Information Links
Related Conferences
Current Issue Volume 9, Issue 2 - 2025
A Study on Evaluating the Economical Burden of Skin Diseases: Fungal Infections and Scabies
Patel Keval Ashvinbhai*, Parera Sneh Sanjivkumar, Patel Dhruvi Ketan, Solanki Jaydeep Maheshbhai
Gujarat Technological University, India
*Corresponding author: Mr. Patel Keval Ashvinbhai, Gujarat Technological University, R.K Building, Railway Crossing Line, Station Road, Petlad, India, Phone: 9601773141, E-mail: [email protected]
Received Date: May 15, 2025
Published Date: July 07, 2025
Citation: Ashvinbhai PK, et al. (2025). A Study on Evaluating the Economical Burden of Skin Diseases: Fungal Infections and Scabies. Mathews J Dermatol. 9(2):30.
Copyrights: Ashvinbhai PK, et al. © (2025).
ABSTRACT
Background: Despite being highly prevalent, Fungal Infections and Scabies pose a significant economical burden. Evaluating this burden allows us to understand the average cost of treatment, potentially revealing expensive medications. This knowledge can guide the development of cost-effective alternatives, ultimately informing strategies and plans to prevent the spread of these common Infections.
Objectives:
- Investigate the financial burden of Fungal Infection and Scabies on patients.
- Determine the Prevalence of Fungal Infection and Scabies on patients.
- Determine the Prevalence of Fungal Infection and Scabies in a diverse patient population.
- Evaluate the burden of Fungal Infection and Scabies on patient’s productivity.
Method: After receiving approval from the ethics committee, a study was conducted to assess the economical burden of Fungal diseases and Scabies. The study involved observing patients visiting the dermatology department of Dr Sohana's Skin and Laser Clinic in Nadiad, India. Patients of all genders diagnosed with either Fungal Infection and Scabies were included in this concurrent observational study.
Result: A total of 257 patients were included in our study out of which 236 patients were of Fungal disease and 21 patients were of Scabies The economical burden study of both Fungal Infection and Scabies showed that overall study population was predominantly male which comprised of 53.38% for Fungal Infection and male which comprised of 57.14% for Scabies. Most of the patients were in age group of 18 to 35 which consist of about 39.40% for Fungal Infection and 57.14% for Scabies respectively. Tinea corporis (75.84%) was mostly found among Fungal Infection patients.
- (62.55%) AntiFungal agents were prescribed by Oral route as compared to Topical route (37.44%).
- (40.78%) Anti-Scabies agents were prescribed by Oral route as compared to Topical route (59.21%).
Conclusion: This observational study highlights the substantial burden of Fungal Infections and Scabies over six months at Dr. Sohana’s Skin and Laser Clinic. Fungal Infections (91.8%) predominantly affected rural males, with Tinea Corporis being most common. Itraconazole and Luliconazole were frequently prescribed, incurring ₹4,11,997 in costs. Scabies (8.2%) was more common in urban males, treated mainly with Permethrin and Ivermectin, costing ₹22,332. These findings underline the significant clinical and economic impact, along with notable demographic and treatment trends.
Keywords: Fungal Infection, Scabies, Pathophysiology and Treatment of Fungal Infection and Scabies, Economical Burden of Skin Diseases, Burden of Fungal Infection, Burden of Scabies.
INTRODUCTION
Economic Burden of Skin Diseases:
- Fungal infections and scabies impose significant economic burdens in India.
- These burdens include direct medical costs (treatment, diagnosis) and indirect costs (lost productivity, suffering) [1,2].
- Fungal infections like dermatophytosis require prolonged treatment, increasing expenses [3].
- Scabies, a contagious infestation, also leads to financial strain due to medication and consultations [1,2]
- Both conditions contribute to economic challenges for individuals and healthcare systems [3].
Skin Anatomy and Function:
- The skin, the body's largest organ, acts as a protective barrier and regulates temperature.
- It comprises three main layers: epidermis, dermis, and hypodermis.
- The epidermis, the outermost layer, provides protection and maintains hydration [4].
- The dermis, containing hair follicles and glands, supports the epidermis and enables sensation.
- The hypodermis, the deepest layer, insulates and stores energy.
- Skin colour and function vary due to factors such as age, race, and gender [4].
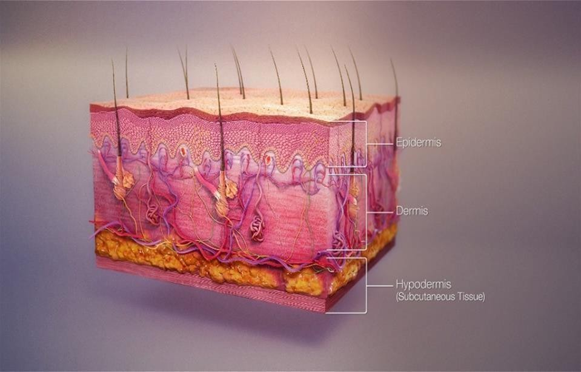
Figure 1. Layers of skin.
Fungal Infections
A fungal infection, or mycosis, is caused by fungi that can affect the skin, hair, nails, mucous membranes, and internal organs. While many fungi are harmless, some cause disease under certain conditions. Superficial fungal infections, impacting the skin, hair, and nails, are usually caused by dermatophytes or yeasts. Tinea, a common and contagious superficial infection, spreads through contact with infected people or contaminated surfaces. Despite the name "ringworm," tinea is caused by dermatophytes, not worms. Tinea and dermatophyte infections differ from other fungal infections like candidiasis. Some forms of tinea can be treated with over-the- counter creams and medications.
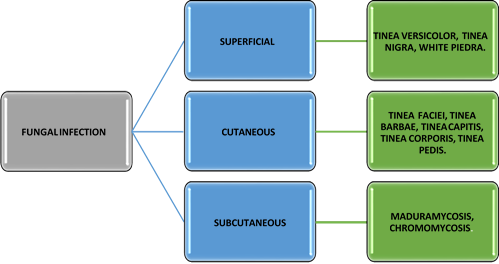
Figure 2. Classification of Fungal Infection.
TINEA CORPORIS (RINGWORM):
- Tinea corporis, or ringworm, is a fungal infection marked by a red, scaly circular rash with clear skin in the centre. In hairy areas like the scalp or beard, hair loss may occur.
- It is caused by dermatophytes, fungi that thrive in warm, humid environments and spread through direct contact with infected individuals, pets, or contaminated items like clothing and towels [5].
- Treatment typically begins with topical antifungal creams. For widespread or severe cases, oral antifungal medications may be prescribed. Creams usually clear the infection in about two weeks, with an additional week of use recommended to fully eliminate the fungus.
- Common topical treatments include clotrimazole, miconazole, and ketoconazole. Oral medications like griseofulvin and terbinafine are often prescribed for about a week [5].

Figure 3. Tinea Corporis.
TINEA CAPITIS (SCALP RINGWORM):
- Tinea capitis is a contagious fungal infection of the scalp caused by dermatophytes, mainly Trichophyton and Microsporum species.
- It presents with patchy hair loss, broken hairs, and dark "black dots." Other symptoms include inflammation, itching, swelling, pustules, scaling, flaking, redness, and ring-shaped patches—sometimes resembling seborrheic dermatitis.
- Treatment involves oral antifungal medications like griseofulvin or terbinafine (Lamisil). Blood and hair cultures may be used to monitor treatment success and confirm the fungus is fully eradicated [6].

Figure 4. Tinea Capitis.
TINEA CRURIS (JOCK ITCH, GROIN RINGWORM):
- Tinea cruris is a fungal infection of the groin, more common in men due to the warm, moist environment but can affect both sexes.
- It is caused by fungi such as Trichophyton rubrum, Candida albicans, Trichophyton mentagrophytes, and Epidermophyton floccosum. The infection can also spread from other areas like athlete’s foot (tinea pedis) or fungal nail infections (tinea unguium).
- Treatment primarily involves topical antifungal medications like azoles and allylamines, which disrupt ergosterol production in the fungal cell wall, leading to fungal death [7].

Figure 5. Tinea Cruris.
TINEA VERSICOLOR:
- Tinea versicolor is a common fungal skin infection caused by an overgrowth of Malassezia yeast (formerly Pityrosporum ovale), normally present on the skin. It disrupts melanin production, causing patchy discoloration—either lighter (hypopigmentation) or darker (hyperpigmentation) than the surrounding skin. Patches may be scaly, itchy, and slightly raised, commonly appearing on the chest, back, shoulders, and upper arms.
