Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2022
Spontaneous Thrombosis of a Vein of Galen Malformation in the Adults: Case Report and a Review of the Literature
K Al Taha1*, N Tahhan2*#, C Dumot2, R Riva3, I Pelissou- Guyotat2
1 Department of Neurosurgery, Centre Hospitalier du Valais Romand, Sion, Switzerland
2Department of Vascular and Tumoral Neurosurgery, Hôpital Pierre Wertheimer, Hospices Civils de Lyon and Claude Bernard University of Lyon 1, Lyon, France
3Department of Interventional Radiology, Hôpital Pierre Wertheimer, Hospices Civils de Lyon and Claude Bernard University of Lyon 1, Lyon, France
Received Date: Jul 12, 2022
Published Date: Aug 05, 2022
*Co-authors: Dr Al Taha and Dr Tahhan
#Corresponding Author: Nadim Tahhan, Department of Vascular and Tumoral Neurosurgery, Hôpital Pierre Wertheimer, Hospices Civils de Lyon, Lyon, France. Tel: +33 675411335. Email: [email protected]
Citation: Tahhan N, et al. (2022). Spontaneous Thrombosis of a Vein of Galen Malformation in the adults: Case-Report and a review of the literature. Mathews J Case Rep. 7(2):74.
Copyrights: Tahhan N, et al. © (2022).
ABSTRACT
The vein of Galen malformations (VGAMs) are usually found in childhood and rarely described in adult. There are two major types of presentation: hemodynamic failure in neonates due to massive shunt, and venous hypertension during infancy. VGAMs are treated by endovascular methods in the majority of cases. We present a rare case of a 40 years old patient with incidental finding of VGAM who presented a spontaneous thrombosis and a complete restoration of the deep venous system followed by a review of the literature of resembling cases.
Keywords: Vein of Galen malformation; deep venous system; spontaneous thrombosis; case report
ABBREVIATIONS
VGAD: Vein of Galen Aneurysmal Dilatation
DSA: Digitally Subtracted Angiography
VGAM: Vein of Galen malformation
MRI: Magnetic Resonance Imaging
TOF: Time of Flight Angiography
CT scan: Computed Tomography scan
INTRODUCTION
The vein of Galen malformation is a rare vascular intracranial abnormality most often seen in neonates and childhood and is caused by an arterio-venous fistula of the median prosencephalic vein [1]. They can be divided into two types: mural and choroidal. They can manifest as cardiac congestive heart failure at the neonatal period, renal failure, cerebral ischemia and hydrocephaly. These entities should be differentiated from The Vein of Galen Aneurysmal Dilatation (VGAD) which results from an outflow obstruction [2].
CASE PRESENTATION
A 40-year-old female patient known for microprolactinoma, in a good health otherwise, was referred to our department after a cerebral MRI showed a mural vein of Galen malformation (Figure 1-a and 1-b).
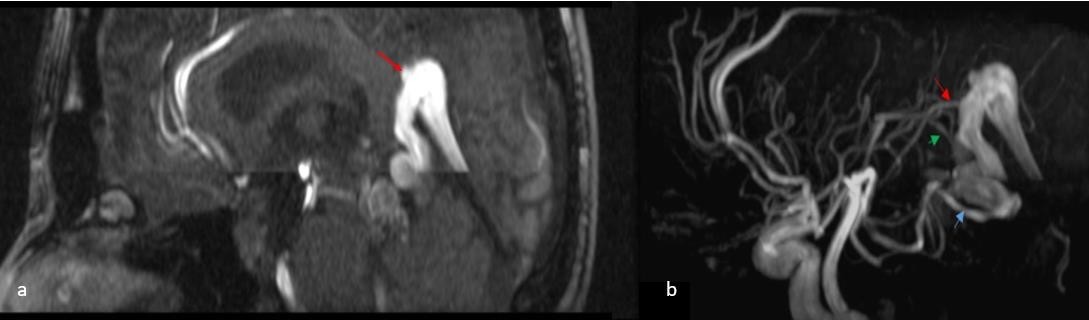
Figure 1- (a) Cerebral MRI T1W with gadolinium contrast showing the vein of Galen malformation (red arrow) with no sign of cerebral hemorrhage (b) Cerebral MRI TOF showing the arteriovenous malformation with 3 feeders from the posterior cerebral artery (red arrow), the posterior choroidal artery (green arrow) and the superior cerebellar artery (blue arrow).
