Previous Issues Volume 1, Issue 4 - 2016
The CT and MRI Findings of Fibrinous Sialodochitis
Ai Usami1, Naoya Kakimoto2, Tomonao Aikawa3, Sosuke Takahata3, Mitsunobu Kishino4, Ryoko Okahata1, Tomomi Tsujimoto1, Yuka Uchiyama1, Tadashi Sasai1, Shumei Murakami1
Ai Usami1, Naoya Kakimoto2, Tomonao Aikawa3, Sosuke Takahata3, Mitsunobu Kishino4, Ryoko Okahata1, Tomomi Tsujimoto1, Yuka Uchiyama1, Tadashi Sasai1, Shumei Murakami1
1Department of Oral and Maxillofacial Radiology, Osaka University Graduate School of Dentistry.
2Department of Oral and Maxillofacial Radiology, Applied Life Sciences, Institute of Biomedical & Health Sciences, HiroshimaUniversity.
3The First Department of Oral and Maxillofacial Surgery, Osaka University Graduate School of Dentistry.
4Department of Oral Pathology, Osaka University Graduate School of Dentistry.
Corresponding Author: Ai Usami, Department of Oral and Maxillofacial Radiology, Osaka University Graduate School of Dentistry, 1-8 yamadaoka, Suita, Osaka 556-0871, Japan, Tel: +81-6-6879-2967; E-Mail: [email protected]
Received Date: 29 Sep 2016 Accepted Date: 17 Nov 2016 Published Date: 18 Nov 2016
Copyright © 2016 Usami A
Citation: Usami A, Kakimoto N, Aikawa T, Takahata S, et al. (2016). The CT and MRI Findings of Fibrinous Sialodochitis. Mathews J Case Rep 1(4): 019.
ABSTRACT
Fibrinous sialodochitis is a very rare disease in which the recurrent swelling of the salivary gland is caused by the obstruction of the glandular duct by a fibrinous material. Few studies have reported both the computed tomography (CT) and magnetic resonance imaging (MRI) findings of fibrinous sialodochitis. We reported a forty-nine-year-old man with this disease including CT and MRI findings. His chief complaint was the recurrent swelling of the bilateral submandibular regions. When his primary dentist pushed them strongly, a whitish jelly-like material and a large amount of clear saliva were expelled from the duct orifices of the submandibular glands. A CT and MRI findings showed the retention of saliva in the glandular duct and no abnormal sign of the glandular parts. On a cytological examination, the material included fibrinous substances and numerous eosinophils. According to clinical, radiological and cytological findings, the patient was diagnosed with fibrinous sialodochitis. The management included the massage to compress the salivary glands, the administration of antihistamines and steroids, and irrigation of the ducts of submandibular glands using a saline solution. The number of times of the swelling of the submandibular regions decreased.
KEYWORDS
Fibrinous Sialodochitis; Computed Tomography; Magnetic Resonance Imaging; Recurrent Swelling; Salivary Gland.
INTRODUCTION
Fibrinous sialodochitis is a very rare disease. It is characterized by the recurrent swelling of the salivary gland, which is caused by the obstruction of the duct by a fibrinous material. When the salivary glands are compressed, a fibrinous material is expressed from the duct orifice, and the swelling disappears [1, 2]. To our knowledge, there were only sixteen case reports about fibrinous sialodochitis in the English literature. However, few studies have reported both the computed tomography (CT) and magnetic resonance imaging (MRI) findings of fibrinous sialodochitis. We herein present a case of fibrinous sialodochitis and report the CT and MRI findings.
CASE REPORT
A forty nine-year-old man was referred for the evaluation and treatment of recurrent swelling in the submandibular region from a general dental clinic to Osaka University Dental Hospital. His chief complaint was the recurrent swelling of the bilateral submandibular region over a one-year period. He did not have pain or fever. His medical and family histories were unremarkable. On physical examination, the bilateral submandibular regions were found to be enlarged but were not tender on palpation (Figure 1a, 1b). When the submandibular areas were pushed strongly by his primary dentist, a whitish jelly-like material and a large amount of clear saliva were expelled from the duct orifices of the submandibular glands (Figure 2). Panoramic radiography and occlusal radiography showed no evidence of stones or calcification. To evaluate the patient's allergy status, a hematological examination was performed and the patient's serum immunoglobulin E (IgE) level was measured. The eosinophil and basophil counts and the serum IgE level were high. The patient's physical constitution was thought to be allergic.

Figure 1a, 1b: Photographs showing the swelling of the right (1a) and left submandibular regions (1b).
