Information Links
Related Conferences
Previous Issues Volume 9, Issue 4 - 2024
Carbohydrate Nutrition and Glucose Homeostasis – Type 2 Diabetes
Vincent O Obinna1,*, Justina K Anozie1
1Department of Food Technology, Akanu Ibiam Federal Polytechnic, Unwana Ebonyi State Nigeria
*Corresponding Author: Vincent O Obinna, Department of Food Technology, Akanu Ibiam Federal Polytechnic, Unwana Ebonyi State Nigeria; Tel: +234 (0)703 448 6378; Email: [email protected]
Received Date: January 6, 2024
Publication Date: March 20, 2024
Citation: Obinna VO, et al. (2024). Carbohydrate Nutrition and Glucose Homeostasis – Type 2 Diabetes. Mathews J Case Rep. 9(4):161.
Copyright: Obinna VO, et al. © (2024)
ABSTRACT
Diabetes is a major metabolic, non-communicable disease, threatening human health all over the world. The disease was formally regarded as ‘disease for the affluent’ but its prevalence in low and medium income economies has changed this perception. Types 1 and 2 have been identified as the major types of diabetes with prediabetes and gestational diabetes as pointers to T2DM. In all the types identified, insulin secretion and glucose absorption are central to them all. This research reviewed carbohydrate nutrition and glucose homeostatsis and depended majorly on PubMed and IDF publications. It was discovered that in 2013, China had 98.4 million cases while Japan had 7.2 million to become the highest and lowest, respectively, among the first ten countries with the highest prevalence of diabetes, globally. It is however projected that in 2035, Africa will comparatively top the world list with an unprecedented increase by 109.1%. An improved lifestyle and careful selection of food consumption have however, been identified as major panacea to forestalling the imminent complications of diabetes and the prevalence of this disease condition. A successful control of the spread of T2DM would have saved the world lots of deaths and funds.
ABSTRACT
Diabetes is a major metabolic, non-communicable disease, threatening human health all over the world. The disease was formally regarded as ‘disease for the affluent’ but its prevalence in low and medium income economies has changed this perception. Types 1 and 2 have been identified as the major types of diabetes with prediabetes and gestational diabetes as pointers to T2DM. In all the types identified, insulin secretion and glucose absorption are central to them all. This research reviewed carbohydrate nutrition and glucose homeostatsis and depended majorly on PubMed and IDF publications. It was discovered that in 2013, China had 98.4 million cases while Japan had 7.2 million to become the highest and lowest, respectively, among the first ten countries with the highest prevalence of diabetes, globally. It is however projected that in 2035, Africa will comparatively top the world list with an unprecedented increase by 109.1%. An improved lifestyle and careful selection of food consumption have however, been identified as major panacea to forestalling the imminent complications of diabetes and the prevalence of this disease condition. A successful control of the spread of T2DM would have saved the world lots of deaths and funds.
INTRODUCTION
Several research efforts have identified diabetes as a major metabolic, non-communicable disease, threatening human health all over the world (Chen et al., 2010, McCarthy, 2010, Nolan et al., 2011, Tahrani et al., 2011, Kurotani et al., 2013) [1-5]. Diabetes is linked to diet, genetics, lifestyle, ageing, income and environmental factors (Chen et al., 2010, Anjana et al., 2011, Hu, 2011, Basu et al., 2013) [1,6-8]. Chen et al (2010) [1] argue that families with the history of this metabolic disease have a higher prevalence of type 2 diabetes. Its prevalence in developing countries is particularly pathetic (Hu, 2011, IDF, 2013) [7,9]. At present, researchers have discovered three types of diabetes namely, type 1 (T1DM), type 2 (T2DM) and gestational diabetes (GDM) with prediabetes signalling the imminence of T2DM (Salas-Salvadó et al., 2011) [10]. The T1DM, an autoimmune disease (Gajos et al., 2013) [11], is insulin dependent while T2DM is non-insulin dependent (Catalano, 2010) [12] gestational diabetes (GDM) and prediabetes are pointers to the possibilities of developing T2DM (Petry, 2010, Anjana et al., 2011) [6,13]. It is difficult to ascertain the exact time T2DM starts (Forouhi and Wareham, 2010) [14]. Kim et al (2010) [15] assert that 15.4% of GDM cases are as a result of overweight, 9.7% due to obesity and 21.1% due to extreme obesity. Whichever form it might present itself, it has always culminated into having excess sugar in the human blood (Tahrani et al., 2011) [4]. Statistical evidence abound that diabetes are common in those aged >40s (UK, 2013) [16], but recently, it has also been observed in children (Sabin, 2012, Reinehr, 2013) [17,18]. Reinehr (2013) [18] observed that T2DM has become so noticeable in children and adolescents in, the mid-1990s, and this he has attributed to possible increased secretion of growth hormone, which impairs the secretion of insulin. The gestational diabetes is often ephemeral and would likely go off soon after delivery; it may, however, possibly be an indication of the possibility of the carrier developing full blown diabetes in the nearest future, but this is not always the case (Catalano, 2010) [12].