The patient had a normal neurologic examination. A Digitally Subtracted Angiography (DSA) was proposed to the patient who refused it due to fear of the procedure’s complications. The patient was lost from follow-up. 8 years later she was referred again to our department with the complaint of new isolated retro-orbital headaches for the last 2 months, with a normal neurologic examination. The cerebral MRI showed a partial thrombosis of the vein of Galen malformation (Figure 2).
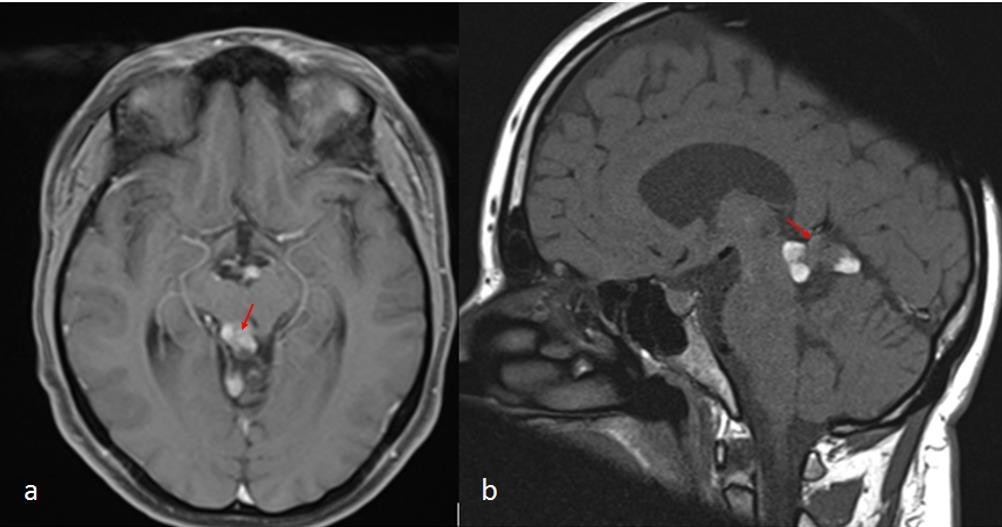
Figure 2. Cerebral MRI T1W (a) with gadolinium contrast and (b) without contrast after 2 months of retro-orbital headaches showing the partial thrombosis of the vein of Galen arteriovenous malformation (red arrows) with no sign of cerebral hemorrhage or hydrocephalus.
10 months later the patient, still asymptomatic, accepted to undergo a DSA. The DSA showed a complete resolution of the vein of Galen malformation with the absence of any signs of cerebral hemorrhage (Figure 3-a and 3-b). The follow-up cerebral MRI 6 months later confirmed the complete resolution of the vein of Galen malformation and a complete restoration of the arterial and venous cerebral circulation in this patient who remained intact on the neurologic examination (Figure 3-c and 3-d).
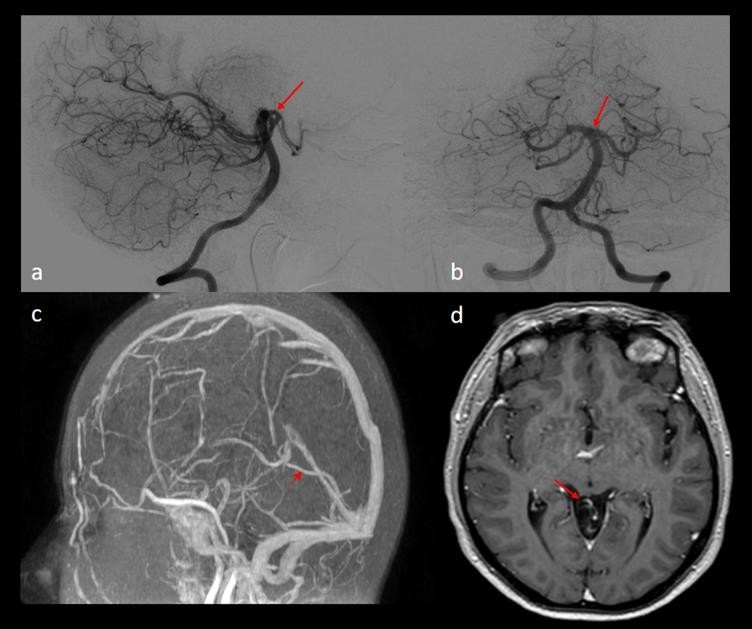
Figure 3- (a) Cerebral DSA lateral view showing normal vascular anatomy (red arrow) with complete thrombosis of the arteriovenous malformation. (b) Cerebral DSA anterior-posterior view showing a completely normal vascular anatomy (red arrow) and complete thrombosis of the arteriovenous malformation. (c) Cerebral MRI - TOF at 6 months follow-up post DSA showing no signs of arteriovenous malformation with normal vascular anatomy (red arrow showing a normal vein of Galen). (d) Cerebral MRI – T1W with gadolinium contrast showing the complete thrombosis of the vein of Galen malformation with normal vascular anatomy (red arrow).