- Treatment involves topical antifungal medications in forms like creams, lotions, or shampoos, with active ingredients such as selenium sulphide, clotrimazole, miconazole, and terbinafine [8].

Figure 6. Tinea Versicolor.
TINEA PEDIS:
- Athlete's foot is the most common fungal infection of the feet, caused by dermatophyte fungi. It is rare in children and more likely with age. Risk factors include tight, non-breathable shoes, sweaty feet, and use of shared spaces like locker rooms.
- The most common form affects the spaces between the toes, making them soft, wrinkled, or scaly. Chronic hyperkeratotic (moccasin-type) tinea pedis presents with persistent redness and scaling on the soles and sides of the feet, sparing the top. A less common type causes blisters or inflammation, sometimes mistaken for pompholyx eczema. Recurrence may be linked to untreated fungal nail infections [9].

Figure 7. Tinea Pedis.
TINEA UNGUIUM:
- Tinea unguium, or onychomycosis, is a common nail infection caused by dermatophyte fungi, especially in older adults—affecting up to 50% of those over 70. It often coexists with fungal skin infections like athlete’s foot (tinea pedis). The most common form begins at the nail's edge and underside, causing yellow-brown discoloration, onycholysis (nail separation), and subungual hyperkeratosis (thickening under the nail).
- Another type presents as white spots on the nail plate (white superficial onychomycosis), which can spread if untreated. Accurate fungal diagnosis is essential, as other nail conditions may mimic it. Those with existing nail disorders, weakened immune systems, or diabetes are more susceptible and face higher risks of complications like cellulitis [10].
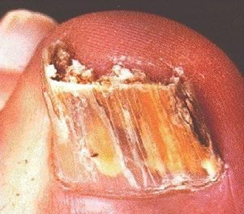
Figure 8. Tinea Unguium.
OTHER FORMS OF TINEA:
- There are other forms of tinea that can occur. Modern dermatology treatments such as medications and topical treatments can be used to treat these forms of tinea effectively.
- Tinea Faciei – This is a tinea Fungal Infection that affects the face.
- Tinea Barbae – This type of tinea is classified as a Fungal Infection of the hair follicles and often can occur in and around men’s beards.
- Tinea Manuum – This is a tinea Infection that is constrained to the hands and fingers [11].
PATHOPHYSIOLOGY OF FUNGAL INFECTION:
- Fungi from the Ascomycota and Basidiomycota groups are major causes of human fungal infections. Ascomycota can infect the mouth, throat (oropharyngeal), ears, sinuses (oto-laryngeal), skin, eyes, nervous system, urinary tract, heart, lungs, and cause systemic infections. Basidiomycota, like Cryptococcus, can lead to meningitis, while Malassezia causes skin infections.
- Fungal infections spread mainly through contact with infected individuals or inhalation of spores. Dermatophytes such as Microsporum, Epidermophyton, Trichophyton, Sporothrix, and Malassezia infect damaged skin via direct contact. These fungi secrete keratin-degrading enzymes, causing superficial infections in hair, nails, and skin. Inhaled spores or conidia can reach the lungs and trigger pulmonary infections [12].
- The immune system uses Pattern Recognition Receptors (PRRs), like dectin and toll- like receptors (TLRs), to detect fungal cell wall components (PAMPs), such as chitin and beta-glucans. This recognition activates innate immune responses: phagocytes (e.g., monocytes, macrophages, neutrophils, dendritic cells) engulf fungi, release reactive oxygen/nitrogen species, and secrete cytokines and chemokines to induce inflammation. Phagocytes may kill fungi in phagolysosomes or contain them in granulomas.
- Monocytes also act as antigen-presenting cells (APCs), activating T lymphocytes for adaptive immunity. However, fungi can evade immunity by altering surface PAMPs, forming immune-resistant structures (e.g., asteroid bodies in S. schenckii), or switching forms like Candida (yeast to hyphae), enabling tissue invasion, phagocyte resistance, and membrane rupture. Some fungi survive within macrophages. Blastomyces species produce BAD1 protein, disrupting the complement system and aiding systemic spread. These evasion strategies help fungi resist phagocytosis, suppress T cell activity, reduce inflammation, and tolerate oxidative/nitrosative stress [12].
TREATMENT OF FUNGAL INFECTION:
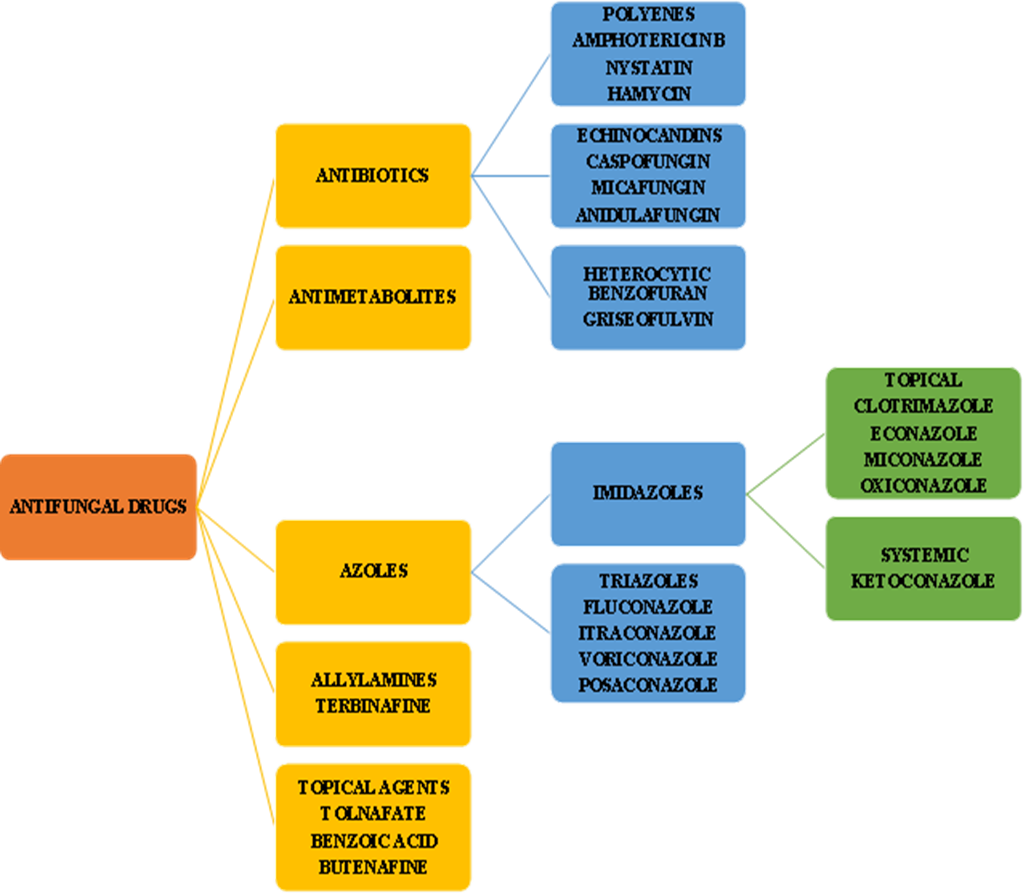
Figure 9. Treatment of Fungal Infection [13].
Scabies:
- Scabies is a highly contagious skin condition affecting millions worldwide, especially young children, older adults, the immunocompromised, and those with developmental delays. It spreads easily in crowded settings like daycare centers, nursing homes, and prisons.
- It is more common in communities facing poverty, overcrowding, malnutrition, and poor healthcare access, particularly in Indigenous and resource-poor areas. Healthcare professionals note the often-overlooked burden of Scabies in these populations.
- In some Indigenous communities, factors like poverty, overcrowding, bed-sharing among children, and lack of healthcare expertise contribute to its spread. Misdiagnosis delayed or inadequate treatment, and limited access to clean water worsen the problem, leading to secondary infections.
- Improving living conditions and access to trained healthcare providers is vital to reducing Scabies in these communities [14].
PATHOPHYSIOLOGY OF SCABIES:
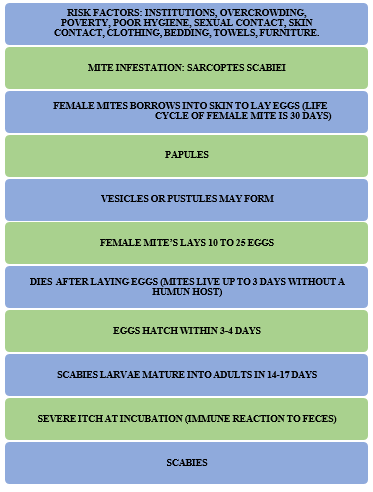
Figure 10. Pathophysiology of Scabies [15].