Figure 1 shows that under normal circumstances, the capillary blood glucose (CBG) should be 5mMl-1 (90mg/dl) but in diabetic conditions the CBG increases to ≥7 mMl-1 (≥126 mgdl-1) and ≥12.2 mMl-1 (≥220 mgdl-1), 2 hours after glucose meal. Another condition, impaired fasting glucose (IFG), exists when CBG ≥6.1 mMl-1 (≥110 mgdl-1) and <7 mMl-1 (<126 mgdl-1), and 2 hours after that <8.9 mMl-1 (<160 mgdl-1). Also, impaired glucose tolerance (IGT) exists when after 2 hours the CBG is ≥ 8.9mMl-1 (≥160mgdl-1) but <12.2mMl-1 (<220mgdl-1) and upon fasting, <7mMl-1 (<126mgdl-1). Both IFG and IGT define a prediabetes condition (Anjana et al., 2011, Reinehr, 2013) [6,18].
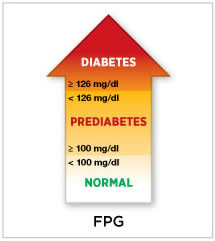
Figure 1: Fasting Plasma Glucose showing normal and various levels of diabetes conditions. ADA http://www.diabetes.org/diabetes-basics/diagnosis/
In the UK, over three million people had been diagnosed with diabetes and about 850,000 undiagnosed cases whereas, in the USA, on a daily basis, about 1,700 new cases are diagnosed. Unfortunately, there are yet, so many other people with undiagnosed diabetes and so these numbers could be increasing (UK, 2013) [16]. Cases and prevalence rate in other economies abound. This staggering number of cases no doubt places much pressure on the economy in funding treatment, loss of man hour, and in extreme cases, death (Roglic and Unwin, 2010, Reinehr, 2013) [18,19]. Self-care was designed through the UK’s National Service Framework for Diabetes by the Department of Health in 2001 (Booth et al., 2008) [20].
A total of 285 million were diagnosed with diabetes in 2010, and almost 75% of this number was in low and middle-income economies thereby jettisoning the earlier postulation that diabetes was a disease for the affluent. It is a major concern that the projection is that, in 2030, in developing economies, the number of people with diabetes would have risen by 69%, and this will certainly outnumber those in developed economies (Basu et al., 2013) [8]. Basu et al (2013) [8] also observed that a wrong approach such as sedentary lifestyles, which promotes obesity, has been the bane of the disease in developing economies.
At present, management of diabetes is more emphasised rather than cure, as efforts are still progressing to discover affordable and accessible cure for diabetes (Mingrone et al., 2012) [21]. The management of this condition has become necessary to prevent complications which either could be short or long term resulting in renal or kidney failure, cardiovascular diseases, and in extreme cases, death (Roglic and Unwin, 2010) [19].
Carbohydrate nutrition
Carbohydrate food sources constitute about 80% of the energy source of the low income group in the tropics and 40% energy source for the rich in many countries. This, therefore, re-defines the earlier traditional thoughts that carbohydrate was just an energy source but has now taken its rightful place as an essential food component (Englyst and Hudson, 2003, Henry and Ahlstrὂm, 2009) [22,23]. Absorption of the digested glucose in the small intestine, as well as the fermentation at the large intestine, determines the physiological effect of dietary carbohydrate.