DISCUSSION
VGAMs are rare pathologies usually seen in childhood and rarely in adults. They consist of multiple arteriovenous shunts draining into a dilated median prosencephalic vein of Markowski [2]. We can differentiate two types of VGAM in childhood: the choroidal type which is supplied by the choroidal and thalamic arteries and normally is not well tolerated, and the mural type which is fed by posterior collicular and choroidal arteries forming an arteriovenous fistula directly within the wall of the persistent median prosencephalic vein and is normally better tolerated [10]. Even though there are no clear predisposing factors for this pathology, some papers suggest a genetic contribution to the development of malformation [7]. This pathology was accompanied with 70% or more mortality and morbidity if untreated until the introduction of the endovascular treatment by embolization which has been found to be highly effective in the young population [9].
Stenosis can occur as a result of the response of the venous endothelium to the rapid and turbulent flow of the shunt [1]. However, our patient didn’t show any sign of dural sinus stenosis, although no DSA was performed to rule out this possibility.
VGAM is a rare pathology in the adult population. While their presentation may vary from asymptomatic to life-threatening, the reason for this variation is still unclear due to the rarity of this pathology in adults [15]. Spontaneous thrombosis of a VGAM is a rare event in the adult and pediatric population. Kerolus et al. [3] described a case of a giant VGAM in a 42 years old patient known for seizures, developmental delay, and ventriculoperitoneal shunts, which was treated only by observation due to the poor clinical status of the patient. An intracranial hemorrhage as an onset presentation of VGAM in adult patients has been also described by Tsai et al. [11]. Wang et al. [13] reported a case of a 59 years old patient who presented with sudden headache, nausea, and vomiting but without any neurologic deficit. The CT scan showed hydrocephalus accompanied by intraventricular hemorrhage and subarachnoid hemorrhage with a large VGAM. The patient was also treated conservatively.
Pareek et al. [6] reported the case of a young adult patient with a VGAM who presented orthostatic headache without any other symptom: The patient was treated by embolization with a very good outcome. Tsimpas et al. [12] described a case of a 37 year-old patient with congestive heart failure since birth due to an untreated VGAM, who presented a nonspecific headache. The patient was treated by embolization with a very good outcome and an intact neurologic status at the 6 months follow-up.
On the other hand, there have been some cases in the literature where a spontaneous thrombosis of the VGAM has been documented. Salwani et al. [8] reported a case of a VGAM in a 44 years old patient which was diagnosed after partial seizures. The patient presented a spontaneous thrombosis of the VGAM without intracranial hemorrhage. A complete seizure resolution was reported in the patient. Konus et al. [5] described a case of spontaneous thrombosis of VGAM after a diagnostic DSA. The patient didn’t show any changes in his neurologic state after the thrombosis.
Although this phenomenon has been described, the physiology by which it happens remains unclear and multiples hypothesis has been proposed. Konus et al. [5] hypothesized in their paper that contrast media might play role in the spontaneous thrombosis of VGAM. In our case, the patient didn’t have a diagnostic DSA so we can rule out the role of contrast media in our patient. Konovalov et al. [4] believe that thrombosis occurs due to low blood flow and insufficient venous drainage. Brunelle et al. [1] found that increased pressure and venous flow turbulence lead to progressive myointimal proliferation with hypertrophy of the vein of Galen wall, resulting in gradual venous thrombosis. Salwani et al. [8] proposed that the gradual occurrence of the venous thrombosis is the reason of lacking hemorrhage event in these patients.
