Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Cytokine-induced Neurogenesis Can Reverse Cognitive Decline in Alzheimer’s Disease
Takuji Shirasawa1*, Luis Carlos Aguilar Cobos2
1Ochanomizu Health and Longevity Clinic, Tokyo, Japan
2Livant Neurorecovery Center, Guadalajara, Mexico
*Corresponding author: Takuji Shirasawa, Ochanomizu Health and Longevity Clinic, Tokyo, Japan; Email: [email protected]
Received Date: March 9, 2023
Publication Date: March 21, 2023
Citation: Shirasawa T, et al. (2023). Cytokine-induced Neurogenesis Can Reverse Cognitive Decline in Alzheimer’s Disease. Mathews J Case Rep. 8(3):97.
Copyright: Shirasawa T, et al. © (2023)
ABSTRACT
Alzheimer’s disease (AD) is a progressive neurodegenerative disease for which no curative treatment has yet been established. We applied cytokine-induced neurogenesis treatment to a 69-year-old female AD patient carrying APOE ε4/ε4 alleles to regenerate residual neuronal stem cells, resulting in the successful regeneration of the atrophied cerebral cortex and hippocampus associated with improved cognitive function and the resolution of electrophysiological abnormalities. To the best of our knowledge, this is the first case report demonstrating that cytokine-induced neurogenesis can reverse cognitive decline due to AD.
Keywords: Alzheimer’s disease (AD), APOE, Cytokine, Neurogenesis, Cognitive decline
INTRODUCTION
Alzheimer’s disease (AD) is a progressive neurodegenerative disease, but no curative treatment has yet been established [1,2]. Regenerative approaches have been extensively researched for AD, but they are still in the early phase of preclinical trials [3]. A recent pathological study, however, clearly showed that neuronal precursor cells were detected in the hippocampus of 18 participants’ brains with a mean age of 90.6 years, including persons with Alzheimer’s disease, suggesting that hippocampal neurogenesis persists in aged and diseased human brains [4]. We explored the possibility that cytokines that induce the differentiation of residual neuronal precursor cells can regenerate atrophied brains with AD and frontotemporal dementia (FTD) and showed that the combination of cytokines successfully regenerates the atrophied hippocampus of patients with AD and FTD [5]. However, clinical symptoms and cognitive functions were not precisely described before and after cytokine cocktail treatment of AD patients [5]. In the present case report, we show evidence that cytokine-induced neurogenesis can reverse cognitive decline in AD patients who are APOE ε4/ε4 carriers.
CASE DESCRIPTION
A 69-year-old housewife developed gradually progressing memory dysfunction with well-preserved language comprehension, emotional control, and orientations in time and place. The Mini-Mental State Examination (MMSE) at the first visit to our clinic on June 12, 2018, indicated cognitive impairment (MMSE 25/30) with mild memory impairment. Emotional control and language comprehension were well preserved. Apoprotein E (APOE) genotype analysis showed that she was an APOE genotype ε4/ε4 homozygous carrier. Cognitive function examination using Cognitrax showed verbal memory impairment, while reaction time, motor speed, sustained attention, cognitive flexibility, executive function, reasoning, and working memory were normal in the assessment performed on June 12, 2018 (Figure 1). MRI data acquired on June 12, 2018, showed moderate atrophy of the cerebral cortex in the parietal lobe and mild atrophy in the frontal and temporal lobes (Figure 2A). A cross-sectional cortical image of the right parietal lobe showed a reduced volume of both gray matter and white matter with an enlarged sulcus (Figure 2C). An in silico endoscopic view from inside the parietal cerebral cortex showed gray matter atrophy with vascular pathologies (Figure 2E). The central part of the anterior left hippocampus showed atrophy (Figure 2G). EEG examination recorded on June 12, 2018, showed slow waves at the frontopolar, frontal, central, and parietal leads at rest (Figure 3A). P300 EEG data analyzed by Neuroscan Software showed that after a target stimulus of high-pitch sound, hyperexcitable premature P300 responses were detected at the frontopolar, frontal, central, parietal, and occipital leads (Figure 3B, red line). The right frontopolar lead showed P300 with a higher voltage of 250 μV2 and a premature peak at 240 msec (Figure 3C, left panel). The left frontopolar lead also showed a similar hyperexcitable and premature P300 (Figure 3C, right panel), suggesting a deficiency in inhibitory GABAergic interneurons in the frontal, temporal, parietal, and occipital lobes, as described previously [5]. P300 also showed asymmetries at the frontolateral leads between F7 and F8 and reduced voltage in temporal anterior leads between T3 and T4 (Figure 3B). Coherence analysis of P300 indicated that frontolateral leads showed asymmetries and the occipital leads showed high values and low fluctuation (data not shown). Flash visual evoked potentials showed moderate dissociation between FP1 and PF2 leads and advanced dissociation between F7 and F8 leads (Figure 3C, left panel), suggesting that vascular pathologies were also involved in the pathology of the frontopolar and frontolateral cerebral cortex. Blood chemistry, CBC, thyroid function, and HbA1c, however, failed to indicate any disorder associated with dementia. We, therefore, diagnosed this patient as having typical AD and carrying APOE ε4/ε4 alleles based on clinical symptoms, morphological abnormalities, and electrophysiological abnormalities, which are compatible with global ß-amyloid (Aß) deposition in the cerebral cortex.
