Information Links
Related Conferences
Previous Issues Volume 11, Issue 1 - 2026
The Role of Relative Determination of the Right Lung Volume by the Diaphragmatic Index in the Diagnosis of Pulmonary Atelectasis
Michael D Levin*
Dorot. Medical Center for Rehabilitation and Geriatrics, Netanya, Israel
*Corresponding Author: Michael D Levin, MD, Ph.D, Dorot. Medical Center for Rehabilitation and Geriatrics, Department of Pediatric Radiology of the 1-st State Hospital, Minsk, Belarus, Dorot. Medical Center for Rehabilitation and Geriatrics, Amnon veTamar, Netanya, Israel, Tel: 972-538281393, Email: [email protected]
Received Date: February 10, 2026
Published Date: February 27, 2026
Citation: Levin MD. (2026). The Role of Relative Determination of the Right Lung Volume by the Diaphragmatic Index in the Diagnosis of Pulmonary Atelectasis. Mathews J Case Rep. 11(1):217.
Copyrights: Levin MD. © (2026).
ABSTRACT
Introduction: Radiographic signs of pulmonary atelectasis have been described in the literature and include elevation of the diaphragm on the side of atelectasis, compensatory overinflation of the contralateral lung, mediastinal shift, cardiac rotation, and changes in pulmonary vessels and ribs. These signs are largely descriptive and lack clear quantitative standards. Although CT and MRI provide higher diagnostic accuracy, plain chest radiography remains more accessible and cost-effective. Seventy-five patients with pulmonary atelectasis detected by us on chest radiographs were admitted to a rehabilitation and geriatric medical center from other hospitals; however, only two of them had a prior diagnosis confirmed by CT, while the remaining cases were diagnosed as recurrent pneumonia. Methods: To diagnose atelectasis, we applied a method for determining the relative volume of the right lung using the diaphragmatic index (DI). A horizontal baseline was drawn on the chest of radiograph along the lower edge of the tenth thoracic vertebra. A vertical line was drawn from the highest point of the right diaphragmatic dome to the baseline, and its length was recorded in centimeters with a positive or negative sign depending on its position relative to the baseline. A second vertical line was drawn from the intersection of the baseline with the right chest wall to the costophrenic sinus and measured similarly. The diaphragmatic index was calculated as the sum of these two values. In healthy individuals with normal breathing, the DI ranges from 0 to +5. Results: Diagnostic accuracy of conventional radiographic assessment was compared with evaluation incorporating the DI. In the entire cohort, the use of DI increased diagnostic accuracy by 39%. The increase was 27% for right-sided atelectasis, 31% for left-sided atelectasis, and 68% for bilateral atelectasis. The analysis demonstrated that hyperinflation of the lung contralateral to atelectasis represents not merely an indirect radiographic sign but a physiological phenomenon, the absence of which indicates additional pathology. Conclusion: Treatment strategies aimed at preventing recurrent pneumonia and facilitating patient rehabilitation depend on timely diagnosis of atelectasis. The use of the proposed quantitative method for evaluating chest radiographs increases the diagnostic accuracy of atelectasis by 39% compared with standard descriptive assessment.
Keywords: Chest X-Ray, Atelectasis, Bronchiectasis, Pneumonia, Diaphragmatic Index, Diagnosis.
INTRODUCTION
Atelectasis literally means incomplete expansion of the lung and refers to any condition associated with a loss of lung volume. It is usually, though not invariably, accompanied by an increase in radiographic density. The most common form is obstructive (resorptive) atelectasis, which develops secondary to complete endobronchial obstruction of a lobar bronchus, followed by resorption of gas distal to the obstruction. The pathophysiological mechanism involves a reduction in the sum of partial gas pressures in venous blood perfusing the atelectatic region, leading to gradual resorption of trapped air. Continued secretion into small airways results in consolidation and post-obstructive pneumonitis or bacterial infection. In patients with impaired cough, the most frequent cause of bronchial obstruction is a mucus plug; less common causes include bronchial tumors or passive atelectasis associated with hydrothorax [1,2]. Bronchiectasis is defined as an abnormal and permanent dilation of the bronchi. It may develop relatively rapidly—sometimes within months to a few years—following persistent lung pathology such as atelectasis, particularly in the setting of repeated infections and chronic inflammation. Although clinical manifestations often appear later, the underlying structural damage may progress earlier. In such cases, bronchiectasis typically develops within the collapsed segment of the lung, resulting in a sustained reduction of lung volume compared with normal values [1-3].