TREATMENT OF SCABIES:

Figure 11. Treatment of Scabies [16].
ECONOMICAL BURDEN:
- The economic burden of skin diseases involves both direct and indirect costs. Direct costs include medical consultations, medications, and treatments, varying with severity and chronicity. Indirect costs encompass lost productivity due to absenteeism and reduced work efficiency. Skin conditions can also significantly impact quality of life, leading to psychological distress, social withdrawal, and decreased self-esteem. Additional indirect costs arise from over-the-counter remedies, specialized skincare, and caregiving expenses. These combined factors place a substantial financial strain on individuals, families, healthcare systems, and society as a whole [17].
NEED OF THE STUDY
Fungal Infections and Scabies are common skin conditions, but their true economical impact remains unclear. This study is needed to address this gap in knowledge for several reasons:
- Economical Burden: By investigating the financial burden on patients, the study can identify areas where healthcare costs can be optimized. This includes costs associated with medications, consultations and financial lost due to missed work.
- Prevalence: Understanding the prevalence of these conditions in the study population can inform public health resource allocation and prioritize interventions.
- Diversity: Including a diverse patient population ensures the findings are generalizable and can be applied to broader populations. This is crucial as prevalence and economical burden may vary across demographics.
- Productivity: Assessing the impact on patient productivity allows us to understand the broader economic impact beyond healthcare costs. Reduced productivity due to missed work or discomfort can have significant consequences.
AIMS AND OBJECTIVES
AIM: a study on evaluating the economical burden of skin diseases: fungal infections and scabies.
OBJECTIVES:
- Investigate the financial burden of Fungal Infection and Scabies on patients.
- Determine the prevalence of Fungal Infection and Scabies on patients.
- Determine the Prevalence of Fungal Infection and Scabies in a diverse patient population.
- Evaluate the burden of Fungal Infection and Scabies on patient’s productivity.
MATERIALS AND METHODOLOGY
STUDY DESIGN: Concurrent observational study.
STUDY SITE: This study was conducted at Dr Sohana’s Skin and Laser Clinic, Nadiad, Gujarat.
STUDY DURATION: This study was conducted over 6 months from 2nd September 2023 to 2nd March 2024.
STUDY POPULATION: 257 patients were enrolled in this study.
ELIGIBILITY CRITERIA:
INCLUSION CRITERIA
- Patients diagnosed with a specific skin disease (i.e. Fungal Infection such as Tinea Corporis, Candidiasis, Tinea Versicolor, Tinea Pediculosis, Tinea Barbae, Tinea Capitis, Tinea Cruris, Tinea Manuum. Tinea unguium) and Scabies.
- All patients above 18 years of age & genders.
- Patients who are willing to participate in the study and provide informed consent.
EXCLUSION CRITERIA
- Patients with comorbid conditions that may significantly impact the economical burden assessment.
- Patients who are unable or unwilling to provide informed consent.
- Patients who have incomplete medical records or missing data for economical evaluation.
- Special populations such as pregnancy, diabetes and pediatric patients.
STUDY MATERIAL:
- ICF (Informed Consent Form) Annexure-4.4
- PIS (Patient Information Sheet) Annexure-4.2
- CRF (Case Report Form).
Requirement of any investigations or interventions to be conducted on participants There is no requirement of any investigations or interventions to be conducted on participants. Plan of statistical analysis [Details of tables, tests and other statistical analysis] Use statistical analysis software (word or excel and etc) for data analysis. Calculate prevalence rates, means, and standard deviations for descriptive statistics. Perform regression analyses to explore relationships between variables, such as treatment outcomes. To assess the burden of skin diseases, we can employ various measures. One common approach is to evaluate the impact on productivity, such as days missed from work or school, reduced quality of life, and healthcare costs associated with treatment. CRF is also be used to gather information directly from affected individuals, helping to understand the physical and financial toll these conditions may have. By combining these methods, we can gain a comprehensive understanding of the burden of skin diseases.
Burden is evaluated by using formula;
BURDEN= DIRECT MEDICAL COST + INDIRECT COST.
Impact means financial and social loss of patient due to disease condition. Prevalence means population of interest out of total population.
ETHICAL ISSUES:
Informed consent process [justify, if asked for waiver] In this study, the data will be collected from patients and direct involvement of patient/ subject and therefore need of informed consent process. Steps proposed for protection of participants from unanticipated harm arising out of the study [Including privacy and confidentiality] Identity of patient’s data will not be disclosed. Confidentiality will be maintained at all levels of the study. Plan of publication at the end of study We are planning to publish research paper of this study after completion of the work. Declaration about amount of funds required and its source External funds are not required for this study.
CONTRIBUTION OF THE RESEARCH PROJECT
[How the research will benefit the community at large; measures to be undertaken to address the identified problem]
The research on evaluating the economical burden of Fungal Infections and Scabies will benefit the community at large in several ways. Firstly, it will provide valuable insights into the prevalence of these skin diseases, helping healthcare providers and policymakers understand the scope of the problem. This knowledge can guide the allocation of resources and the development of preventive measures. To address the identified problem, measures can be undertaken such as raising awareness about proper hygiene practices, promoting early detection and treatment, and implementing cost effective interventions. Additionally, investing in healthcare infrastructure and improving access to affordable treatments can help alleviate the burden on patients and the economy. By taking these measures, we can work towards minimizing the impact of Fungal Infections and Scabies on the community's well- being.
RESULT
RESULT FOR FUNGAL INFECTION
A Concurrent Observational study was conducted at Dr. Sohana’s Skin and Laser Clinic, Nadiad over a period of 6 months from 2nd October 2023 to 2nd March 2024. Based on eligibility criteria, subjects were recruited in the study. In this study a total of 257 cases were collected out of which 236 subjects were presented with Fungal Infections.
ECONOMICALBURDEN OF FUNGAL INFECTION
The economical burden of a disease refers to the total cost of disease, this includes both direct medical costs and indirect costs.
The burden is calculated by using formula BURDEN= Direct medical cost + Indirect cost
₹366687 is a total direct medical cost of 236 Patients of Fungal Infection.
₹45310 is a total Indirect cost of 236 Patients of Fungal Infection.
Burden = Direct cost + Indirect cost
= 366687 + 45310
= ₹4,11,997 (Total Economical burden of Fungal Infection)
Fungal Infections:
- The study found a total economic burden of ₹4,11,997 for fungal infections, with direct medical costs contributing ₹366,687 and indirect costs ₹45,310. Males experienced a slightly higher economic burden (₹214,628) than females (₹197,369). Rural patients also showed a higher economic burden (₹227,896) compared to urban patients (₹184,101).
- The study population consisted of 236 patients, with a mean age of 33.75 years. The most affected age group was 18-35 years, with a higher prevalence in males. Tinea corporis was the most common fungal infection (75.84%), followed by tinea cruris (15.25%).
- Oral antifungal medications were more frequently prescribed (62.55%) than topical agents (37.44%). Luliconazole and itraconazole were the most commonly prescribed antifungal drugs, while levocetirizine was the most common supportive medication.
RESULT FOR SCABIES
- A concurrent observational study was conducted at Dr. Sohana’s Skin and Laser Clinic, Nadiad over a period of 6 months from 2nd September 2023 to 2nd March 2024. Based on eligibility criteria, subjects were recruited in the study. In this study total 257 cases were collected out of which 21 subjects were presented with Scabies.
ECONOMICAL BURDEN OF SCABIES
The economical burden of a disease refers to the total cost of disease, this includes both direct medical costs and indirect costs.
The burden is calculated by using formula BURDEN= Direct medical cost + Indirect cost.
₹19092 is a total direct medical cost of 21 Patients of Scabies.
₹3240 is a total Indirect cost of 21 Patients of Scabies.
Burden = Direct cost + Indirect cost
= 19092 + 3240
=₹22332 (Total Economical burden of Scabies)
Scabies:
- The total economic burden of scabies was ₹22,332, with direct medical costs of ₹19,092 and indirect costs of ₹3,240. Males had a higher economic burden (₹13,098) than females (₹9,234), and urban patients had a higher burden (₹13,868) than rural patients (₹8,464).
- The study included 21 scabies patients, with a mean age of 30.71 years. The 18-35 age group was most affected, with a higher prevalence in males.
- Topical agents were more commonly prescribed (59.21%) than oral agents (40.78%). Permethrin lotion and levocetirizine were the most frequently prescribed medications.
Overall Burden:
The combined economic burden of fungal infections and scabies was ₹434,329. Fungal infections accounted for 94.85% of the total burden, while scabies accounted for 5.14%.