Englyst and Hudson (2003) [22] affirm that digestion of carbohydrate foods start from the mouth where it is masticated. In this brief moment, amylase (ptyalin) in saliva mixes with the food and digestion is initiated. This mix makes for easy passage through the oesophagus, and the activities of the amylase are terminated in the stomach by gastric acid, and the bolus is further broken down before getting into the small intestine, where digestion by the pancreatic α-amylase hydrolyses the starch into dextrin and disaccharide molecules.
The activities of glucosidases in the intestinal epithelium brush border reduce dextrin and disaccharides into their constituent monosaccharides: glucose, fructose and galactose. These simple sugars are then transported to the portal vein through the epithelial cells. Glucose and galactose are absorbed faster than fructose. The glucose is then dispensed of either by insulin to the cells or direct to non-insulin dependent tissues (Schwartz et al., 2013) [24].
Glucose homeostasis
Energy supply to the body and especially the brain is majorly sourced from glucose and so its balance in the body must be maintained (Hong et al., 2013) [25] further asserted that glucose homeostasis is important and that any failure could result to an imbalance, which could manifest as T2DM.
Menge et al (2011) [26] observed that ‘‘glucagon and insulin are secreted in a coordinated pulsatile manner’’. This, therefore, implies that the secretion of insulin suppresses the secretion of glucagon but this relationship is disrupted in T2DM, which could result in glucagonemia.
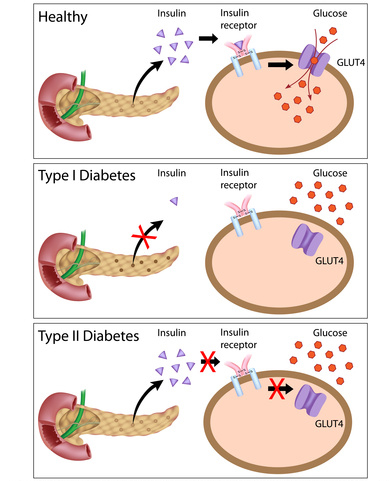
Figure 2: glucose metabolism in normal, T1DM and T2DM Source: http://sciencetuition.co.uk/diabetes/.
Figure 2 shows the three possible states in glucose homeostasis – normal, T1DM and T2DM. The pancreas detects an increase or otherwise of blood glucose. So after glucose had been absorbed into the blood, the pancreas secretes insulin from the β-cells to reduce the glucose level. The β-cells achieve this by transporting the glucose molecules into the cells (Hong et al., 2013) [25]. When 5mM/l in the blood is attained, the surplus is transported to the liver and skeletal muscles, where they are converted to glycogen (Schwartz et al., 2013) [24].
When there is a drop of glucose level in the blood, the α-cells will be released by the pancreas (Hong et al., 2013) [25]. The α-cells then breaks down the stored glycogen from the liver and muscle and release them to the blood as glucose, which is then transported to the cells where they are utilised for the production of energy (Hong et al., 2013) [25].
Figure 3 further illustrates that when insulin is secreted from the pancreas, there will be a decline in glycogenesis; the skeletal muscles would be more disposed to absorb more glucose and yet inhibit the release of fatty acid from the adipose tissues. All the factors that promote T2DM influence both the secretion and actions of insulin. A decline in the secretion of insulin reduces its signalling effect on the target tissues and this would give rise to increase in both fatty acids and glucose in the blood. This development would in turn worsen both the secretion and resistance of insulin.
T1DM results when the pancreas could not produce insulin despite the presence of glucose in the blood (Sabin, 2012) [17].
.png)
Figure 3: The relationship between the increase in blood glucose and fatty acids in T2DM (Stumvoll et al., 2005) Source: Stumvoll, M.; Goldstein, B. J. and van Haeften, T. W. (2005). Type 2 diabetes: principles of pathogenesis and therapy. Lancet; 365: 1333–1346
In T2DM, when glucose is absorbed into the blood after digestion, the pancreas releases insulin but the insulin would not transport the glucose from the blood into the cells for the production of energy (Reinehr, 2013) [18]. This could be due to either or all of these – multiple metabolic defects, β-cells dysfunction, insulin resistance and/or abnormal regulation of glucagon (Menge et al., 2011) [26].