The radiographic manifestations of atelectasis include localized increased lung density, crowding of pulmonary vessels, rearrangement of bronchial structures, displacement of fissures and the pulmonary hilum, mediastinal shift, elevation of the hemidiaphragm, cardiac rotation, approximation of ribs, and compensatory overinflation of the contralateral lung. However, these findings are largely descriptive, lack quantitative comparison with normal standards, and are neither consistently present nor uniformly reliable. For example, localized increased lung density is rarely evident in atelectasis of the right lower lobe because compaction of lung tissue is frequently obscured by the hepatic shadow. Cardiac rotation represents a pathological phenomenon rather than a direct radiographic sign; its radiographic manifestation is inferred from disappearance or marked reduction of the pulmonary hilum on the side of atelectasis. More reliable indicators include elevation of the hemidiaphragm and mediastinal shift toward the affected side, although these signs may be absent in cases with compensatory hyperinflation of the remaining lung segments.
The aim of this study was to increase the diagnostic value of plain chest radiography in the detection of pulmonary atelectasis. To achieve this, we applied a quantitative method for assessing relative lung volume that was protected by a copyright certificate in 1988 [4]. The normal reference values and diagnostic accuracy of this method were previously reported in two publications [5,6].
Method for determining the relative volume of the right lung on a plain chest radiograph
The diaphragmatic domes are anatomically attached to the tenth thoracic vertebra. During inspiration, the diaphragmatic domes descend, resulting in an increase in lung volume as air is drawn into the lungs. During expiration, the domes ascend, reducing lung volume by expelling air. This physiological relationship forms the basis for a quantitative assessment of lung volume using plain chest radiography. To determine the relative volume of the right lung, a horizontal reference line (baseline) was drawn on the chest radiograph along the lower edge of the tenth thoracic vertebra. Along the right midclavicular line, a perpendicular vertical line was drawn from the highest point of the right diaphragmatic dome to the baseline. If the dome was located above the baseline, the measured distance in centimeters was assigned to have a positive value; if below the baseline, a negative value was assigned. A second vertical line was drawn from the intersection of the baseline with the right lateral chest wall to the deepest point of the right costophrenic sinus. The length of this line was also measured in centimeters and assigned a positive or negative value depending on whether its upper end was located above or below the baseline. The diaphragmatic index (DI), representing an integral quantitative characteristic of right lung volume, was calculated as the sum of the diaphragmatic dome height and the sinus depth (Figure 1). Previous studies conducted in individuals without pulmonary pathology demonstrated that, under conditions of normal breathing, DI values range from 0 to +5 [5,6].