Key Findings and Implications:
- Fungal infections represent a significantly larger economic burden than scabies in the studied population.
- Rural populations and males tend to experience a greater economic impact from fungal infections.
- Urban populations and males tend to experience a greater economic impact from Scabies.
- Tinea corporis is the predominant fungal infection, highlighting the need for targeted prevention and treatment strategies.
- The high prevalence of fungal infections in the 18-35 age group underscores the importance of public health initiatives aimed at this demographic.
- The high utilization of Azole drugs in fungal infections, and Permethrin lotion in scabies show the current treatment trends.
- The study highlights the need for further research to explore the underlying factors contributing to the observed demographic and economic disparities.
DISCUSSION
- The study on economical burden of Fungal Infection in the diverse population revealed that the higher economical burden may found in male patient are ₹214628 (52%) and in female the economical burden of Fungal Infection is ₹197369 (48%) and the total burden on both male as well as female are ₹411997.
- The most economical burden of Fungal Infection was found in rural area are ₹227896 (55%) and in urban area the economical burden of Fungal Infection was found to be 184101(45%) and total burden in both area Urban as well as in Rural was found to be ₹411997.
- The age wise distribution was analysed, and it was found as mean cost for the treatment of Fungal Infection are higher in female and the age group of the female are 36-52 (₹1948.26) and 53-70 (₹1769.38) and in male age group, the mean cost is higher in age 36-52(₹2095.40) and 53-70 (₹1750.5).
- Age wise distribution was analysed, and it was found that most of male patient having the Fungal Infection and in which most of the age group of 18-35 (39.40%), 36-52 (11.44%) and in female age group most of the age group are 18-35(25.84%) and 36- 52(14.40%).
- The study on eonomical burden of Fungal Infection in diverse population revealed that the higher chances of Fungal Infection in male (53.38%) and the mean cost are ₹1703.4, and in female (46.61%) and the mean cost are ₹1794.26.
- The most of the Fungal Infection patients were found in Rural area 52.54% (n=124) compared with the Urban area are 47.45% (n=112). The mean cost is higher in rural area (₹1837.87) and in Urban area (₹163.75) and the mean cost of both area Urban as well as Rural found to be ₹3481.62.
- Most common Fungal Infection in study population was Tinea Corporis accounting 75.84%. In a similar study conducted by Naaz R, et al. [18] revealed that Tinea Corporis was most found Fungal Infection estimating 33% followed by Tinea Cruris estimating 25.8%. In a contradictory study carried out by Bansal P, et al. (2021) [19] reported that most common Fungal Infection was found Tinea Cruris estimating 41.5% followed by 38% of Tinea Corporis.
- The mean cost of Tinea Corporis (₹1757.83), Tinea Cruris (₹1715.61), Tinea Capitis (₹1649.8), Tinea Faciei (₹1501.83), Tinea Pedis (₹2096), Candidiasis (₹1066), Tinea Versicolor (₹1462), Tinea Incognito (₹2082.66) and Tinea Unguium (₹1248).
- This study manifested that mostly drug was prescribed by per oral route accounting 62.55 % followed by Topical route accounting 37.44 %. In a similar study conducted by Deb P, et al. [16] concluded that most common route of administration was oral accounting 64.8% followed by topical route 58.4%. In a contradictory study conducted by Reza A, et al. [20] concluded that topical route was most prescribed route with 69% followed by oral route with 30.3%. In a contrast study conducted by Naaz R, et al. [18] concluded that 64% drugs prescribed topically, and 36% drugs were prescribed orally and the mean cost of per oral drug are ₹195.43 and topical are ₹281.35.
- From the analysis of 236 prescriptions of Fungal diseases it was found that the most prescribed topical antifungal agent was Luliconazole estimating 31.52 % and ketoconazole estimating 0.33 % followed by oral antifungal agent such as Itraconazole estimating 29.99 %. In a contrast study conducted by Amiri Reza et al. (2022) [20] concluded that Ketoconazole soap was most prescribed antifungal drug. In a contradictory study conducted by Naaz R, et al. [18] revealed that ketoconazole was most prescribed followed by Itraconazole and supportive treatment include anti-histaminic medicines such as levocetirizine estimating 32.06% and desloratadine estimating 0.33 %. The mean cost of luliconazole is ₹296.04, Itraconazole ₹235.73, Levocetirizine ₹51.37, and Ketoconazole ₹759 [21-54].
DISCUSSION OF SCABIES
- The study on Economical burden of Scabies in the diverse population revealed that the higher Economical burden may found in male patient are ₹13098 (59%) and in female the Economical burden of Scabies is ₹9234 (41%) and the total burden on both male as well as female are ₹22332.
- The most Economical burden of Scabies was found in Urban area are ₹13868 (62%) and in Rural area the Economical burden of Scabies was found to be ₹8464 (38%) and Total burden in both area Urban as well as in Rural was found to be ₹22332.
- Age wise distribution was analysed and it was found that most of male patient having the Scabies and in which most of the age group are 18-35 (57.14%) and in female age group the most of the age group are 18-35(19.04%) and 36-52(19.04%) and 53-70 (4.76). and the mean cost found to be ₹1022.5 in female and ₹1091.5 in male age group of 18-35 and total mean cost are ₹4052.5.
- The study on economical burden of Scabies in population revealed that the higher chances of Scabies in male patients are 57.14% and in female 42.85 %. The mean cost higher in male (₹1091.5) and in female patients (₹1026). Total mean cost was found to be ₹2117.5.
- The most of the Scabies patients was found in Urban area was 61.90 % (n=13) compared with Rural area was 38.09% (n=8). The mean cost found in Urban area was ₹1066.76 and in Rural area ₹1058 , total mean cost was ₹2124.76.
- This study manifested that mostly drugs was prescribed by topical route accounting 59.21% followed by per oral route accounting 14.78% and the mean cost of topical drug was found to be ₹323.90 and per oral was ₹171.38.
- From the analysis of 21 prescription of Scabies it was found that most prescribed anti-Scabies agent was permethrim lotion estimating 23.81% and ivermectin lotion estimating 11.11% and secalia lotion estimating 9.52 % and supportive treatment include anti-histaminic medicines such as levocetirizine estimating 33.33% and Vizigly soap estimating 14.29% and desloratadine estimating 3.17%. and the mean cost of permethrin lotion was ₹109, Vizigly soap ₹279, Ivermectin ₹123, Levocetirizine ₹64, Secalia lotion ₹217 and Desloratadine ₹75.
LIMITATIONS
Difficulty in accurately estimating indirect costs such as productivity loss and reduced quality of life, which may vary based on individual circumstances and cultural factors.
Limited availability of data on certain aspects of skin disease burden, particularly in low- resource settings or marginalized populations.
Challenges in accounting for comorbidities and other confounding factors that may influence economical burden assessment.
Potential biases in self-reported data, leading to inaccuracies in cost estimations.
CONCLUSION
The concurrent observational study conducted at Dr. Sohana’s Skin and Laser Clinic from 2nd September 2023 to 2nd March 2024 revealed significant findings regarding Fungal Infections and Scabies. Out of 257 cases, 236 patients were diagnosed with Fungal Infections, with a total economical burden of ₹4,11,997, predominantly affecting males and rural areas. Tinea Corporis was the most common Fungal Infection, with oral drugs being the primary treatment. Luliconazole cream and Itraconazole were most commonly prescribed antiFungal agents. Scabies affected 21 out of 257 cases, with an economical burden of ₹22,332, more prevalent in urban areas. Male patients showed a higher incidence of Scabies. Topical agents were the most prescribed treatment for Scabies. Permethrin lotion and Ivermectin were the most commonly prescribed anti-Scabies agents. Overall, these findings underscore the considerable economical and healthcare impact of these dermatological conditions, with variations observed across demographics and treatment modalities.
TABLES AND GRAPHS
A. GENDER WISE ECONOMICAL BURDEN OF FUNGAL INFECTION:
|
GENDER |
ECONOMICAL BURDEN |
|
MALE |
214628 |
|
FEMALE |
197369 |
|
TOTAL |
411997 |
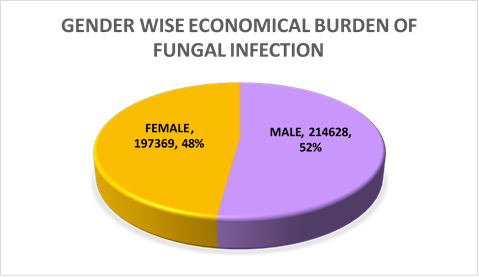
Graph 6.1.1 A: Gender wise economical burden of fungal infection.