We therapeutically applied a cytokine cocktail containing HGF (hepatocyte growth factor), GCSF (granulocyte colony stimulating factor), adiponectin, IGF-1 (insulin-like growth factor-1), and IGF-2. The clinical protocol used in this study as well as the cytokine cocktail formulation was designed and developed by Luis Carlos Aguilar Cobos in the Livant Neurorecovery Center, Mexico, as described previously [5]. On Jan 30, 2019, six months after cytokine cocktail treatment, the patient’s verbal memory function, which had declined previously, recovered with a concomitant improvement in MMSE score from 25/30 to 27/30 (Figure 1). We then continued cytokine-induced neurogenesis treatment for nearly 2 years until July 10, 2020. The patient’s cognitive functions further improved along with working memory, verbal memory, attention, reaction time, motor speed, and reasoning, while cognitive flexibility and executive function were maintained with an MMSE score of 27/30, as illustrated in Figure 1. We reevaluated the patient’s EEG signals on July 10, 2020, which showed a significant decrease in slow waves (Figure 3A). P300 EEG responses were significantly suppressed in all brain areas, including the frontal, temporal, parietal, and occipital lobes (Figure 3B, black lines), suggesting that inhibitory GABAergic interneurons were regenerated globally to suppress the hyperexcitable P300 responses evoked by glutamatergic neuronal activities observed before treatment, as suggested previously [5]. Higher magnification of P300 responses in the left frontopolar leads clearly showed that the premature response at 240 msec with 250 µV2 observed before treatment significantly improved to a normal P300 response at 550 msec with 50 µV2 after treatment (Figure 3C, left panel). A similar improvement was observed at the right frontopolar leads (Figure 3C, right panel). The dissociations of flash visual evoked potentials observed between FP1 and FP2, or F7 and F8 on June 12, 2018, significantly improved on July 10, 2020 (Figure 3D), indicating that cytokine-induced neurogenesis was physiologically relevant for the processing of visual stimuli. We performed MRI on July 10, 2020, which showed a slight increase in the volume of the atrophied gyrus in the parietal cortex after treatment (Figure 2B). The cut surface image of the recovered gyrus showed enlarged gray matter and white matter with an enlarged gyrus (Figure 2D). Vascular pathologies detected on June 12, 2018, disappeared in an endoscopic view in silico of the same cortex recorded on August 18, 2022 (Figure 2F). Another endoscopic view in silico showed that the atrophied left hippocampus was significantly regenerated with a tiny dent in the anterior part of the hippocampus after treatment (Figure 2H), which is clinically compatible with recovered memory functions (Figure 1). The patient was then followed up for 14 months without cytokine treatment and showed preserved cognitive function with an MMSE score of 26/30 on September 18, 2021, without developing further declines in cognitive functions such as memory, language comprehension, emotional control, and orientations with time and place.