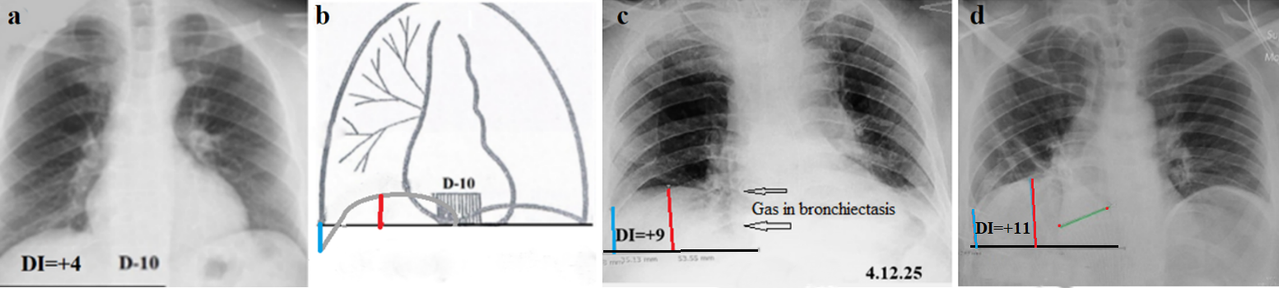
Figure 1. The principle of the proposed method. (a). Location of the diaphragm in a patient with a normal right lung volume. (b). Schematic for Figure 1.a. (c). In the chest radiograph the gas-filled bronchiectasis (arrows on the right) are visible. There are no shadows above the diaphragm, and no difference in diaphragmatic height on either side. However, the cardiac shadow is displaced to the left and rotated, as evidenced by the absence of the right hilus. (d). Atelectasis of the lower lobe on the right is visible against the liver shadow as a lighter triangular shadow (green line). The atelectasis occupies the same location as the bronchiectasis in Figure 1c. In both cases (c, d), the DI was greater than normal, indicating a decrease in the volume of the right lung.
Patients
We analyzed chest radiographs of 75 patients aged 50 to 86 years who were admitted to the Medical Center for Rehabilitation and Geriatrics between 2019 and 2025 with a diagnosis of respiratory failure. Unlike other patients with respiratory failure, these individuals were diagnosed with pulmonary atelectasis upon admission based on radiographic analysis. Most patients were referred to by other hospitals. Only 2 of the 75 patients (3%) were admitted with a diagnosis of pulmonary atelectasis established by chest CT. In the remaining cases, the cause of respiratory failure was recorded as recurrent pneumonia. All patients were divided into three groups according to the initial radiographic findings. The first group included 30 patients in whom atelectasis was initially diagnosed in the right lung. The second group consisted of 26 patients whose initial chest radiographs demonstrated atelectasis in the left lung. The third group included 19 patients who were admitted with radiographic evidence of atelectasis involving both lungs. The most patients were severely ill and had significant comorbidities, including recent myocardial infarction, stroke, and various surgical interventions. Longitudinal follow-up with serial chest radiographs was available in 54 patients, allowing assessment of radiographic dynamics over the course of prolonged hospitalization.
RESULTS
Right Lung Atelectasis
Atelectasis of the right lung was diagnosed on admission in 30 patients. Most of them were referred from other hospitals with a diagnosis of recurrent aspiration and had repeatedly received antibiotic therapy during febrile episodes. A representative example is shown in Figures 2a and 2b. In 21 of the 30 patients, right lung volume was markedly reduced compared with normal. This was manifested by elevation of the right diaphragmatic dome, rightward displacement of the cardiac silhouette, and a clear reduction in right lung volume relative to the left. In these patients, the diaphragmatic index ranged from 6 to 16 (mean, 12.4) (Figure 2b). Typical radiographic signs of atelectasis were present in 17 of these 21 patients, while in 4 cases the findings were equivocal. In these latter cases, an increased DI indicating significant reduction in right lung volume allowed confirmation of the diagnosis of atelectasis. In three patients with right-sided atelectasis, the DI values were within the normal range (2 to +5). In two of these cases, hyperinflation of the right upper lobe was present (Figure 2c), whereas in one case there was a marked rightward mediastinal shift (Figure 2d). Despite normal DI values, the conventional radiographic findings in these three patients were sufficiently convincing to establish the diagnosis of atelectasis. During follow-up, six patients developed atelectasis of the left lung. In four of these six patients, conventional radiographic signs of left-sided atelectasis were absent (Figure 2a). In these cases, the diagnosis of atelectasis was established solely based on a DI value greater than 5 (Figure 1a) (Table 1).