B. AREA WISE ECONOMICAL BURDEN OF FUNGAL INFECTION:
|
AREA |
ECONOMICAL BURDEN |
|
RURAL |
227896 |
|
URBAN |
184101 |
|
TOTAL |
411997 |
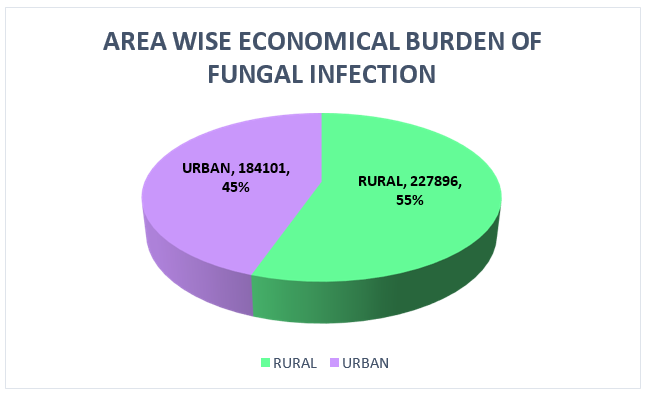
Graph 6.1.1 B: Area wise economical burden of fungal infection.
A. Demographic data according to age:
|
Age group (Years) |
GENDER |
Total number of patients(n) |
Percentage |
Mean cost |
|
18-35 |
FEMALE |
61 |
25.84% |
1728.06 |
|
MALE |
93 |
39.40% |
1586.54 |
|
|
36-52 |
FEMALE |
34 |
14.40% |
1948.26 |
|
MALE |
27 |
11.44% |
2095.4 |
|
|
53-70 |
FEMALE |
13 |
5.50% |
1769.38 |
|
MALE |
6 |
2.54% |
1750.5 |
|
|
70 UP |
FEMALE |
2 |
0.84% |
1357 |
|
MALE |
0 |
0 |
0 |
|
|
Total(N) |
236 |
100% |
12235.2 |
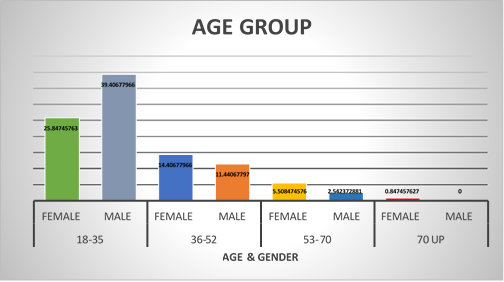
Graph 6.1.2 A: Age and Gender wise distribution of fungal disease.
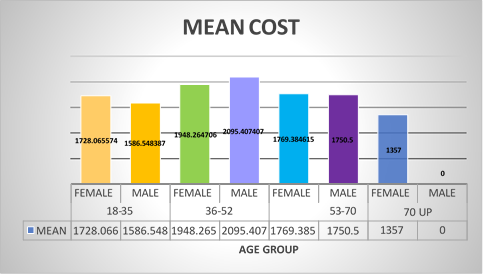
Graph 6.1.2.A: Age and Gender wise mean cost.
B. Demographic data according to Gender:
|
Gender |
Total number of patients(n) |
Percentage |
Mean cost |
P value |
|
Male |
126 |
53.38% |
1703.4 |
0.29 |
|
Female |
110 |
46.61% |
1794.26 |
|
|
TOTAL |
236 |
100% |
3497.66 |
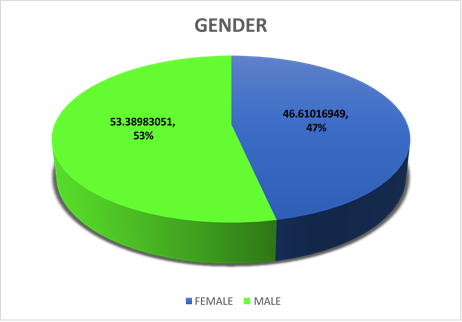
Graph 6.1.2.B: Gender wise categorization of fungal disease.
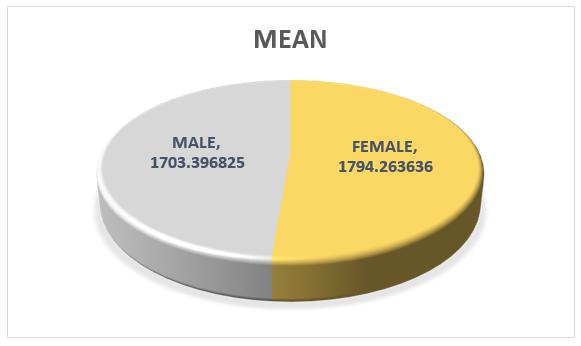
Graph 6.1.2.B: Gender wise categorization of mean cost.
6.13 AREA WISE DETAIL OF STUDY POPULATION:
|
Area |
Total Number of Patients (N) |
Percentage |
Mean Cost |
|
Rural |
124 |
52.54% |
1837.87 |
|
Urban |
112 |
47.45% |
1643.75 |
|
Total |
236 |
100% |
3481.62 |
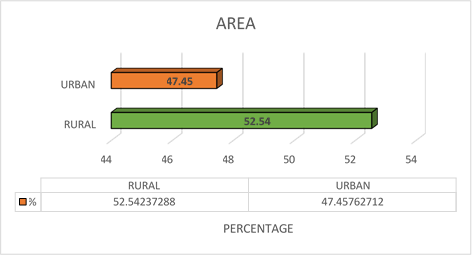
Graph 6.1.3: Area wise detail of study population.
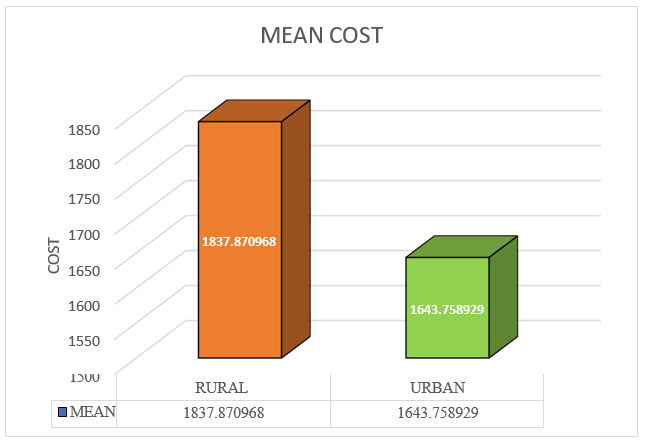
Graph 6.1.3: Area wise mean cost.
6.1.4 FUNGAL INFECTION CATEGORIZATION:
|
Fungal Infection |
Total number of patients(n) |
Percentage |
Mean cost |
|
T. CORPORIS |
179 |
75.84 |
1757.83 |
|
T. CRURIS |
36 |
15.25 |
1715.61 |
|
T. FACIEI |
6 |
2.54 |
1501.83 |
|
T. CAPITIS |
5 |
2.11 |
1649.8 |
|
T. VERSICOLOR |
4 |
1.69 |
1462 |
|
T. INCOGNITO |
3 |
1.27 |
2082.66 |
|
CANDIDIASIS |
1 |
0.42 |
1066 |
|
T. PEDIS |
1 |
0.42 |
2096 |
|
T. UNGUIUM |
1 |
0.42 |
1248 |
|
Total(N) |
236 |
100% |
14579.73 |
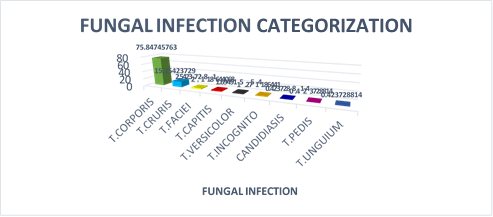
Graph 6.1.4: Fungal infection categorization.
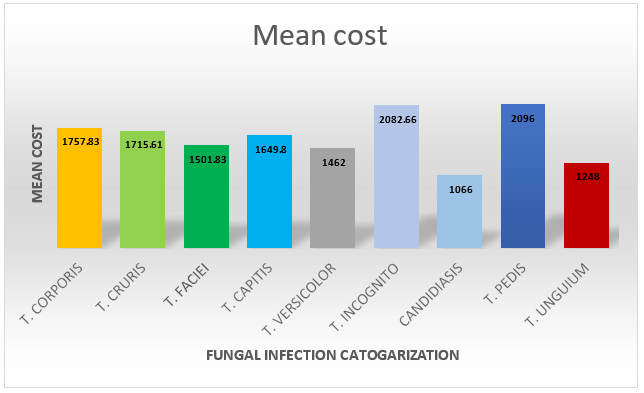
Graph 6.1.4: Mean cost of fungal infection categorization.