The complete normalization of venous drainage after occlusion of the malformation which has been shown in our patient, has also been described by Winkler et al. [14] and thought to be caused by a slow adaption and reconstruction of the vascular architecture and hemodynamic system due to the gradual obstruction of the malformation by embolization or spontaneously as in our case.
CONCLUSION
A vein of Galen arteriovenous malformation is rare in the adult population and may have various clinical presentations. Although endovascular treatment has been proposed for this pathology with good results in childhood, there is still no clear method of treatment in adult patients and there have been some cases of VGAM spontaneous thrombosis with good clinical outcomes and normal restoration of the deep venous system through unknown physiology.
AUTHORS’ CONTRIBUTION
All authors contributed to the study conception and design. Material preparation, data collection were performed by NT. The first draft of the manuscript was written by NT and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
REFERENCES
- Brunelle F. (1997). Arteriovenous Malformation of the Vein of Galen in Children. Pediatr Radiol. 27(6):501-513.
- Stanley H, Choudhri O, Edwards M, Guzman R. (2009). Vein of Galen Malformation. Neurosurg Focus. 27(5):e8.
- Kerolus MG, Tan LA, DK Lopes. (2017). Giant Vein of Galen Malformation in an Adult. Radiol Case Rep. 12(3):585-589.
- Konovalov AN, DI Pitskhelauri, Arutiounov NV. (2002). Surgical Treatment of the Thrombosed Vein of Galen Aneurysm. Acta Neurochir (Wien). 144(9):909-915.
- Konus ÖL, Ilgıt ET, Özdemir A, Önal B. (2000). Spontaneous Thrombosis of a Vein of Galen Aneurysmal Malformation: Possible Effects of Contrast Media. Eur Radiol. 10(9):1456-1458.
- Pareek K, Trilochan S, VD Sinha. (2018). Choroidal Type of Vein of Galen Aneurysmal Malformation in Adult Patient with Unusual Presentation of Orthostatic Headache. Asian J Neurosurg. 13(2):418-420.
- Revencu N, Boon LM, Mulliken JB, Enjolras O, Cordisco MR, et al. (2008). Parkes Weber Syndrome, Vein of Galen Aneurysmal Malformation, and Other Fast-Flow Vascular Anomalies Are Caused By RASA1 Mutations. Hum Mutat. 29(7):959-965.
- Sawlani V, Handique A, Phadke RV. (2004). Spontaneous Regression of Cerebral AVM Due to Thrombosis of Draining Vein—Angiographic and MRI Demonstration. J Neurol Sci. 223(2):195-198.
- Sivasankar R, Limaye US, Wuppalapati S, Shrivastava M. (2019). Endovascular Management of Vein of Galen Aneurysmal Malformations: A Retrospective Analysis over a 15-Year Period. J Vasc Interv Neurol. 10(3):23–29.
- Spazzapan P, Zoran M, Velnar T. Vein of Galen Aneurismal Malformations - Clinical Characteristics, Treatment, and Presentation: Three Cases Report. World J Clin Cases. 7(7):855‑862.
- Tsai YS, YR Chen, LW Chen. (2015). Mystery Case: Intracranial Hemorrhage in Adult Vein of Galen Malformation. Neurol. 85(13): e94–e95.
- Asterios T, Chalouhi N, Halevy JD, Tjoumakaris S, Gonzalez LF, et al. (2014). The Use of Adenosine in the Treatment of a High-Flow Vein of Galen Malformation in an Adult J Clin Neurosci. 21(7):1259-1261.
- Wang CS, Yeh TC, Chao CM. (2016). Vein of Galen Malformation. The Journal of Emergency Medicine. 51(3):e51-e52.
- Winkler O, Brinjikji W, Lanfermann H, Brassel F, Meila D. (2019). Anatomy of the Deep Venous System in Vein of Galen Malformation and Its Changes after Endovascular Treatment Depicted by Magnetic Resonance Venography. J Neurointerv Surg. 11(1):84-89.
- Xu DS, Usman AA, Hurley MC, Eddleman CS, Bendok BR. (2010). Adult Presentation of a Familial-Associated Vein of Galen Aneurysmal Malformation: Case Report. Neurosurg. 67(6):e1845-1851