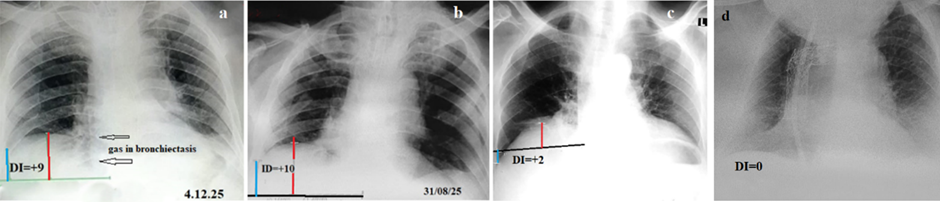
Figure 2. Chest radiographs showing atelectasis of the lower lobe of the right lung. (a). Right lower lobe atelectasis with gas-filled bronchiectasis (arrows). DI=+9 indicates right lung volume reduction despite the absence of radiographic evidence of atelectasis, which is due to the development of atelectasis on the other side. (b). The same patient showed signs of right-sided atelectasis on an X-ray 3.5 months ago. There was no pathology over the left dome of the diaphragm. He was treated as a patient with pneumonia using Intrapulmonary Percussive Ventilation (IPV) for sputum removal, which resulted in the spread of infection to the left lung [7]. (c). The right dome of the diaphragm is higher than the left. It has risen to the level of the hilum of the right lung, but the cardiac shadow is shifted to the left. DI=+ 2 is within the normal range because of hyperinflation of the right upper lobe, as evidenced by increased lucency and rare pulmonary pattern. (d). A triangular shadow of atelectasis of the lower lobe of the right lung is visible. DI= 0 is within normal limits because the cardiac shadow and mediastinum are shifted to the right, and the upper lobe of the right lung is stretched in the craniocaudal direction.
Table 1. Shows the statistical results of different variants of atelectasis of the right lung
|
Groups |
Number |
Min - Max |
M |
X-ray signs of atelectasis |
|
|
Yes |
No |
||||
|
DI >5 |
21 (69%) |
6 - 15 |
12.4 |
17 |
4 |
|
DI<5 |
3 (10%) |
0 – 3 |
-1.7 |
3 |
|
|
+ Lt atelectasis |
6 (21%) |
4 - 17 |
11.0 |
2 |
4 |
|
Total |
30 |
|
|
|
8 |
+ Lt atelectasis – is a case where atelectasis of the right side was complicated by atelectasis of the left side.
The statistical summary of different variants of right lung atelectasis is presented in Table 1. The use of the diaphragmatic index increased the diagnostic accuracy of right-sided atelectasis in 4 of 21 patients and enabled detection of left-sided atelectasis resulting from disease progression in 4 of 6 patients. Overall, incorporation of the DI provided additional diagnostic information in 8 of the 30 patients (27%). Notably, none of the 30 cases demonstrated convincing radiographic evidence of hyperinflation of the left lung.
Left Lung Atelectasis
The most common radiographic findings on admission were those typically described in the literature: leftward displacement of the cardiac silhouette, elevation of the left hemidiaphragm, disappearance or marked reduction of the left pulmonary hilum due to cardiac rotation, decreased volume of the left lung, and hyperinflation of the right lung (Figure 3a). Hyperinflation, defined as an increase in right lung volume quantified by a decrease in the diaphragmatic index (DI) below the lower limit of normal (i.e., < 0), was detected in 18 of 22 cases, with a mean DI of −4.5. The use of a mathematical parameter increased the reliability of this sign and allowed assessment of its dynamics. In many cases, the atelectatic shadow was visible against the background of the cardiac silhouette (Figure 3a, c, d). In 4 of the 22 patients with a negative DI, several radiographic features did not correspond to the typical pattern. In one case, both diaphragmatic domes were at the same level despite atelectasis of the left lower lobe (Figure 3b). In three cases, the right hemidiaphragm was higher than the left (Figure 3c). In four patients with a positive DI, the right hemidiaphragm was also higher than the left (Figure 3d, e). In two of these patients, serial radiographs documented progression of the process, with an increase in DI indicating the development of atelectasis in the right lung (Figure 3d–e). In six patients with left lung atelectasis, the gastric air bubble was not located directly beneath the diaphragmatic dome but was separated from it by 3–7 cm. In four of these cases, the gas bubble was deformed, as if compressed from above (Figure 3b).