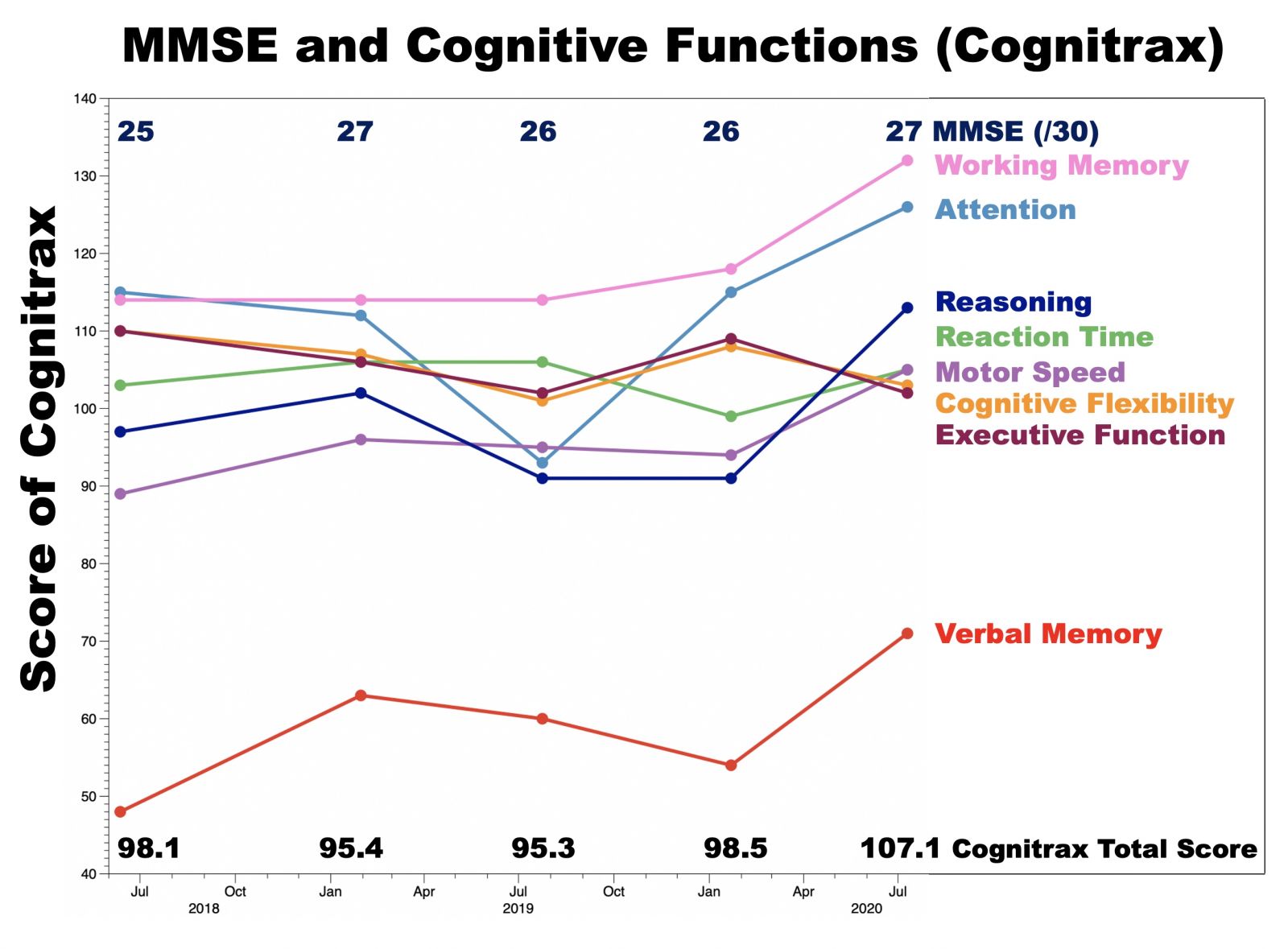
Figure 1: MMSE and cognitive functions before and after cytokine-induced neurogenesis.
Cognitive functions were evaluated by CognitraxR and the Mini Mental State Examination (MMSE) on June 12, 2018; Jan 30, 2019; July 24, 2019; Jan 22nd, 2020; and July 10, 2020. The MMSE scores are annotated in the upper part of the graph. Cognitrax scores for working memory (magenta), attention (light blue), reasoning (dark blue), motor speed (plum), cognitive flexibility (yellow), executive function (brown), and verbal memory (red) are chronologically illustrated as line graphs with different colors.