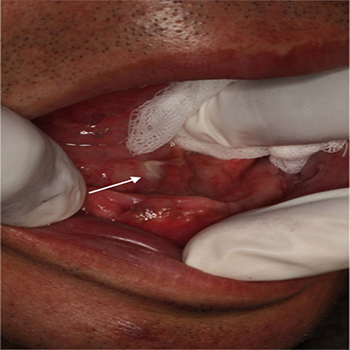
Figure 2: When the submandibular areas were pushed strongly, a whitish jelly-like material (white arrow) and a large amount of clear saliva were expressed from the duct orifice of the submandibular gland.
The CT, MRI and Cytological Findings
Axial CT images showed the diffuse swelling and many lowdensity areas in both submandibular glands (Figure 3a). Reformatted coronal and sagittal CT images showed bead-like lowdensity areas (Figure 3b, 3c). These findings corresponded to the dilatation of the glandular ducts. The CT values of the ten duct parts and ten glandular parts were measured (Figure 4). The CT values of ten duct parts ranged from -9 to 19 HU; the mean CT value was 4.7 HU. The CT values of the ten glandular parts ranged from 25 to 57 HU; the mean CT value was 44.2 HU. There was no evidence of sialoliths on the CT images.
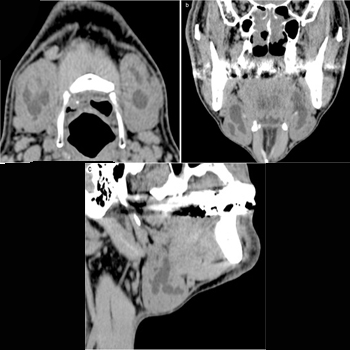
Figure 3a, 3b, 3c: An axial CT image on the hyoid bone level (3a). This showed the diffuse swelling of both submandibular glands and many low-density areas in both submandibular glands. The reformatted coronal CT image (3b) and the right side of the sagittal CT image (3c). These showed bead-like low-density areas.
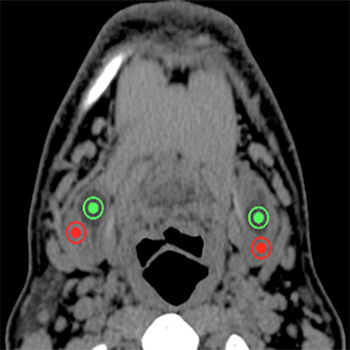
Figure 4: A sample CT image showing the measurement of the CT values of the ductal parts (green points) and glandular parts (red points) of the submandibular glands.
MRI showed many areas in the bilateral submandibular glands that had a low signal intensity on T1-weighted MRI and a water- like high signal intensity on fat suppressed (FS) T2-weighted MRI (Figure 5a, 5b). These findings suggested the retention of a large amount of saliva in the glandular duct. The glandular tissues showed a normal signal intensity on T1 and FS T2-weighted MRI.
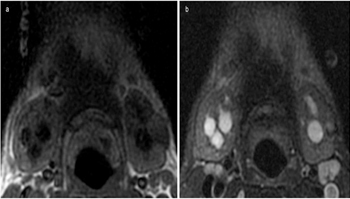
Figure 5a, 5b: MRI of the bilateral submandibular glands showing numerous areas with a low signal intensity on T1-weighted MRI (5a, TR: 500, TE: 7.664) and a water-like high signal intensity on FS T2-weighted MRI (5b,TR: 3600,TE: 76.64).
A cytological specimen of the fibrinous material was composed of fibrinous substances, numerous eosinophils and a small number of glandular cells (Figure 6). According to clinical, radiological and cytological findings, the patient was diagnosed with fibrinous sialodochitis.
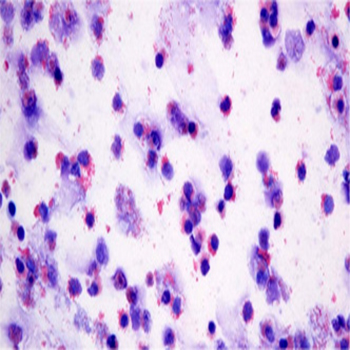
Figure 6: A cytological specimen of the fibrinous material showed that it was composed of fibrinous substances and numerous eosinophils (Giemsa staining).
TREATMENT
The management included the massage to compress the salivary glands, the administration of antihistamines and steroids, and irrigation of the ducts of submandibular glands using a saline solution. The swelling of the submandibular region still recurred over the following year, but it occurred less frequently.