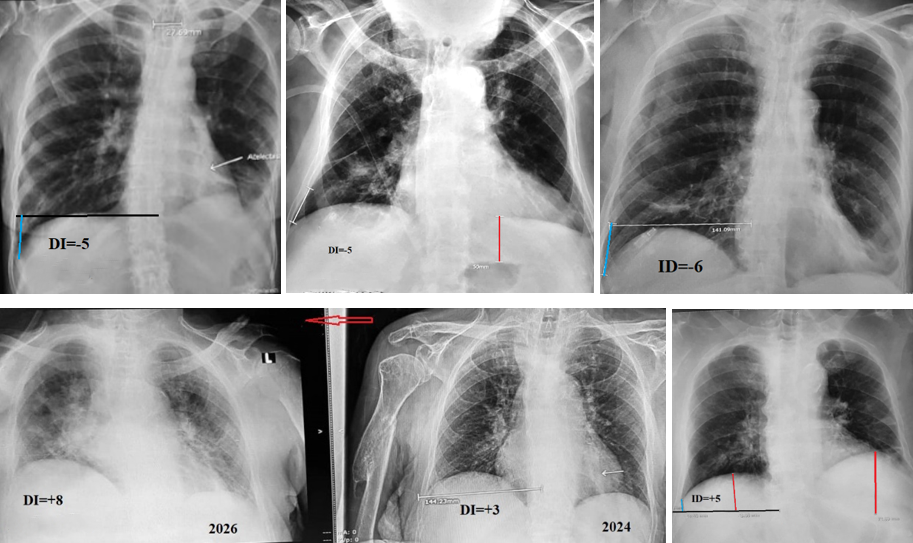
Figure 3. Radiographs of patients admitted to atelectasis at the base of the left lung. (a). Typical picture of atelectasis in the left lung (arrow) with hyperventilation of the right lung (DI=-5). (b). Patient with increased volume of both lungs (DI=-5). Both diaphragms are at the same level. Atelectasis of the lower lobe on the left displaces the gas bubble of the stomach downwards. Inflammatory changes on the right, together with other signs, indicate atelectasis also at the base of the right lung. (c). In a patient with atelectasis on the left, the right dome of the diaphragm is higher than the left one. Above it, there are inflammatory changes confirming atelectasis also at the base of the right lung. (d-e). In 2024, atelectasis was visible on the left and atelectasis was suspected on the right. In 2026, atelectasis was evident on both sides. (f). Leftward displacement of the heart, elevation of the left dome of the diaphragm, and a decrease in the volume of the left lung are accompanied by an inflammatory reaction in the root of the right lung and the absence of hyperinflation. This confirms atelectasis on the right (Table 2).
Table 2. Presents the statistical results of different variants of left lung atelectasis.
|
Groups |
Number |
Min - Max |
M |
Changes on the right |
|
|
Inflammation |
Atelectasis |
||||
|
DI < 5 |
22 (85%) |
1 - (-9) |
- 4.5 |
12 |
4 |
|
D I>5 |
4 (15%) |
2 - 5 |
1.7 |
|
4 |
|
Total |
26 |
|
|
|
8 |
Hyperinflation of the right lung was detected in 18 (69%) of 26 patients with left lung atelectasis. Analysis of these observations suggests that hyperinflation is not merely an accompanying radiographic sign but a physiological compensatory response. In eight patients (four with a negative DI and four with a DI within the normal range), some classical radiographic signs of left lung atelectasis were absent. Further analysis demonstrated that this was due to concomitant atelectasis of the right lung (Table 2). Indeed, only 6 (27%) of the 22 patients with a negative DI showed no inflammatory changes on the right. In 12 cases (55%), inflammatory changes were present, and in 4 (18%), atelectasis of the right lung was diagnosed. Dynamic follow-up showed that periodic reflux of infected bronchiectasis contents from the left lung leads to the spread of inflammation and subsequent development of atelectasis in the right lung. Thus, the use of DI not only clarified the pathophysiology of atelectasis but also allowed diagnosis of atelectasis in 8 (30%) of 26 patients in whom it was not initially suspected.