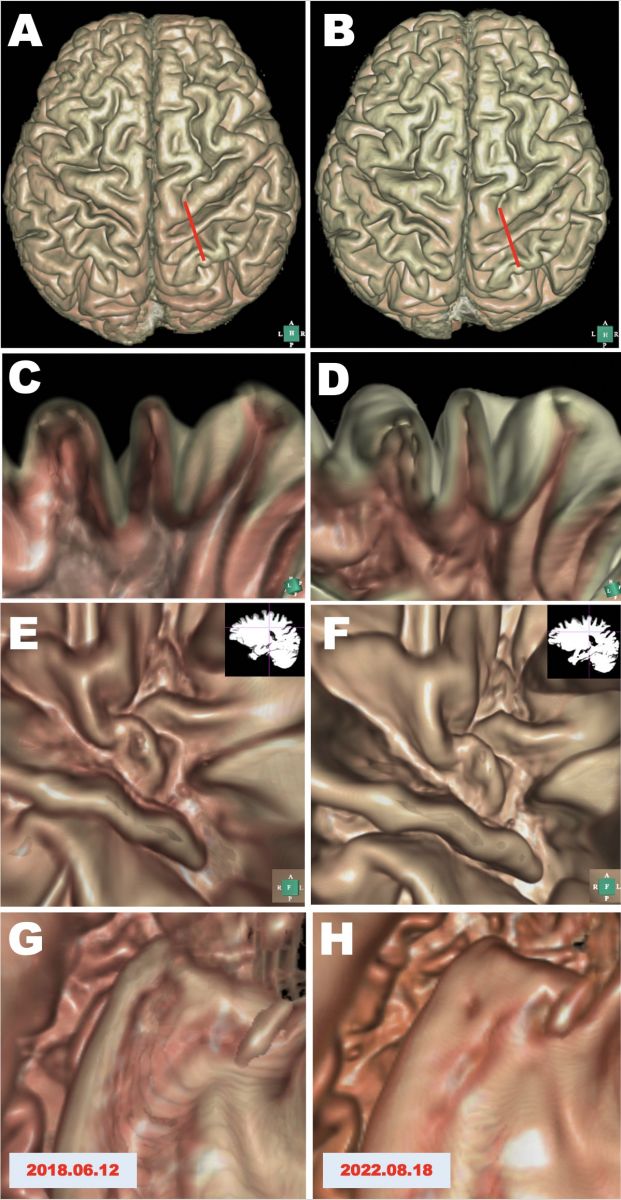
Figure 2: Morphological evaluations before and after cytokine-induced neurogenesis.
MRI scans on June 12, 2018, and on August 18, 2022, before and after cytokine cocktail treatment. A, B. 3D structure of the cerebral cortex reconstructed in silico using Expert INTAGER software from MRI T1-weighted images with 1 mm sagittal slices before and after cytokine cocktail treatment. C, D. Cut surface images of the parietal lobe as indicated by red lines in A and B show the regeneration of the atrophied cerebral cortex. E, F. Endoscopic views in silico of the parietal lobes of the cerebral cortex from inside the white matter. The position (red lines) and view angle (green line) of the endoscopic camera are indicated in the upper right insets. G, H. Endoscopic views in silico of the left hippocampus show the regeneration of the atrophied left hippocampus after cytokine cocktail treatment.