ROUTE OF ADMINISTRATION OF ANTI-FUNGAL AGENTS:
|
ROA |
Number of Prescription |
Percentage |
Mean cost |
|
PO |
675 |
62.55 |
195.43 |
|
Topical |
404 |
37.44 |
281.35 |
|
Total |
1079 |
100% |
476.78 |
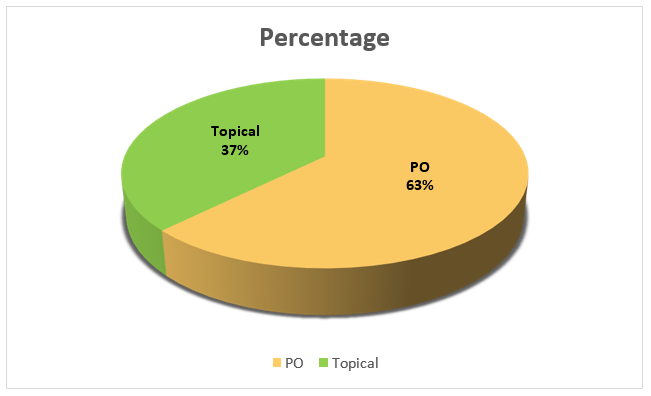
Graph 6.1.5: Route of administration of antifungal agents.
.png)
Graph 6.1.5: Mean cost of route of administration of antifungal agents.
EXTENT OF ANTIFUNGAL AGENTS PRESCRIBED:
|
Drugs |
Total Number of Drugs |
Percentage |
Mean cost |
|
Luliconazole |
289 |
31.52% |
296.04 |
|
Itraconazole |
275 |
29.99% |
235.73 |
|
Levocetirizine |
294 |
32.06% |
51.37 |
|
Supportive treatment |
51 |
5.56% |
4608.94 |
|
Desloratadine |
2 |
0.33% |
225 |
|
Griseofulvin |
3 |
0.33% |
482 |
|
Ketoconazole |
3 |
0.33% |
759 |
|
Total |
917 |
100% |
6658.08 |
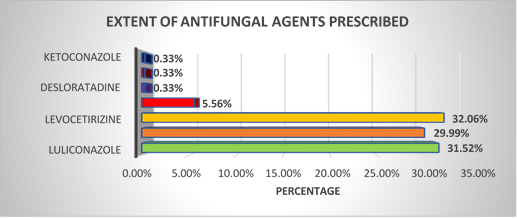
Graph 6.1.6: Antifungal agents.
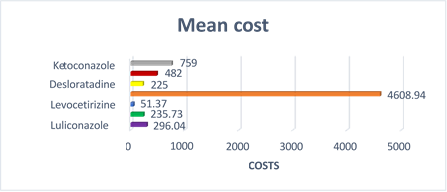
Graph 6.1.6: Mean cost of antifungal agents.
A. GENDER WISE ECONOMICAL BURDEN OF SCABIES:
|
GENDER |
ECONOMICAL BURDEN |
|
MALE |
13098 |
|
FEMALE |
9234 |
|
TOTAL |
22332 |
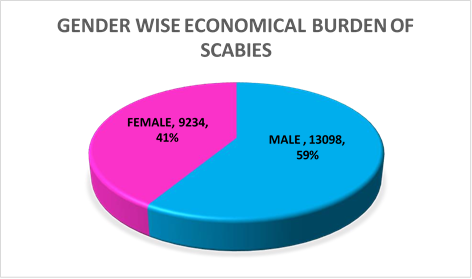
Table 6.2.1 A: Gender wise economical burden of scabies.
A. AREA WISE ECONOMICAL BURDEN OF SCABIES:
|
GENDER |
ECONOMICAL BURDEN |
|
RURAL |
8464 |
|
URBAN |
13868 |
|
TOTAL |
22332 |
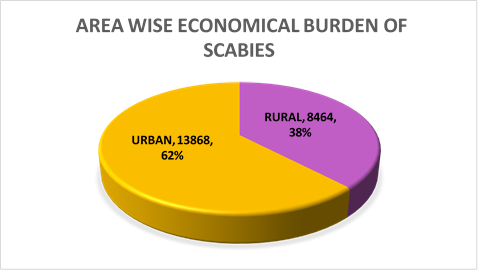
Table 6.2.1 B: Area wise economical burden of scabies.
6.2.2 DEMOGRAPHIC DETAILS OF STUDY POPULATION:
A. DEMOGRAPHIC DATA ACCORDING TO AGE:
|
Age group (Years) |
GENDER |
Total number of patients(n) |
Percentage |
Mean cost |
|
18-35 |
FEMALE |
4 |
19.04% |
1022.5 |
|
MALE |
12 |
57.14% |
1091.5 |
|
|
36-52 |
FEMALE |
4 |
19.04% |
1068.5 |
|
MALE |
0 |
0% |
0 |
|
|
53-70 |
FEMALE |
1 |
4.76% |
870 |
|
MALE |
0 |
0% |
0 |
|
|
70 UP |
FEMALE |
0 |
0% |
0 |
|
MALE |
0 |
0% |
0 |
|
|
TOTAL (n) |
21 |
100% |
4052.5 |
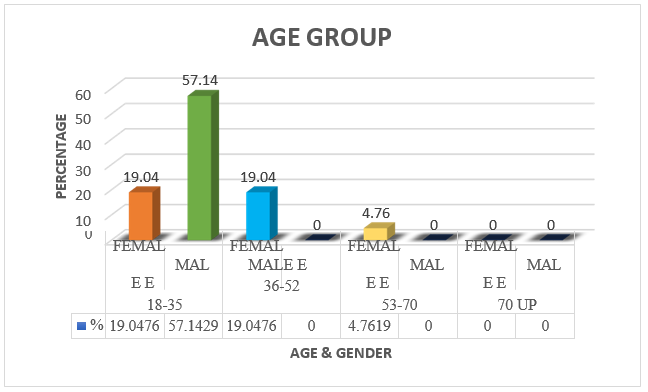
Graph 6.2.2 A: Age wise distribution of scabies.
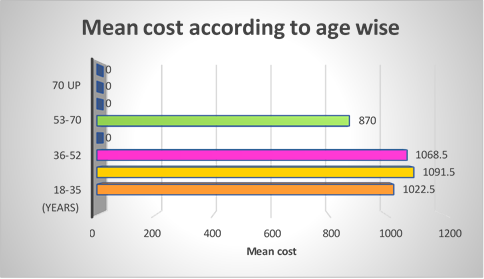
Graph 6.2.2 A: Age wise mean cost of scabies.
Demographic data according to Gender:
|
Gender |
Number of patients (n) |
Percentage |
Mean cost |
P value |
|
Male |
12 |
57.14% |
1091.5 |
0.5126 |
|
Female |
9 |
42.85% |
1026 |
|
|
Total (N) |
21 |
100% |
2117.5 |
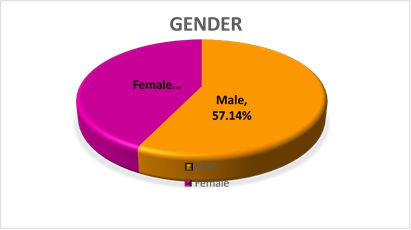
Graph 6.2.2.B: Gender wise categorization of scabies.
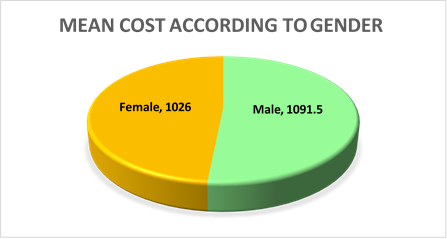
Graph 6.2.2.B: Gender wise mean cost for scabies.
6.2.3 AREA WISE DETAIL OF STUDY POPULATION:
|
Area |
Total Number of Patients (N) |
Percentage |
Mean cost |
|
Rural |
8 |
38.09% |
1058 |
|
Urban |
13 |
61.90% |
1066.76 |
|
TOTAL |
21 |
100% |
2124.76 |
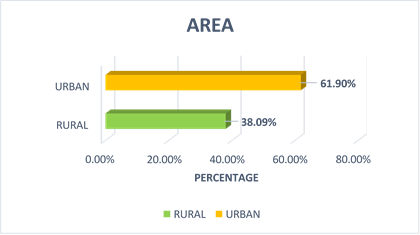
Graph 6.2.3: Area wise detail study of scabies in study population.
