Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2020
Sister Mary Joseph’s Nodule in a Patient with Adenocarcinoma of Lung
Dushantha Madegedara*, Lihini Basnayake, Sajani Dharmadasa, Sachini Seneviratne, Luckmy S. A, Ishelda Nawarathne, Prasanna Wijerathne, Jayani Jayawardhana
*Corresponding author: Dushantha Madegedara, Respiratory unit, National Hospital, Kandy, Sri Lanka, E-mail: [email protected]; Tel: +94-777-840-114.
Received Date: August 02, 2020 Publication Date: August 26, 2020 Copyright: Madegedara D, et al. ©2020. Citation: Madegedara D. (2020). Sister Mary Joseph’s Nodule in a Patient with Adenocarcinoma of Lung. Mathews J Case Rep. (5)1: 62.
ABSTRACT Sister Mary Joseph’s nodule (SMJN) is a metastatic umbilical deposit secondary to any primary visceral malignancy. It is a relatively rare phenomenon which signifies poor prognosis and shorter survival time as it is usually associated with advanced malignancy. The most common origins of SMJN are gastrointestinal and gynaecological malignancies. We present a case of a 69-year-old male who presented with progressive breathlessness, cachexia and a coexisting umbilical lesion suggestive of SMJN. He was found to have a right side malignant pleural effusion with multiple pleural deposits and the histopathological studies of both pleural and umbilical deposits confirmed metastatic deposits from an adenocarcinoma of primary pulmonary origin, which is a rare occurrence with only a few cases reported so far. KEYWORDS: Sister Mary Joseph’s nodule; Adenocarcinoma; Lung; Histopathology; Case INTRODUCTION Cutaneous metastases at the umbilicus manifesting as a palpable nodule is referred to as Sister Mary Joseph nodule. This sign was first identified by Sister Mary Joseph in 1928 and the term SMJN was used by Sir Hamilton Bailey in his textbook ‘Demonstration of Physical Signs in Clinical Surgery” in 1949 [1]. It is a relatively rare clinical finding in modern medical practice, however when present it signifies advanced malignancy, hence limited treatment options. More than half of SMJN occurs secondary to gastrointestinal malignancies [2] (gastric, colonic, pancreatic) while the rest is accounted for by gynaecological malignancies mainly (ovarian, endometrial) and unknown primary tumors [3,4]. Primary lung malignancy has rarely been associated with SMJN with only a few reported cases so far [5]. Previous case analysis of patients with SMJN conducted by Charoenkul V, et al. [6] and Chalya PL, et al. [7] using 262 and 34 patients respectively did not reveal lung malignancy as the primary site. Hence here we report a patient who presented with umbilical deposits and was subsequently diagnosed to have disseminated lung malignancy. CASE REPORT A 69-year-old previously healthy male presented to the respiratory unit in National Hospital, Kandy with a five month history of progressive breathlessness and non-productive cough. There was associated pleuritic type of chest pain on the right side, which gradually worsened in severity over the last three months. He denied having any wheezing, hemoptysis, orthopnoea, paroxysmal nocturnal dyspneaor pedal swelling. He also complained of significant constitutional symptoms in the preceding four months with severe anorexia and a weight loss of 10 kilograms. There was no fever, night sweats, or contact history of tuberculosis. The systemic review did not reveal any other symptoms. He was a retired prison officer and had a 25-pack year history of smoking without any other significant organic or inorganic substance exposures. On examination, the patient was emaciated, moderately pale, and anicteric. There was a right axillary lympahadenopathy which was firm and non-tender. He did not have finger clubbing or ankle swelling. Respiratory system examination revealed a right-sided moderate pleural effusion with central positioned trachea. On inspection of the abdomen, there was a hard periumbilical bluish violet swelling measuring about 2 cm in width, resembling SMJN (Figure 1). The rest of the abdominal, cardiovascular, and neurological examinations were unremarkable. The initial investigations revealed the following: Hemoglobin 11.4g/dL (11.0-16.0), WBC 5.44 x 109/L (4.0-10.0), platelet 280 x 109/L (150-450), ESR 45mm/1st hour, CRP 13 mg/L(<10). Renal and liver function tests, urinalysis, serum sodium, potassium, total, and ionized calcium and phosphate were normal. Chest radiography revealed a right-sided moderate pleural effusion (Figure 2). The sputum for acid-fast bacilli was negative. The pleural fluid analysis revealed blood-stained pleural fluid with WBC- 58/Cumm (polymorphs 95%, lymphocytes 5%) and RBC 20000/Cumm. Pleural fluid culture revealed no growth.