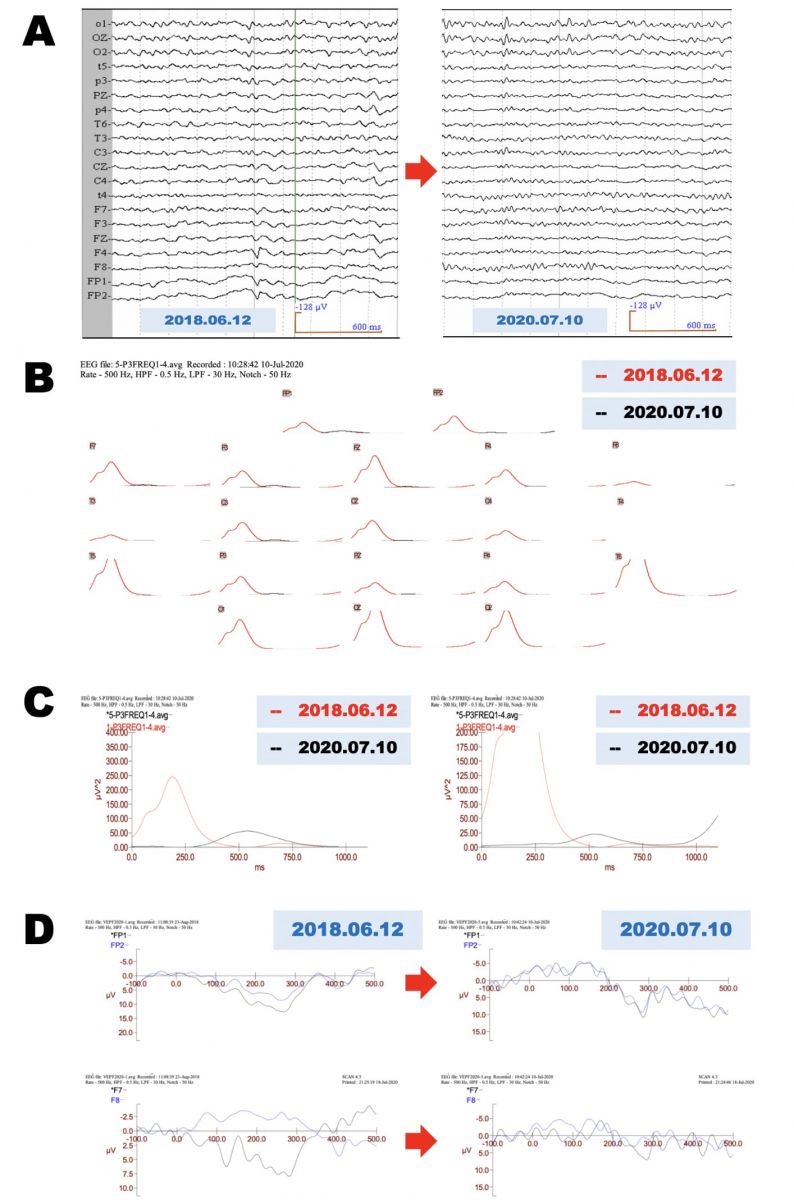
Figure 3: Neurophysiological evaluations before and after cytokine treatment.
A. Electroencephalogram (EEG) recorded on July 10, 2018, and July 10, 2020. B. Electrophysiological evaluation of P300 EEG responses before and after cytokine-induced neurogenesis. Before treatment, P300 EEG responses recorded on June 12, 2018, are shown as red lines, and EEG responses recorded on July 10, 2020, after treatment P300, are shown as black lines. C. Magnified recordings of frontopolar leads of Figure 3A show that the premature hyperexcitability recorded on June 12, 2018 (red lines) significantly improved in both frontopolar leads recorded on July 10, 2020 (black lines; left, left frontopolar leads; right, right frontopolar leads). D. Electrophysiological records of flash visual evoked potentials before and after cytokine treatment. Asymmetrical potentials recorded on June 12, 2018, with FP1 (left frontopolar leads, black line) and FP2 (right frontopolar leads, blue line) improved on July 10, 2020 (right upper panel). Asymmetrical flash visual evoked potentials recorded on June 12, 2018, with F7 (left frontolateral leads, black line) and F8 (right frontolateral leads, blue line) significantly improved on July 10, 2020 (right lower panel).