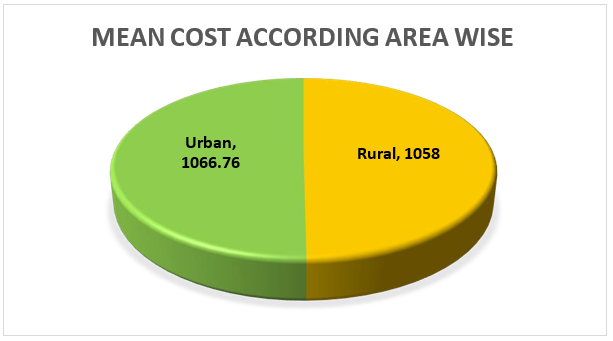
Graph 6.2.3: Area wise mean cost of scabies in study population.
6.2.4 ROUTE OF ADMINISTRATION OF ANTI-SCABIES AGENTS:
|
ROA |
Number of Prescription |
Percentage |
Mean cost |
|
PO |
31 |
40.78% |
171.38 |
|
Topical |
45 |
59.21% |
323.9 |
|
Total |
76 |
100% |
495.28 |
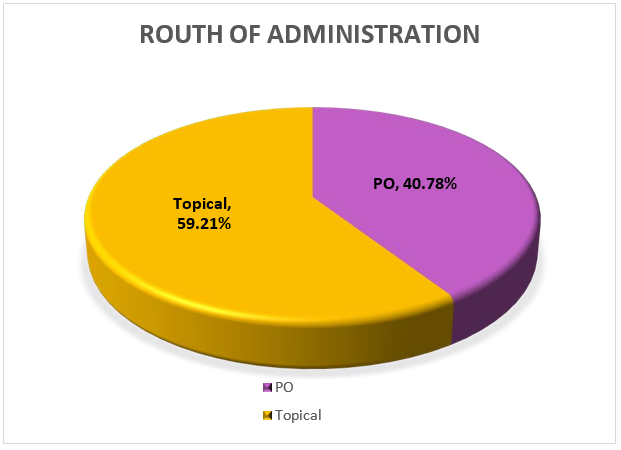
Graph 6.2.4: Route of administration of anti-scabies agents.
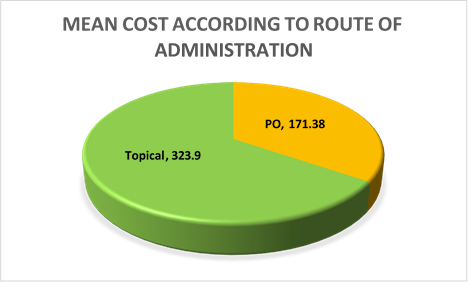
Graph 6.2.4: Mean cost according to route of administration.
6.2.5 EXTENT OF ANTISCABIES AGENTS PRESCRIBED:
|
Drugs |
Total Number of Drugs |
Percentage |
Mean cost |
|
Permethrin lotion |
15 |
23.81% |
109 |
|
Vizigly soap |
9 |
14.29% |
279 |
|
Levocetirizine |
21 |
33.33% |
64 |
|
Ivermectin |
7 |
11.11% |
123 |
|
Secalia lotion |
6 |
9.52% |
217 |
|
Supportive treatment |
3 |
4.76% |
186 |
|
Desloratadine |
2 |
3.17% |
75 |
|
Total |
63 |
100% |
1053 |
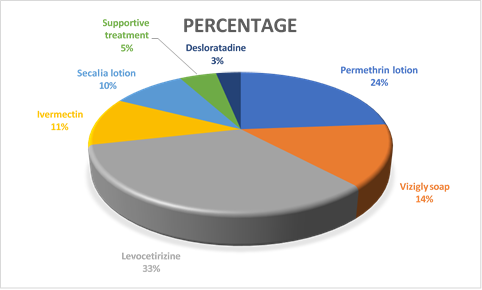
Graph 6.2.5: Extent of anti-scabies agents prescribed.
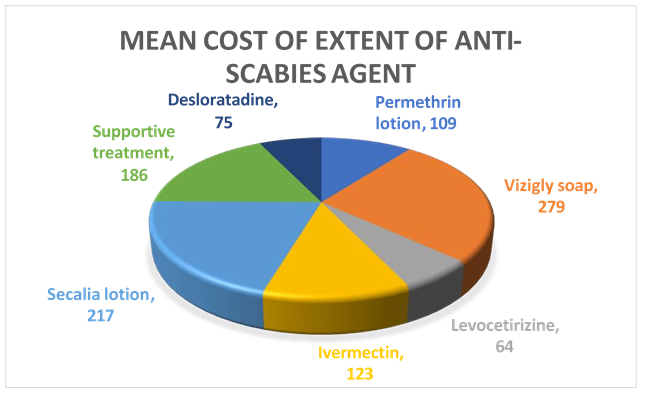
Graph 6.2.5: Mean cost of Extent of anti-scabies agents prescribed.
6.3 ASSESSMENT OF TOTAL BURDEN OF FUNGAL INFECTION AND SCABIES:
|
DISEASE FUNGAL |
TOTAL BURDEN |
PERCENTAGE (%) |
|
INFECTION |
411997 |
94.85% |
|
SCABIES |
22332 |
5.14% |
|
TOTAL |
434329 |
100% |
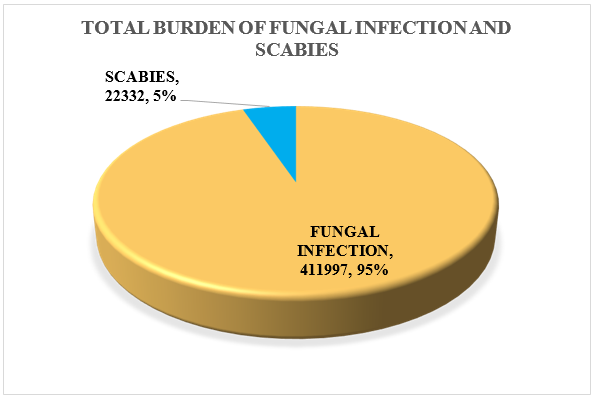
Graph 6.3. Total Burden of Fungal Infections and scabies.
REFERENCES
- Nair PA, Vora RV, Jivani NB, Gandhi SS. (2016). A Study of Clinical Profile and Quality of Life in Patients with Scabies at a Rural Tertiary Care Centre. J Clin Diagn Res. 10(10):WC01-WC05.
- Behera P, Munshi H, Kalkonde Y, Deshmukh M, Bang A. (2021). Control of scabies in a tribal community using mass screening and treatment with oral ivermectin -A cluster randomized controlled trial in Gadchiroli, India. PLoS Negl Trop Dis. 15(4):e0009330.
- Kavita A, Thakur JS, Narang T. (2023). The burden of skin diseases in India: Global Burden of Disease Study 2017. Indian J Dermatol Venereol Leprol. 89(3):421-425.
- Evening Primrose Oil: Why It’s the Best Skin Moisturizer [Internet]. LOA SKIN. Available at: https://loaskin.com/blogs/loa-skin-care/evening-primrose-oil-skin-benefits
- Mayo Clinic. (2018). Ringworm (body) - Symptoms and causes [Internet]. Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/ringworm-body/symptoms-causes/syc-20353780
- Al Aboud AM, Crane JS. (2020). Tinea Capitis [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK536909/
- Jock itch - Symptoms and causes [Internet]. Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/jock-itch/symptoms-causes/syc20353807#:~:text=Jock%20itch%20is%20a%20Fungal
- Tinea Versicolor: Symptoms, Causes, Treatments [Internet]. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/17719-tinea-versicolor
- Nigam PK, Saleh D. (2020). Tinea Pedis [Internet]. StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK470421/
- Elewski BE. (1998). Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 11(3):415-429.
- Australian Journal of General Practice. (2022). Superficial Fungal Infections. Available at: https://www1.racgp.org.au/ajgp/2019/october/superficial-Fungal-Infections
- Reddy GKK, Padmavathi AR, Nancharaiah YV. (2022). Fungal infections: Pathogenesis, antifungals and alternate treatment approaches. Curr Res Microb Sci. 3:100137.
- Jaypee Digital. AntiFungal Drugs [Internet]. www.jaypeedigital.com. Available at: https://www.jaypeedigital.com/book/9789385999840/chapter/ch31
- Chiu S, Argaez C. (2019). Ivermectin for Parasitic Skin Infections of Scabies: A Review of Comparative Clinical Effectiveness, Cost-Effectiveness, and Guidelines [Internet]. PubMed. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health.
