Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2020
Endobronchial Leiomyoma – When CT Demonstrates the Tumor: A Radio-Pathological Correlation
Diana Penha1,2*, Khoren Abelian1, Gregory Cross3, Erique Pinto2, Edson Marchiori4
1Liverpool Heart and Chest Hospital, Liverpool, UK
2Universidade da Beira Interior, Covilha, Portugal
3Liverpool University Hospitals NHS Foundation Trust, Liverpool, UK
4Universidade Federal do Rio de Janeiro, Brazil
*Corresponding author: Diana Penha, Liverpool Heart and Chest Hospital, Liverpool, UK, E-mail: [email protected]
Received Date: June 29, 2020 Publication Date: December 03, 2020 Copyright: Penha D, et al. ©2020 Citation: Penha D, et al. (2020). Endobronchial Leiomyoma – When CT Demonstrates the Tumor: A Radio-Pathological Correlation. Mathews J Case Rep. 5(1):64.
ABSTRACT
Endobronchial leiomyomas are rare benign tumors, accounting for less than 2% of all benign lung tumors. Known to arise from the smooth muscle of the tracheobronchial tree, leiomyomas occur in parenchymal, endotracheal, or endobronchial locations. Endobronchial lesions constitute about 33% of all pulmonary leiomyomas. Literature on primary endobronchial leiomyomas is extremely limited. Symptomatology depends on the degree of endoluminal bronchial obstruction.
We report a case of 71-year-old woman admitted to our hospital complaining of persistent non-productive cough. Computed tomography (CT) imaging revealed a rounded tumor arising in the right upper lobe bronchus which subsequently underwent bronchoscopy and tissue sampling for definitive treatment. We also describe the cytological characteristics of endobronchial pulmonary leiomyoma.
KEYWORDS: Endobronchial leiomyoma; Chest; Bronchial neoplasms; Cryotherapy; Liquid biopsy
CASE REPORT
A 71-year-old female, presented to our tertiary hospital for investigation of bilateral loss of sight and chronic dry cough, was diagnosed with optic neuritis and treated with steroid treatment. The patient had previous medical history of asthma (since childhood and currently medicated with salbutamol), breast cancer (diagnosed 18 years ago) and melanoma (diagnosed 14 years ago). Both malignancies were submitted to complete surgical resection and no recurrence.
As a part of the diagnostic work-up for a potential underlying paraneoplastic syndrome, the patient underwent a CT scan of the chest, abdomen, and pelvis, which revealed an endobronchial lesion of the proximal right upper lobe bronchus. The patient subsequently underwent flexible bronchoscopy that confirmed a white rounded lesion. Samples were taken and the histological analysis was consistent with a bronchial leiomyoma. After respiratory multidisciplinary meeting discussion, patient was referred for flexible bronchoscopy with cryotherapy. Complete resection of the lesion was achieved, and full patency of the bronchus was restored. Five-year follow-up showed no recurrence of the tumor.
DISCUSSION
Primary leiomyoma is a benign tumor of the smooth muscles. It is common in the uterus, but rare in the smooth muscles of other organs [1-3]. Leiomyomas of the lower respiratory tract can arise from the trachea, bronchi, or lung parenchyma. Clinical presentation depends on the location, size, and effect of the tumor. Severity of presenting symptoms depends on a degree of airway obstruction, presence of bronchiectasis, and an associated history of recurrent chest infections [1,2].
Due to its high sensitivity for the evaluation of the airways, CT documents endobronchial obstruction, the degree of luminal narrowing, location, extension, the presence of adjacent lung tissue involvement (e.g. atelectasis or pneumonitis) and associated mediastinal disease [4,5]. Definitive diagnosis is provided by bronchoscopy with histological analysis [1]. Treatment options of bronchial leiomyomas include endobronchial techniques or surgical resection of lung parenchyma [1,6].
Although infrequent outside the uterus, published cases of primary leiomyomas can be found in the literature involving the esophagus, small bowel, thyroid gland, chest wall, lung, and trachea. Within the lung, about half (51%) of cases affect the parenchyma, with 33 to 45% of cases being endobronchial tumors, the latter found in young or middle age patients with no gender predominance [1]. Leiomyoma metastases affecting the lung parenchyma are even more infrequent [3,6-8].
CT evaluation played a major role in the detection of a 12 x 8mm, rounded lesion, with soft-tissue attenuation (mean of 55 Hounsfield units) of the right main bronchus. The right upper lobe had no atelectasis or consolidation. There was a subtle decrease in the lung density in this lobe likely related to partial compression of the airway and subsequent reduced ventilation. The CT acquisition was repeated after cough maneuver for differential diagnosis with dense mucous plugging, and no change was noticed in the position or shape.
The differential diagnosis for endobronchial lesions is commonly made with benign lesions such as papilloma, lipoma, and hamartoma, with the last two showing fat content [4]. The most common malignant primary lesions presenting as smooth rounded soft-tissue appearance are squamous cell carcinoma, adenoid cystic carcinoma, mucoepidermoid and carcinoid tumors [4]. Also, airway metastases can present as endobronchial lesions, specially from melanoma, breast cancer and genitourinary malignancies [5]. Bronchial metastases from breast cancer or melanoma were two strong consideration included in the differential diagnosis in the reported case since the patient had previous history of these two malignancies in her medical record.