Long-term complications
Depression, hypertension, dyslipidemia, polycystic ovarian syndrome, or acan- thosis nigricans, end-stage renal disease, loss of visual acuity and limb amputation (Reinehr, 2013, Siddiqui, 2013) [18,27] have been identified as possible complications of T2DM. Others are cancer, cardiovascular diseases, liver pathologies, and inflammatory diseases (Park et al., 2014) [28]. Ferland-McCollough et al (2010) [29] also identified heart diseases, stroke, kidney failure, blindness and nerve damage as other possible complications.
Worldwide Prevalence of Type 2 Diabetes
IDF 2013 asserts that, in 2013, the number of people with diabetes across the world was about 382 million and about an additional 175.72 million undiagnosed cases, which is 46% of the identified cases. A total of 592 million cases are anticipated in the year 2035; this gives an increase of 55% (about 325.6 million cases) anticipated within the period. Diabetes has eaten into the economy of nations with about USD548 billion spent in 2013 across the world and USD 627 billion estimated in managing diabetes in 2035 globally. It is reported that, in 2013 alone, about 5.1 million people died, and this means that one person died every six (6) seconds across the globe (IDF, 2013) [9]. If the trend continues, in 2035, about 13.4 million people would have died due to diabetes (Figure 7).
The worst affected region (countries and territories) is in the Western Pacific, which recorded 138 million cases in 2013 and would by 2035 have recorded 201.48 million cases by current projections, an increase by 46%. It is anticipated that Africa would experience a very rapid increase from 20 million in 2013 to 41.83 million cases in 2035, which is an increase of 109.1%. In Figure 4 the statistics for other regions are presented (IDF, 2013) [9].
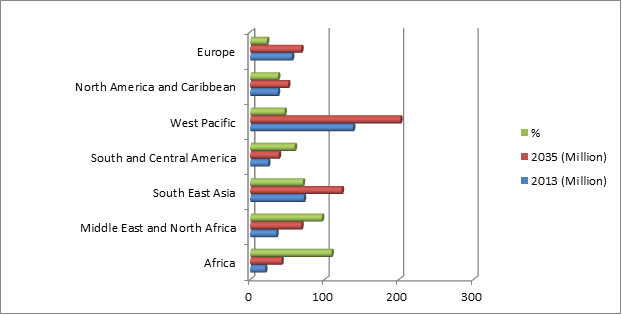
Figure 4: Number of people with diabetes by IDF Region diabetes (20 – 79 years), 2013 with estimate for 2035. Adapted from: IDF Diabetes Atlas 2013 6th ed., 11- 12
IDF 2013 [9] reported that China topped the world list with 98.4 million cases of diabetes (Figure 5). However, in terms of comparative prevalence, Figure 6 shows that Tokelau was at the top with 37% of the entire population diagnosed with diabetes.
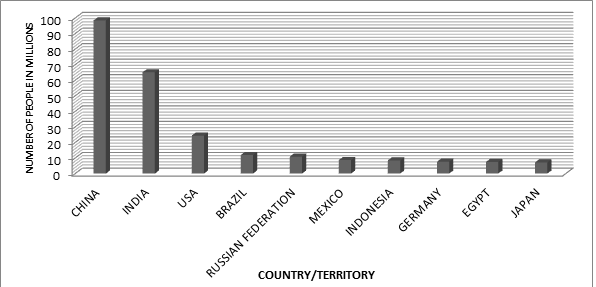
Figure 5: The top 10 countries with the highest number of diabetes cases across the world (20 – 79 years). Adapted from: IDF Diabetes Atlas 2013 6th ed., 13. China tops the list with 98.4 million cases while Japan recorded 7.2 million to come 10th.
It is arguable that diabetes has impoverished the world economy and undoubtedly, the worst hit is the developing economies (Shaw et al., 2010) [30]. Unfortunately, the available data are not even the true position of this plague, since there are millions of cases either not reported or undiagnosed (Forouhi and Wareham, 2010) [14].