Atelectasis at the Bases of Both Lungs
Nineteen patients were admitted with a diagnosis of bilateral recurrent pneumonia; however, in all cases, radiographic evidence of atelectasis was already present on admission. In 13 cases (68%), the diagnosis of bilateral atelectasis was possible only based on DI > 5, which ranged from 6 to 14 (mean 9.8). This indicated a marked reduction in lung volume despite both diaphragmatic domes being at the same level (Figure 4a, d). In three cases, the right hemidiaphragm was significantly higher than the left (Figure 4e). Nevertheless, dynamic imaging (Figure 4d–f) demonstrated a substantial reduction in the volume of both lungs on all radiographs. Atelectasis of the left lung was further supported by a significant distance between the left hemidiaphragm and the gastric air bubble in five patients (Figure 4c–f, red line), whereas normally the gastric bubble lies directly beneath the diaphragm. In three additional cases, the left hemidiaphragm was higher than the right, but no hyperinflation of the right lung was observed. Instead, the right lung volume was below normal, as indicated by a DI > 5. In at least 13 (68%) of the 19 patients with bilateral atelectasis and symmetrical diaphragm position, all conventional radiographic signs of atelectasis were absent. Only a marked reduction in lung volume, quantified by DI, enabled correct diagnosis, which was subsequently confirmed during follow-up.
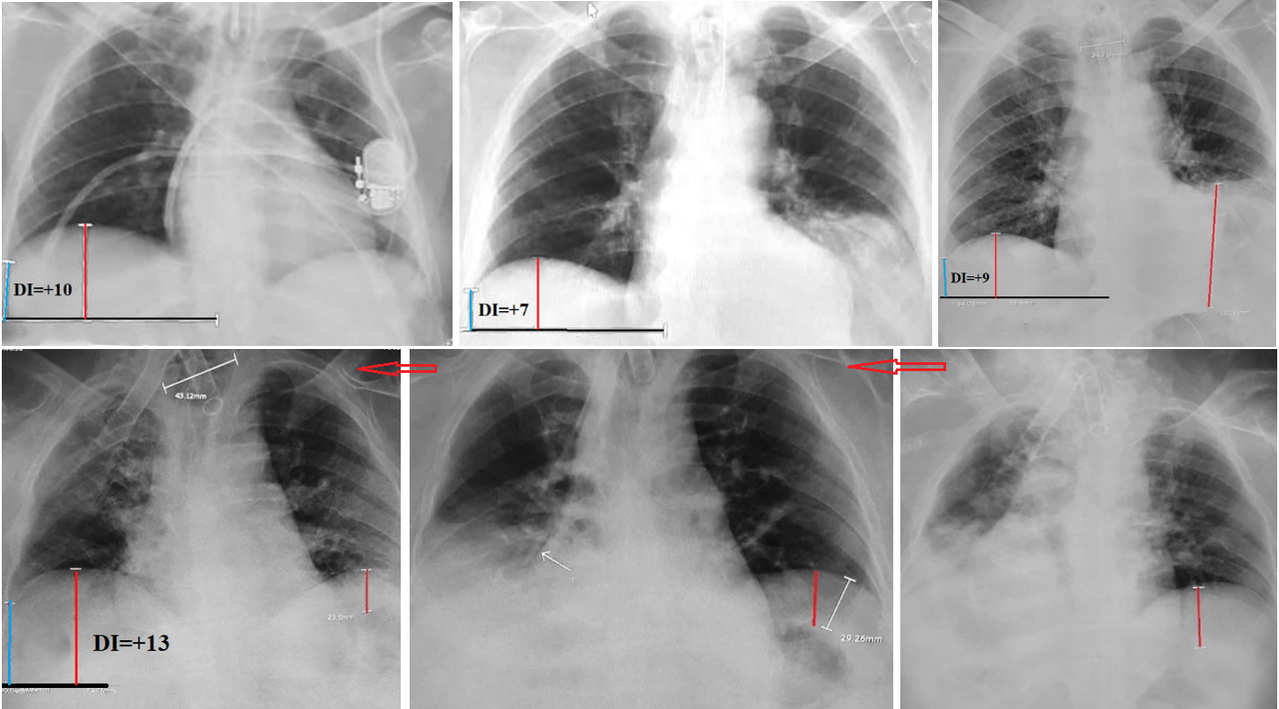
Figure 4. Radiographs of patients admitted with bilateral atelectasis. (a). In a patient with tracheal intubation, shows inflammatory changes above the diaphragm on both sides, but there are no typical signs of atelectasis. The right dome of the diaphragm is slightly higher than the left, as is normal. DI = +10 indicates a significant decrease in the volume of the right lung due to atelectasis. (b, c). A sharp rise of the left diaphragm does not raise doubts about atelectasis on the left. However, it is not accompanied by hyperventilation of the right lung. The volume of right lung is clearly reduced, since DI> 5. (d, e, f). The patient was admitted with a diagnosis of recurrent pneumonia. Despite the radiographic conclusion about bilateral atelectasis, he received antibiotics for 4 months after each attack of shortness of breath accompanied by high fever. Since these cases were considered aspiration of food or gastric contents, doctors gradually inflated the balloon on the tracheostomy tube, increasing its diameter to 4 cm (see d). In Figure 3e, the arrow indicates bronchiectasis containing air after infected mucus was expelled into the bronchi of the right lung. Atelectasis of the left lung is suggested by both the decreased lung volume and the distance between the left dome of the diaphragm and the gastric bubble.