- Scabies Patho. PDF. Medical Specialties. Wellness [Internet]. Scribd. Available at: https://www.scribd.com/doc/37257420/Scabies-Patho
- Deb P, Mohanty I, Slathia I, Verma V. (2017). Drug utilisation and selfmedication pattern of anti-Fungal drugs in dermatology outpatient department of a tertiary care hospital. Int J Basic Clin Pharmacol. 6(9):2189-2192.
- Dehkharghani S, Bible J, Chen JG, Feldman SR, Fleischer AB Jr. (2003). The economic burden of skin disease in the United States. J Am Acad Dermatol. 48(4):592-599.
- Naaz R, Chand S, Up N, Bc V, Kc BR, Shetty S. (2021). Prospective Observational Study on Prescribing Pattern of AntiFungal Drugs in the 400 Out-Patient Department of Dermatology in a Tertiary Care Hospital. Biomedical and Pharmacology Journal. 14(1):311-316.
- Bansal P, Baishnab S, Singla A. (2021). Drug prescribing pattern of antiFungal drugs for local Fungal Infections in a tertiary care hospital: MAMC, Agroha. Int J Basic Clin Pharmacol. 10(6):689-693.
- Amiri R, Shirooei B, Hajatifard S. (2015). DRUG UTILIZATION EVALUATION OF ANTIFUNGAL AGENTS IN OUTPATIENTS VISITING THE DERMATOLOGY DEPARTMENT OF A TERTIARY CARE HOSPITAL IN INDIA. World Journal of Pharmacy and Pharmaceutical Sciences. 11(6):977-983.
- Ray A, Aayilliath K A, Banerjee S, Chakrabarti A, Denning DW. (2022). Burden of Serious Fungal Infections in India. Open Forum Infect Dis. 9(12):ofac603.
- Butt AQ, Bangash FA, Abbas H. (2010). Burden of Skin Diseases at a Tertiary Care Hospital. Available at: https://journalrmc.com/index.php/JRMC/article/view/664
- Urban K, Chu S, Giesey RL, Mehrmal S, Uppal P, Delost ME, et al. (2020). Burden of skin disease and associated socioeconomic status in Asia: A cross-sectional analysis from the Global Burden of Disease Study 1990-2017. JAAD Int. 2:40-50.
- Karimkhani C, Colombara DV, Drucker AM, Norton SA, Hay R, Engelman D, et al. (2017). The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. Lancet Infect Dis. 17(12):1247-1254.
- Campbell M, van der Linden N, Gardner K, Dickinson H, Agostino J, Dowden M, et al. (2022). Health care cost of crusted scabies in Aboriginal communities in the Northern Territory, Australia. PLoS Negl Trop Dis. 16(3):e0010288.
- Cox V, Fuller LC, Engelman D, Steer A, Hay RJ. (2021). Estimating the global burden of scabies: what else do we need? Br J Dermatol. 184(2):237-242.
- Nair PA, Vora RV, Jivani NB, Gandhi SS. (2016). A Study of Clinical Profile and Quality of Life in Patients with Scabies at a Rural Tertiary Care Centre. J Clin Diagn Res. 10(10):WC01-WC05.
- Walle TA. (2023). Prevalence of Scabies and associated factors among Governmental Elementary School Students in Gondar town Northwest Ethiopia. J Pract Prof Nurs. 7(3):1-6.
- Belachew SA, Kassie A. (2018). Burden and drivers of Human Scabies among children and adults in Northwestern Ethiopia: The case of the neglected tropical disease. International Journal of Infectious Diseases. 73:317.
- Urban K, Giesey RL, Delost M, Delost GR. (2020). An Update on the Global Burden and Socioeconomics of Scabies. SKIN The Journal of Cutaneous Medicine. 4(6):534-542.
- Urban K, Chu S, Scheufele C, Giesey RL, Mehrmal S, Uppal P, et al. (2020). The global, regional, and national burden of fungal skin diseases in 195 countries and territories: A cross-sectional analysis from the Global Burden of Disease Study 2017. JAAD Int. 2:22-27.
- Pfavayi LT, Denning DW, Baker S, Sibanda EN, Mutapi F. (2021). Determining the burden of fungal infections in Zimbabwe. Sci Rep. 11(1):13240.
- Duong TN, Le MH, Beardsley J, Denning DW, Le NH, Nguyen BT. (2023). Updated estimation of the burden of fungal disease in Vietnam. Mycoses. 66(4):346-353.
- Al-Hatmi AMS, Al-Shuhoumi MA, Denning DW. (2020). Estimated Burden of Fungal Infections in Oman. J Fungi (Basel). 7(1):5.
- Bongomin F, Gago S, Oladele RO, Denning DW. (2017). Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. J Fungi (Basel). 3(4):57.
- Jaishi VL, Parajuli R, Dahal P, Maharjan R. (2022). Prevalence and Risk Factors of Superficial Fungal Infection among Patients Attending a Tertiary Care Hospital in Central Nepal. Interdiscip Perspect Infect Dis. 2022:3088681.
- Hay RJ, Steer AC, Engelman D, Walton S. (2012). Scabies in the developing world--its prevalence, complications, and management. Clin Microbiol Infect. 18(4):313-323.
- Giesey RL, Mehrmal S, Uppal P, Delost ME, Delost GR. (2020). Dermatoses of the Caribbean: Burden of skin disease and associated socioeconomic status in the Caribbean. JAAD Int. 1(1):3-8.
- Turan Ç, Metin N. (2021). Impact of Pandemic in the Frequency of Scabies: Possible Scabies Outbreak Scenario Aftermath COVID-19. Turkiye Parazitol Derg. 45(3):190-194.
- El-Moamly AA. (2021). Scabies as a part of the World Health Organization roadmap for neglected tropical diseases 2021-2030: what we know and what we need to do for global control. Trop Med Health. 49(1):64.
- Karimkhani C, Dellavalle RP, Coffeng LE, Flohr C, Hay RJ, Langan SM, et al. (2017). Global Skin Disease Morbidity and Mortality: An Update From the Global Burden of Disease Study 2013. JAMA Dermatol. 153(5):406-412.
- Hay RJ, Johns NE, Williams HC, Bolliger IW, Dellavalle RP, Margolis DJ, et al. (2014). The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 134(6):1527-1534.
- Elezbawy B, Fasseeh AN, Fouly E, Tannira M, Dalle H, Aderian S, et al. (2023). Humanistic and Economic Burden of Atopic Dermatitis for Adults and Adolescents in the Middle East and Africa Region. Dermatol Ther (Heidelb). 13(1):131-146.
- Government NT. (2023). Scabies and crusted Scabies [Internet]. health.nt.gov.au. Available at: https://health.nt.gov.au/public-health-notifiable-diseases/Scabies
- Burden of skin disease [Internet]. www.aad.org. Available at: https://www.aad.org/member/clinical-quality/clinical-care/bsd
- File:3D medical animation skin layers.jpg. 2020. Wikipedia [Internet]. commons.wikimedia.org. Available at: https://en.m.wikipedia.org/wiki/File:3D_medical_animation_skin_layers.jpg
- Bell H. (2020). Tinea corporis. dermnet NZ [Internet]. dermnetnz.org. Available at: https://dermnetnz.org/topics/tinea-corporis
- Tinea Capitis [Internet]. The London Skin And Hair Clinic. Available at: https://www.thelondonskinandhairclinic.com/tinea-capitis/
- Jock Itch: What It Is, Symptoms & Treatment [Internet]. Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/22141-jock-itch-tineacruris
- Mayo Clinic. (2018). Tinea versicolor - Symptoms and causes [Internet]. Mayo Clinic. Available at: https://www.mayoclinic.org/diseases- conditions/tineaversicolor/symptoms-causes/syc-20378385
- Johnson S. (2012). Everything You Need to Know About Scabies [Internet]. Healthline. Healthline Media. Available at: https://www.healthline.com/health/Scabies
- The Healthline Editorial Team. (2018). Athlete’s Foot (Tinea Pedis) [Internet]. Healthline. Healthline Media. Available at: https://www.healthline.com/health/athletes-foot
- Fungal Nail Infections (Tinea Unguium) - Kerry Skin Clinic [Internet]. www.kerryskinclinic.ie. [cited 2024 Apr 6]. Available at: https://www.kerryskinclinic.ie/services/hair-and-nail-problems/105nails/389-Fungal-nail-Infections-tinea-unguium
- Gupta S, Khan W, Krishna A. (2016). Pattern of skin diseases and common drugs prescribed in dermatology OPD of an Indian tertiary care hospital. Int J Basic Clin Pharmacol. 6(1):203.