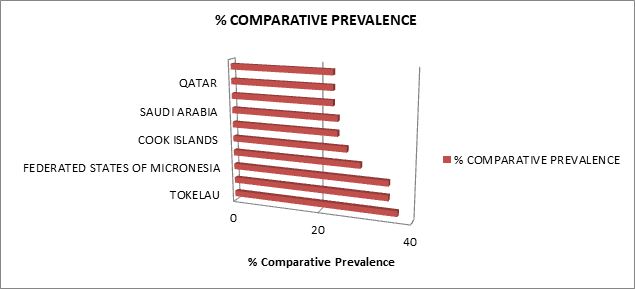
Figure 6: Top 10 countries/territories for prevalence (%) diabetes (20 – 79 years), 2013. Adapted from: IDF Diabetes Atlas 2013 6th ed., 13. Tokelau tops the list with 37% of the population diagnosed with diabetes while Qatar is the 10th most prevalent with 23% of the population having diabetes.
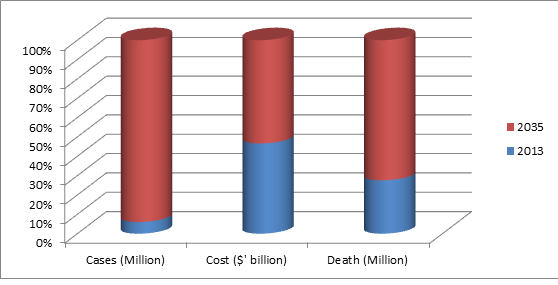
Figure 7: Prevalence, cost and deaths across the world due to diabetes. Adapted from IDF 2013 6th ed 11 – 12.
Prevalence of diabetes in Nigeria
The statistics available for Nigeria showed that in 2013, there were about 3,992,000 diagnosed cases, which is about 5.82% of the entire population. About USD 137.00 was purportedly spent on each case, resulting in total of about USD 547 million (IDF, 2013) [9]. The total budget of Nigeria for 2013 was USD 31.63 billion (NGN4.99 trillion) (Office, 2013) [31], diabetes alone took about 1.73% of the total budget. Nevertheless, this information about Nigeria may not be totally correct given to poor record keeping culture and poverty that may not even allow the patient to go to the hospital.
Gajos et al (2013) [11] postulated that change in life style with more of sedentary living has led to increased obesity cases and hence, type 2 diabetes. This position has been supported by several research reports including those of (Kahn et al., 2011, Whiting et al., 2011, Basu et al., 2013) [8,32,33].
Influence of change in life style and prevalence of T2DM in the over weight
Several authorities have alluded to the fact that overweight and obesity are major threats to diabetes. It is confirmed that body mass index (BMI) of 18.5 – 24.9 ‘is considered normal’ while a BMI of 25 – 29.9 is adjudged overweight; conditions of obesity and extreme obesity has 30 – 39.9 and > 40, respectively. One is considered underweight if the BMI is < 18 (Brian et al., 2011, Cheong et al., 2013) [34,35]. Overweight has been key to the prevalence of impaired glucose intolerance (IGT) and hence T2DM (Scheen and Gaal 2014; Saas-Salvadό et al 2011; Tahrami et al 2011) [4,10,36]. Scheen and Gaal (2014) [36] argued that about 80% of T2DM could be traced to these two factors (overweight and obesity). Similarly, Donin et al (2014) [37] described obesity as the precursor of T2DM. Prevention of weight gain and facilitating weight loss would be effective in controlling the prevalence of T2DM (Salas-Salvadó et al., 2011, Scheen and Van Gaal, 2014) [10,36]. Also, a change in dietary formulation that will ensure low glycemic index (GI), low glycemic load (GL) and low insulin level (II) would make any weight management effort more meaningful (Esfahani et al., 2014) [38].
Mild and consistent physical exercise, which could help in losing 5% - 10% of the body weight (Wing et al., 2011, Wasserman et al., 2011, Oliveira et al., 2012) [39-41]suggested that a daily 15 minutes or a total of 92 minutes per week, moderate exercise would help those with cardiovascular disease. Hu (2011) [7] opines that 30 minutes of moderate to vigorous exercise a day would suffice. Also, avoidance of smoking and half serving of alcoholic beverage per day would be helpful (Acheson, 2010, Hu, 2011) [7,42]. A remarkable reduction in the risk by the overweight is possible with consumption of cereal fibre and polyunsaturated fat but dependence on food with higher glycemic index and trans fat could increase the risk (Hu, 2011) [7]. A change in lifestyle (involving weight loss through structured exercises and change in diet) resulting in 58% reduction, in risk of T2DM, has been reported (Salas-Salvadó et al., 2011) [10].