DISCUSSION
In the present case report, we demonstrated for the first time that cytokine-induced neurogenesis not only regenerates the hippocampus of AD patients with APOE ε4/ε4 carriers but also regenerates the atrophied cerebral cortex and hippocampus associated with the reversal of various aspects of cognitive decline, such as working memory, verbal memory, attention, and reasoning. Neurophysiological studies clearly showed that inhibitory GABAergic neuron networks were impaired in the cerebral cortex (Figure 3B and 3C). Cytokine treatment induced the neurogenesis of inhibitory GABAergic neurons, which then suppressed the hyperexcitability of glutamatergic pyramidal neurons (Figure 3B and 3C). Additionally, GABAergic neurons were reported to constitute the niche of neuronal stem cells in the hippocampus, which plays an important role in adult neurogenesis [6-8]. It is then reasonable to speculate that neurogenesis of inhibitory GABAergic neurons regenerates the functional niche that supports neuronal stem cells in the brains of AD patients. To eliminate ß-amyloid (Aß) deposition in the brains of AD patients, we applied GCSF and IGF-1, which were reported to activate microglial cells that can degrade Aß deposition in the cerebral cortex as well as the hippocampus in animal models [9-10]. Interestingly, the AD case reported here showed that the reversal in cognitive function was maintained without further neurogenesis for more than 14 months, suggesting the possibility that Aβ was degraded by cytokines, such as GCSF and IGF-1. We are still in the early phase of the clinical application of cytokine-induced neurogenesis for AD, but so far, we have administered cytokine cocktail treatment to 15 patients with AD who were APOE ε4/ε4 carriers; we confirmed neurogenesis for all AD patients even in those in advanced stages [5]. To our knowledge, cytokine-induced neurogenesis is the most promising clinical strategy to cure AD.
CONCLUSION
AD is a progressive neurodegenerative disease for which no curative treatment has yet been established. This is the first case report demonstrating that cytokine-induced neurogenesis can reverse cognitive decline due to AD. In this case report, we explored the possibility that cytokine-induced neurogenesis would be a novel promising strategy to cure AD.
ACKNOWLEDGEMENTS
The authors would like to thank Ms. Sayuri Sato, Ms. Masami Fukuda, and Ms. Fernanda Diaz for the preparation of this manuscript.
ETHICAL APPROVAL OF STUDIES AND INFORMED CONSENT
Written informed consent was obtained from the patient and her son.
CONFLICT OF INTEREST
The authors have no conflicts of interest.
REFERENCES
- Masters CL, Bateman R, Blennow K, Rowe CC, Sperling RA, Cummings JL. (2015). Alzheimer's disease. Nat Rev Dis Primers. 1(1):15056.
- Knopman DS, Amieva H, Petersen RC, Chételat G, Holtzman DM, Hyman BT, et al. (2021). Alzheimer disease. Nat Rev Dis Primers. 7(1):33.
- Essa H, Peyton L, Hasan W, León BE, Choi DS. (2022). Implication of Adult Hippocampal Neurogenesis in Alzheimer's Disease and Potential Therapeutic Approaches. Cells. 11(2):286.
- Tobin MK, Musaraca K, Disouky A, Shetti A, Bheri A, Honer WG, et al. (2019). Human Hippocampal Neurogenesis Persists in Aged Adults and Alzheimer's Disease Patients. Cell Stem Cell. 24(6):974-982.
- Shirasawa T, Cobos LCA. (2022). Cytokine-induced Neurogenesis for Alzheimer’s Disease and Frontotemporal Dementia. Personalized Medicine Universe. 11(1):27-32.
- Urban N, Guillemot F. (2014). Neurogenesis in the embryonic and adult brain: same regulators, different roles. Front Cell Neurosci. 8(1):1-19.
- Gonzalez-Ramos A, Waloschkova E, Mikroulis A, Kokaia Z, Bengzon J, Ledri M, et al. (2021). Human stem cell-derived GABAergic neurons functionally integrate into human neuronal networks. Sci Rep. 11(1):22050.
- Li Y, Guo W. (2021). Neural Stem Cell Niche and Adult Neurogenesis. Neuroscientist. 27(3):235-245.
- Guo X, Liu Y, Morgan D, Zhao LR. (2020). Reparative Effects of Stem Cell Factor and Granulocyte Colony-Stimulating Factor in Aged APP/PS1 Mice. Aging Dis. 11(6):1423-1443.
- Li C, Chen YH, Zhang K. (2020). Neuroprotective Properties and Therapeutic Potential of Bone Marrow-Derived Microglia in Alzheimer's Disease. Am J Alzheimers Dis Other Demen. 35(1):1533317520927169.