DISCUSSION
Shimada et al. [2] reported that fibrinous sialodochitis and allergic parotitis could be considered to be the same disease. The English literature includes twenty three case studies about fibrinous sialodochitis or allergic parotitis. Chikamatsu et al. [3] reported that the secretion of a fibrinous material containing numerous eosinophils from the glandular duct orifices was a distinctive finding of fibrinous sialodochitis. Sixteen of the above-mentioned twenty-three articles mentioned this finding [1-6]. Among these sixteen reports, few articles included both CT and MRI findings. This represents the first report to show both the CT and MRI findings in a case of fibrinous sialodochitis of submandibular glands. The patient's chief complaint was the recurrent swelling of the bilateral submandibular regions over a one-year period. The pressure around the submandibular glands caused the extrusion of the fibrinous material followed by a gush of saliva. We suspected that the material might accompany the secondary bacterial infection of sialolithiasis, and performed a CT examination to detect sialoliths. Although no sialoliths were observed, the diffuse swelling of both submandibular glands and the bead-like dilation of submandibular glandular ducts were detected on the CT images. The CT values of the ten duct parts and ten glandular parts on this patient's CT images were measured. The mean CT value of the ten duct parts was 4.7 HU, which corresponded to saliva. This means that a large amount of saliva was retained in the submandibular glandular ducts. The mean CT value of the ten glandular parts was 44.2 HU, which corresponded to normal submandibular gland tissue (the CT value of the normal submandibular gland in a middle-aged male from the general population is reported to be approximately 43.4±2.9 HU) [7]. These findings were consistent with 'chronic sialodochitis'. However, we could not rule out the possibility of 'obstructive sialoadenitis' because of the swelling of the submandibular glands. As the usual cause of the duct obstruction is a calculus or tumor, we performed a MRI examination . No tumors were detected on MRI. Instead, MRI showed the retention of saliva and the normal signal intensity of the glandular parts in both submandibular glands. We therefore diagnosed the patient with 'chronic sialodochitis' rather than "obstructive sialoadenitis". After the cytological examination of the fibrinous material showed the presence of numerous eosinophils, our final diagnosis was "chronic sialodochitis", specifically, "fibrinous sialodochitis". Okuda et al. [8] reported that the abnormal histopathological findings of the submandibular gland involved the duct rather than the glandular tissue. Ishii et al. [1] reported that the sialographic and histopathological findings only revealed ductal abnormalities. It is therefore reasonable to assume that this disease only affected the duct and not the glandular tissue. These reports were consistent with the present CT and MRI findings, which showed that the CT values and the signal intensity of the glandular parts of the submandibular glands on MRI were normal. Uno et al. [9] reported that the histopathological examination of the glandular ducts revealed numerous eosinophils in the larger glandular ducts, and concluded that an allergic reaction had occurred at the location. In this case, the retention of saliva was observed in the same region, which was also thought to be the site of an allergic reaction.
CONCLUSION
The present study represents the first case report that shows both the CT and MRI findings in a patient with fibrinous sialodochitis of submandibular glands. The swelling of the submandibular glands, dilatation of the glandular ducts, retention of saliva, and normal glandular tissue were observed. These CT and MRI findings were very important for distinguishing fibrinous sialodochitis from submandibular sialoadenitis.
REFERENCES
- Ishii M, Watanabe M, Ishii Y and Enomoto S. (1996). Sialodochitis fibrinosa: report of two cases. Asian J Oral Maxillofac Surg. 8, 111-114.
- Shimada T, Okano H and Hisa Y. (2006). A case of severe dilatation of the parotid duct due to fibrinous sialodochitis. Acta Otolaryngol. 126(10), 1112-1114.
- Chikamatsu K, Shino M, Fukuda Y, Sakakura K, et al. (2006). Recurring bilateral parotid gland swelling: two cases of sialodochitis fibrinosa. J Larygol Otol. 120(4), 330-333.
- Yamamoto T, Kimura I and Goto K. (2014). Hydrocortisone irrigation in the management of sialodochitis fibrinosa. J Jpn Soc Dent Medically Compromised Patient. 23(2), 80-83.
- Ray A, Burgin SJ and Spector ME. (2015). A rare case of Kussmaul disease (Sialodochitis fibrinosa). J Case Rep Med. 4(1+3).
- Hayashi K, Onda T, Ohata H, Takano N, (2016). Case of Suspected Sialodochitis Fibrinosa (Kussmaul's Disease). Bull Tokyo Dent Coll. 57(2), 91-96.
- Heo MS, Lee SC, Lee SS, Choi HM, et al. (2001). Quantitative analysis of normal major salivary glands using computed tomography. Oral Sug Oral Med Oral Pathol Oral Radiol Endod. 92(2), 240-244.
- Okuda M, Ogami Y and Umino T. (1975). Sialodochitis fibrinosa (Kussmaul). Otologia Fukuoka in Japanese. 21, 635-639.
- Uno M, Sakitani E, Nonaka M and Yoshihara T. (2014). Pathological study of sialodochitis fibrinosa. J Jpn Immunol Allergol Otolaryngol. 32, 145-46.