Table 3. Presents the statistical results of different variants of atelectasis on both sides
|
Groups |
Number |
Min - Max |
M |
Which diaphragm dome was higher? |
||
|
DI >5 |
19 |
6 - 14 |
9.8 |
Equal |
Rt |
Lt |
|
13 (68%) |
3 (16%) |
3 (16%) |
||||
|
Total |
19 |
|
|
13 |
3 |
3 |
In at least 13 (68%) of the 19 patients with bilateral anelectasis and symmetrical diaphragm position, all conventional radiographic signs of atelectasis were absent. Only a marked reduction in lung volume, quantified by DI, enabled correct diagnosis, which was subsequently confirmed during follow-up.
DISCUSSION
In this study, the hypothesis that hyperinflation develops in the lung contralateral to atelectasis was objectively confirmed through digital analysis of cases with left basal atelectasis. In 18 (69%) of 26 patients, the DI was below the minimum normal limit (mean −4.5), indicating hyperinflation. However, in four patients with a negative DI, the right hemidiaphragm was higher than the left. Similarly, in all four patients with a positive DI (mean +1.7), the right hemidiaphragm was higher. Dynamic follow-up in these eight patients demonstrated that absence of hyperinflation is indicative of atelectasis at the base of the right lung. The presence of hyperinflation of the left lung in cases of right-sided basal atelectasis—was less convincing for two reasons: (1) the right hemidiaphragm is normally higher than the left, and (2) there are no numerical standards defining the position of the left hemidiaphragm relative to bony landmarks. Nevertheless, there is strong reason to assume that the pathophysiology of unilateral atelectasis is symmetrical. Thus, we conclude that hyperventilation of the lung contralateral to atelectasis is primarily a physiological phenomenon and only secondary a radiographic sign of atelectasis. In review Ashizawa at all the pitfalls in the diagnosis of lobar atelectasis on chest radiographs. It is shown that Lobar atelectasis with marked volume loss is hard to recognize and may be easily missed. It presenting as a mass-like opacity may be misdiagnosed as mediastinal or lung tumor [7]. The improvement in diagnostic accuracy achieved using DI is summarized in Table 4.