Histologically, endobronchial leiomyomas are identical to leiomyomas seen at other sites, consisting of intersecting fascicles of spindled smooth muscle cells, and having a well-defined border. Cytological atypia, necrosis and mitotic figures numbering more than three per ten high power fields are histological features suggestive of malignancy [9]. In the reported case, the histological appearances were classical with no features of malignancy, and the tumor’s smooth muscle derivation was confirmed with positive immunohistochemical staining for desmin and smooth muscle actin.
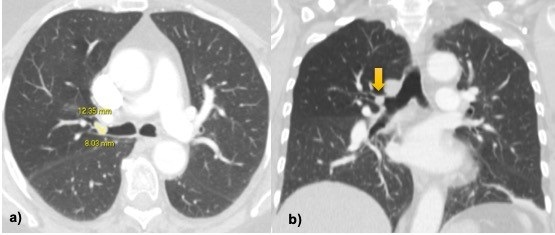
Figure 1: a, b) Axial and coronal images CT show a 12x8mm soft-tissue nodule inside the right main bronchus. There is slight reduction in the density of right upper lobe likely related to decreased pulmonary ventilation but no atelectasis nor consolidations is seen.
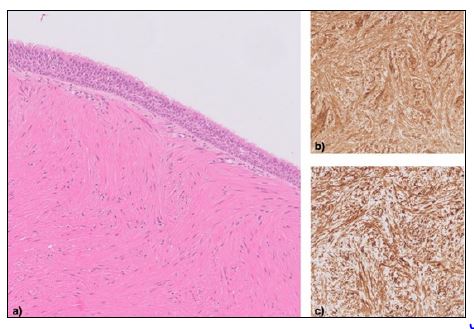
Figure 2: a) Hematoxylin and eosin (H&E) stain shows intersecting fascicles of bland spindle cells with eosinophilic cytoplasm, the appearances consistent with a leiomyoma. The lesion is covered by bronchial epithelium. Immunohistochemistry reveals strong and diffuse expression of smooth muscle actin (b) and desmin (c).
Regardless of the severity of the symptoms or obstructive bronchial features, the treatment of endobronchial leiomyomas, implies resection. Commonly used conservative endoscopic techniques include electrocautery, argon plasma coagulation, cryotherapy, and laser, all with good, documented results [6,10]. In the reported case, the patient showed no evidence of recurrence at a five year follow-up post-cryotherapy.
TEACHING POINT
Endobronchial leiomyoma is a rare entity that can cause non-specific symptoms and go undiagnosed for a long time. CT imaging plays a pivotal role in depicting the endobronchial tumor due to its high sensitivity for airway evaluation, while a final diagnosis requires histological sampling.
AUTHORS' CONTRIBUTIONS
DP - Clinical diagnosis and discussion, conceptualization of case report, KA - Research, writing the case report, references
GC - Research, references, EP - Discussion, case review, EM - Discussion, case review.
ACKNOWLEDGEMENTS
None.
DISCLOSURES
No disclosures.
CONSENT
Yes.
HUMAN AND ANIMAL RIGHTS
Not applicable.
REFERENCES
- Cárdenas-García J, Lee-Chang A, Chung V, Shim C, Factor S, et al. (2014). Bronchial leiomyoma, a case report and review of literature. Respiratory Medicine Case Reports. 12:59-62.
- Swarnakar R, Sinha S. (2013). Endobronchial leiomyoma: A rare and innocent tumour of the bronchial tree. Lung India. 30:57-60.
- Erkiliç S, Erkiliç A, Bayazit YA. (2003). Primary leiomyoma of the thyroid gland. J Laryngol Otol. 117:832‑4.
- Stevic R, Milenkovic B. (2016). Tracheobronchial tumors. J Thorac Dis. 8(11):3401-3413.
- Metta H, Corti M, Redini L, Dure R, Campitelli AM, et al. (2009). Endobronchial leiomyoma : an unusual non-defining neoplasm in a patient with AIDS. Rev Inst Med Trop Sao Paulo. 51(1):53e5.
- Vaza AP, Magalhães A, Bartoschb C, Fernandesc G, Marquesc A. (2011). Primary endobronchial leiomyoma - endoscopic laser resection. Rev Port Pneumol. 17(5):228-231.
- Lorenzoni PJ, Donatti MI, Muller PT, Aguiar ESA, Dobashi PN. (2000). Intrabronchial leiomyoma: report of a case with seven years of tumor evolution. J Bras Pneumol. 26(2):99-102.
- Dossegger JM, Carneiro LH, Rodrigues RS, Barreto MM, Marchiori E. (2019). Pulmonary benign metastasizing leiomyoma presenting as small, diffuse nodules. J Bras Pneumol. 45(4):e20180318.
- Wilson RW, Kirejczyk W. (1997). Pathological and radiological correlation of endobronchial neoplasms: Part I, Benign tumors. Ann Diagn Pathol. 1(1):31‐46.
- Fell CD, Tremblay A, Michaud GC, Michaud GA, Urbansky S. (2005). Electrocauterization of an endobronchial leiomyoma. J Bronchol. 12:181-183.