CONCLUSION
‘‘Imported sugars deserve further investigation as a potential population-level driver of global diabetes’’ (Basu et al., 2013) [8]. Medical intervention in the treatment and management of T2DM has proven ineffective since some of the formulations promote weight gain (Scheen and Van Gaal, 2014) [34]. The use of structured physical exercise, change in lifestyle and diet promise to be more effective in combatting this scourge.
REFERENCES
- Chen Y, Rennie DC, Dosman JA. (2010). Synergy of BMI and family history on diabetes: the Humboldt Study. Public Health Nutr. 13(4):461-465.
- Mccarthy MI. (2010). Genomics, Type 2 Diabetes, and Obesity. New England J Med. 363:2339-2350.
- Nolan CJ, Damm P, Prentki M. (2011). Type 2 diabetes across generations: from pathophysiology to prevention and management. Lancet. 378:169-181.
- Tahrani AA, Bailey CJ, Del prato S, Barnett AH. (2011). Management of type 2 diabetes: new and future developments in treatment. Lancet. 378:182-197.
- Kurotani K, Nanri A, Goto A, Mizoue T, Noda M, Kato M, et al. (2013). Vegetable and fruit intake and risk of type 2 diabetes: Japan Public Health Center-based Prospective Study.
- Anjana RM, Pradeepa R, Deepa M, Datta M, Sudha V, Unnikrishnan R, et al. (2011). Prevalence of diabetes and prediabetes (impaired fasting glucose and/or impaired glucose tolerance) in urban and rural India: Phase I results of the Indian Council of Medical Research–INdia DIABetes (ICMR–INDIAB) study. Diabetologia. 54:3022-3027.
- HU FB. (2011). Globalization of Diabetes: The role of diet, lifestyle, and genes. Diabetes Care., 34:1249-1257.
- Basu S, Stuckler D, Mckee M, Galea G. (2013). Nutritional determinants of worldwide diabetes: an econometric study of food markets and diabetes prevalence in 173 countries. Public Health Nutrition.16:179-186.
- IDF. (2013). IDF Diabetes Atlas. 11–17.
- Salas-Salvadó J, Martinez-González MÁ, Bulló M, Ros E. (2011). The role of diet in the prevention of type 2 diabetes. Nutri Metabol Cardio Dis. 21(2):B32-B48.
- Gajos G, Piłaciński S, Zozulińska-Ziółkiewicz D. (2013). Controversies in Diabetes in 2013 – a Brief Update. Adv Clin Exp Med. 22:777–784.
- Catalano PM. (2010). The impact of gestational diabetes and maternal obesity on the mother and her offspring. J Devpt Origins of Health Dis. 1:208–215.
- Petry CJ. (2010). Gestational diabetes: risk factors and recent advances in its genetics and treatment.
- Br J Nutr. 104(6):775-787.
- Forouhi NG, Wareham NJ. (2010). Epidemiology of diabetes. Medicine. 38:5.
- Kim SY, England L, Wilson HG, Bish C, Satten GA, Dietz P. (2010). Percentage of gestational diabetes mellitus attributable to overweight and obesity. J Public Health 100(6):1047–1052.
- UK D. (2013). What is diabetes? In: UK D. (ed.).
- Sabin MA. (2012). Type 2 Diabetes in Children. Diabetes Management: A journal for General Practitioners and Other Health Professionals. 38:24–26.
- Reinehr T. (2013). Type 2 diabetes mellitus in children and adolescents. World Journal Of Diabetes. 4:270-281.
- Roglic G, Unwin N. (2010). Mortality attributable to diabetes: Estimates for the year 2010. Diabetes Res Clin Practice. 87:15-19.
- Booth AO, Lowis C, Hunter SJ, Mckinley MC. (2008). Role of diet and physical activity in the self-management of type 2 diabetes: experiences and opinions of patients and health professionals. Proceedings of the Nutrition Society. 67:N.PAG.
- Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, Leccesi L, et al. (2012). Bariatric Surgery versus Conventional Medical Therapy for Type 2 Diabetes. England J Med. 366:1577-1585.
- Englyst HN, Hudson GJ. (2003). Carbohydrates in Human Nutrition and Dietetics. (eds.) Churchill Livingstone: Elsevier Science.
- Henry CJ, AhlstrὊm L. (2009). Nutrition in Food Science and Technology. (eds.) Sussex, Blackwell.
- Schwartz MW, Seeley RJ, Tscho¨p MH, Woods SC, Morton GJ, Myers MG, et al. (2013). Cooperation between brain and islet in glucose homeostasis and diabetes. Nature. 503:59-66.
- Hong H, J0 J, Sin SJ. (2013). Stable and flexible system for glucose homeostasis. Phy Rev. 88:032711.
- Menge BA, Grüber L, Jørgensen SM, Deacon CF, Schmidt WE, Veldhuis JD, et al. (2011). Loss of Inverse Relationship Between Pulsatile Insulin and Glucagon Secretion in Patients With Type 2 Diabetes. Diabetes. 60:2160-2168.
- Park JH, Bae JH, IM SS, Song DK. (2014). Green tea and type 2 diabetes. Integr Med Res. 3(1):4-10.
- Ferland-McCollough D, Ozanne SE, Siddle K, Willis AE, Bushell M. (2010). The involvement of microRNAS in Type 2 diabetes. Biochem Soc Trans. 38(6):1565–1570.
- Siddiqui S. (2013). Depression in type 2 diabetes mellitus – A review. Diabetes Metab Syndr. 8(1):62-65.
- Shaw JE, Sicree RA, Zimmet PZ. (2010). Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 87:4-14.
- Office B. (2013). Federal Government of Nigeria Budget.
- Kahn SE, Cooper ME, Del Prato S. (2011). Pathophysiology and treatment of type 2 diabetes: perspectives on the past, present, and future. The Lancet.
- Whiting DR, Guariguata L, Weil C, Shaw J. (2011). IDF Diabetes Atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Practice. 94:311-321.
- Brian G, Ramke J, Page A, Maher L, Szetu J, Qoqonokana MQ. (2011). The association of diabetes and BMI among Melanesian and Indian Fijis aged ≥ 40 years. British J Nutri. 105:1539–1545.
- Cheong KC, Yusoff AF, Ghazali SM, Lim KH, Selvarajah JH, Khor GL, et al. (2013). Optimal BMI cut-off values for predicting diabetes, hypertension and hypercholesterolaemia in a multi-ethnic population. Public Health Nutr. 16:453–459.
- Scheen AJ, Van gaal LF. (2014). Combating the dual burden: therapeutic targeting of common pathways in obesity and type 2 diabetes. Lancet Diabetes Endocrinol. 2(11):911-922.
- Donin AS, Nightingale CM, Owen CG, Rudnicka AR, Jebb SA, Ambrosini GL, et al. (2014). Dietary energy intake is associated with type 2 diabetes risk markers in children. Diabetes Care. 37(1):116-123.
- Esfahani A, Lam J, Kendall CWC. (2014). Acute effects of raisin consumption on glucose and insulin reponses in healthy individuals. J Nutr Sci. 3:00.
- Wing RR, Lang W, Wadden TA, Safford M, Knowler WC, Bertoni AG, et al. (2011). Benefits of Modest Weight Loss in Improving Cardiovascular Risk Factors in Overweight and Obese Individuals With Type 2 Diabetes. Diabetes Care. 34:1481-1486.
- Wasserman DH, Kang L, Ayala JE, Fueger PT, Lee-young RS. (2011). The physiological regulation of glucose flux into muscle in vivo. J Exp Biol. 214:254-262.
- Oliveira C, Simȯes M, Carvallo J, Ribeiro J. (2012). Combined exercise for people with type 2 diabetes mellitus: A systemic review. Diabetes Research and Clinical Practice. 98:187 - 198.
- Acheson KJ. (2010). Carbohydrate for weight and metabolic control: Where do we stand? Nutrition. 26:141-145.