Table 4. The contribution of mathematical analysis of radiographs using DI
|
Location of Atelectasis |
Number of Cases |
Known X-Ray Features |
Including DI |
|
Right |
30 |
22 |
8 (27%) |
|
Left |
26 |
18 |
8 (31%) |
|
From both sides |
19 |
6 |
13 (68%) |
|
Total |
75 |
46 (61%) |
29 (39%) |
In 11 patients with left-sided atelectasis, a previously undescribed sign was observed: a gap of 4–7 cm between the diaphragmatic dome and the gastric air bubble. Given its high prevalence exclusively in left-sided atelectasis and gas bubble deformation in some of them, as well as its absence in other radiographs its absence in other radiographs, we propose this finding as a potential radiographic sign of left lung atelectasis. Confirmation using other imaging modalities is required. Only 2 (3%) of the 75 patients had a diagnosis of atelectasis prior to admission, established by CT. In all other cases diagnosis of the referring hospitals was “recurrent pneumonia.” Although modern imaging techniques such as CT and MRI surpass chest radiography in diagnostic accuracy, they are more expensive, less accessible, and unsuitable for frequent monitoring, particularly in long-term care settings for severely ill, bedridden patients. There is therefore no justification for relying on chest radiography while ignoring the classical signs of atelectasis described in educational literature [1-3]. Treatment strategy depends directly on the diagnosis. When recurrent pneumonia is attributed to aspiration of food or gastric contents, management includes antibiotics and inflation of the tracheostomy tube balloon (if present). In atelectasis, fever and pulmonary infiltrates result from infected mucus periodically expelled from bronchiectasis cavities into the lungs. In such cases, periodic aspiration of bronchiectasis contents is required to prevent dissemination of infection. Between 2019 and 2025, treatment strategy gradually shifted. Instead of prescribing antibiotics during recurrent febrile episodes, drainage of secretions via catheterization of the affected lobe was increasingly employed. This prevented regurgitation of infected secretions into the lungs. As febrile episodes decreased, the number of chest radiographs declined, and contralateral lung infections became less frequent. The clinical outcomes of this paradigm shift will be presented in a separate publication.
CONCLUSION
Effective prevention of recurrent pneumonia and successful patient rehabilitation depend on timely diagnosis of atelectasis. Use of the proposed radiographic evaluation method increased diagnostic accuracy by 39% compared with standard radiographic assessment.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST
The author has no conflict of interest.
REFERENCES
- Radiology Review Manual. (1993). Dähnert, Wolfgang. Publisher, Williams & Wilkins. 2nd Edn. pp. 295-296.
- Fundamental of diagnostic radiology /edited by William E. Brant, Clide A. Helms. Copyrith © 1994 Williams & Wilkins. p.414-418.
- Brant & Helms' Fundamentals of Diagnostic Radiology: by Jeffrey Klein MD FACR & Vincent Mellnick. eBook with Multimedia. (2025). Sixth Edition.
- Levin MD. (1988). Author's certificate for the invention "Method for diagnosing widespread pulmonary inflation. State Committee for Inventions and Discoveries, USSR. SU 1651861 A1.
- Levin MD. (1988). Method for determining lung volume and its role in the diagnosis of certain diseases in children. Zdravoochranenie Belorussii. 11:51-55.
- Levin MD, Averin VI, Degtyarev YG, Bolbas TM. (2022). Method for Determining the Volume of the Right Lung and its Role in the Diagnosis of Some Lung Diseases. Novosti Khirurgii. 30(5):447-452.
- Ashizawa K, Hayashi K, Aso N, Minami K. (2001). Lobar atelectasis: diagnostic pitfalls on chest radiography. Br J Radiol. 74(877):89-97.