of Medical Genetics; 65:1–4.
- Farhad B. Naini. (2014). Estética Facial Conceitos e Diagnóstico Clínicos. 1a ed. Rio de Janeiro: Elsevier. 150-164.
- Ramires RR, Ferreira LP, Marchesan IQ, Cattoni DM, et al.(2010).Adult facial anthropometric measurements according to facial type and gender. Revista CEFAC. 2011;13(2):245-52
- Chiu CSW, Clark RKF. (1991). Reproducibility of natural head position. Journal of Dentistry.19:130–1.
- Cooke MS, Orth D, Wei SHY. (1988). The reproducibility of natural head posture: A methodological study. American Journal of Orthodontics and Dentofacial Orthopedics. 93:280–8.
- Eddo ML, El Hayeck É, Hoyeck M, Khoury É, et al. (2017). La reproductibilité de la position d’équilibre naturel sur photographie. L' Orthodontie Francaise. 88:377–82.
- Moradi A, Watson J. (2015). Current Concepts in Filler Injection.Facial Plastic Surgery Clinics of North America; 23:489–94.
- Bravo-Hammett S, Nucci L, Christou T, Aristizabal JF, et al. (2020). 3D Analysis of Facial Morphology of a Colombian Population Compared to Adult Caucasians.European Journal of Dental.14:342–51.
- Farkas LG. (1994). Anthropometry of the head and face. 2a ed. New York: Raven Press. (1-77).
- Ricketts RM.(1982). Divine proportion in facial esthetics. Clinics in Plastic Surgery. 9:401–22.
- Sarver D, Jacobson RS. (2007). The Aesthetic Dentofacial Analysis. Clinics in Plastic Surgery. 34:369–94.
- Farkas LG, Hreczko TA, Kolar JC, Munro IR. (1985). Vertical and horizontal proportions of the face in young adult North American caucasians: Revision of neoclassical canons. Plastic and Reconstructive Surgery.75:328–37.
- Farkas LG, Katic MJ, Hreczko TA, Deutsch C, et al. (1984). Anthropometric proportions in the upper lip-lower lip-chin area of the lower face in young white adults. American Journal of Orthodontics. 86:52–60.
- Legan H, Burstone C. (1980). Soft tissue cephalometric analysis for orthognathic surgery. Journal Oral Surgery. 38:744–51.
- Worms FW, Isaacson RJ, TM, Speidel TM. (1976). Surgical orthodontic treatment planning: profile analysis and mandibular surgery. Angle Orthodontist. 46.
- Bueller H. (2018). Ideal Facial Relationships and Goals. Facial Plastic Surgery. 34:458–65.
- Seixas MR, Costa-Pinto RA, de Araújo TM. (2011). Checklist dos aspectos estéticos a serem considerados no diagnóstico e tratamento do sorriso gengival. Dental Press Journal of Orthodontics. 16:131–57.
- Camara CA. (2018). Estética em ortodontia - Um sorriso para cada face. 1a ed. Dental Press. 84-126.
- Cornette de Saint Cyr B, Prevot H. (2017). Upper lip lift.Annales de. Chirurgie Plastique Esthétique. 62:482–7.
- Islam S, Taylor CJ, Hayter JP. (2017). Analysis of facial morphology of UK and US general election candidates: Does the ‘power face’ exist?Journal of Plastic, Reconstructive & Aesthetic Surgery. 70:931–6.
- Alrajih S, Ward J. (2014). Increased facial width-to-height ratio and perceived dominance in the faces of the UK’s leading business leaders. British Journal of Psychology. 105:153–61.
- Stirrat M, Perrett DI. (2010). Valid facial cues to cooperation and trust: Male facial width and trustworthiness. Psychology Science. 21:349–54.
- Vazirnia A, Braz A, Fabi SG. (2020). Nonsurgical jawline rejuvenation using injectable fillers. Journal of Cosmetic Dermatology. 19:1940–7.