Previous Issues Volume 1, Issue 1 - 2016
Sonographic Features of Hypertrophic Pyloric Stenosis
Hidayatullah Hamidi1
1Radiology department, French Medical Institute for Children (FMIC), Kabul, Afghanistan.
Corresponding Author: Hidayatullah Hamidi, Radiology department, French Medical Institute for Children (FMIC), Kabul, Afghanistan, Tel: 0093744733605; E-Mail: [email protected]
Received Date: 18 Feb 2016 Accepted Date: 31 Mar 2016 Published Date: 13 Apr 2016
Copyright © 2016 Hamidi H
Citation: Hamidi H. (2016). I Sonographic Features of Hypertrophic Pyloric Stenosis. Mathews J Case Rep 1(1): 003.
KEYWORDS
Hypertrophic Pyloric Stenosis; Gastric Outlet Obstruction; Non-Bilious Vomiting.
CASE PRESENTATION
A three month old boy that weighs 4 Kg has persistent vomiting for last two months. Trans-abdominal sonography with high frequency linear probe shows the abnormally thick walled, peripherally hypo-echoic and centrally hyper-echoic tubular structure just inferior to the gall bladder which is proximally continued to the dilated stomach. The length of this abnormal segment is 24 mm with a wall thickness of 8 mm.

Figure 1: Trans-abdominal ultrasound with high frequency linear probe: Abnormally thick walled, peripherally hypo-echoic and centrally hyperechoic tubular structure just inferior to the gall bladder (GB) proximally continued to the dilated stomach.
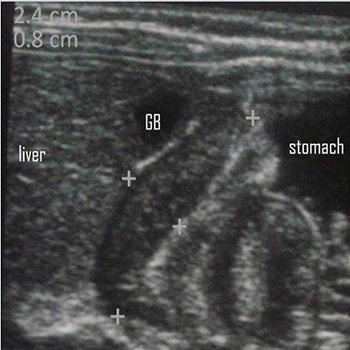
Figure 2: Length of this abnormal segment is 24 mm and wall thickness is 8 mm.
DISCUSSION
Hypertrophic pyloric stenosis (HPS) is the thickening of the muscular layer of antropyloric canal with resultant failure to relax and subsequent gastric outlet obstruction. Elongation of the canal and thickened mucosa are also seen [1]. The incidence is 3 per 1000 live births per year; however variations are present with geographic location, season and ethnic origin [1, 2]. Typically infants are clinically normal at birth but during the first few weeks of life, they develop non-bilious projectile vomiting [3]. Diagnosis is suggested by typical clinical presentation [3]. Palpation of the hard muscle mass or olive is diagnostic with detection rate of 85%-100% in experienced hands and with adequate time and preparation but it is often challenging and time consuming [3, 4]. Accurate clinical diagnosis in patients in whom a thickened antropyloric muscle is not readily palpable can be difficult, resulting in delayed diagnosis [3]. Ultrasound (US) is the preferred diagnostic modality especially when performed with high frequency linear probe by experienced hands [5]. It is a non-invasive and radiation free technique. The typical sonographic feature is increased thickness of the muscular layer. An abnormal cut off value of 3 mm in thickness has been described in the literature [6]. The other criterion is the llength of the pyloric canal greater than 12 mm in length [7]. In conclusion; infants with persistent, non-bilious vomiting that are clinically suspected for infantile hypertrophic pyloric stenosis can be evaluated by trans-abdominal (multi frequency linear transducer) sonography as a noninvasive, radiation free imaging modality. When thickened pyloric muscular layer of 3 mm or more in thickness and greater than 12 mm in length is noted, the diagnosis of hypertrophic pyloric stenosis can be made with great accuracy.
REFERENCES
- SC Dias, S Swinson, H Torrão, Gonçalves L, et al. (2012). Hypertrophic pyloric stenosis: tips and tricks for ultrasound diagnosis. Insights Imaging. 3(3), 247-250.
- Panteli C. (2009). New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 25(12), 1043-1052.
- Hernanz-Schulman M. (2003). Infantile Hypertrophic Pyloric Stenosis. Radiology. 227(2), 319-331.
- Irish M, Pearl R, Caty M and Glick P. (1998) Pediatric surgery for the primary care pediatrician. I. The approach to common abdominal diagnoses in infants and children. Pediatr Clin North Am. 45, 729-772.
- Hiorns MP. (2011). gastrointestinal tract imaging in children: current techniques. Pediatr Radiol. 41(1), 42-54.
- O’Keeffe FN, Stansberry SD, Swischuk LE and Hayden CK. (1991). Antropiloric muscle thickness at US in infants: what is normal. Radiology. 178(3), 827-830.
- Reed AA and Michael K. (2010). Hypertrophic pyloric stenosis. J Diagn Med Sonography. 26, 157-160.