Figure 1: Hard periumbilical bluish violet swelling

Figure 2: Chest radiography of right-sided moderate pleural effusion.

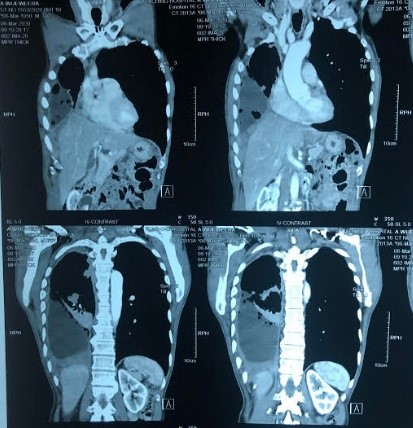
Contrast-enhanced computed tomography (CECT) chest (Figure 3) revealed a large pleural effusion on the right side with hydropneumothorax and right lower lobe collapse. Diffuse nodular pleural thickening was noted involving the mediastinal (maximum diameter measuring 3.2cm), costal and diaphragmatic pleura in right hemithorax. An enlarged right axillary lymph node (12mm) was identified. An enhancing focal lesion of the liver was seen in segment VIII (1cm x 1.2cm).
Figure 3: CECT Chest showing right side large plural effusion with diffuse nodular thickening of the pleura.
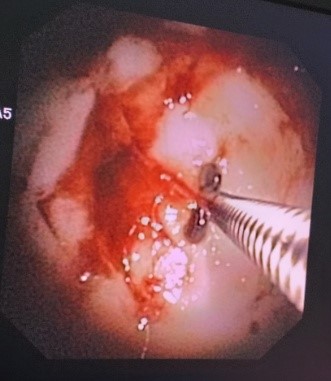
The patient underwent fiberoptic thoracoscopy which revealed numerous white plaque like lesions located on the costal and diaphragmatic pleura (Figure 4). Pleural biopsy revealed metastatic deposits from a G2 adenocarcinoma which stained positively for CK7 and TTF- 1 and negative for CK20 confirming the primary site of malignancy as pulmonary. The biopsy of the periumbilical lesion also demonstrated metastatic deposits from a moderately differentiated adenocarcinoma. The immunohistochemical examination confirmed primary pulmonary origin. Detailed clinical examination and investigations including CECT abdomen, upper and lower gastrointestinal endoscopies and serum tumor markers (CEA, CA 19-9 and PSA) did not reveal any other coexisting malignancy. Therefore the patient was diagnosed to have adenocarcinoma of the lung associated with SMJN and subsequently referred for oncological management.
Figure 4: Thoracoscopic appearance of costal pleura showing whitish plaque like lesions.
DISCUSSION Cutaneous metastasis of lung cancer is a recognized manifestation and frequently occurs in supradiaphragmatic regions (mostly chest). Spread of metastasis to the umbilical region is assumed to occur via several modes such as contiguous spread along the peritoneum, hematogenous, or lymphatic spread with contiguous extension along with embryonic ligaments [3,5]. Malignant extension from the right pleura to the peritoneum was thought to give rise to umbilical deposits in this patient. Irrespective of the primary, the presence of SMJN indicates poor prognosis with a mean survival of approximately 10-12 months [8]. Most of the time, patients with established SMJN receive only palliative care, especially when the primary tumor is non-resectable as in our case. However recent studies have demonstrated better survival in selected patients when combination treatment such as wide surgical excision, chemotherapy, and radiotherapy was used [9]. Also, some data has shown that the survival is better in patients whose umbilical metastasis was detected before the definitive treatment of primary tumor, compared to those whose umbilical lesion appeared following the treatment of the primary tumor [10]. This case emphasizes the importance of thorough physical examination; as detection of SMJN not only suggests an underlying malignant process but also influences management decisions. Radiological assessment with CT and/or MRI is important to determine the primary site and the extent of the underlying malignancy. Further on, histopathological examination of all suspicious umbilical lesions is invaluable to diagnose SMJN as well as to exclude rare benign primary neoplasms of the umbilicus. Other major differential diagnosis of an umbilical nodule includes umbilical hernia, umbilical endometriosis, omphalith, keloid, pyoderma gangrenosum, and foreign body [11]. Distinguishing between these differential diagnosis should be carefully done in order to provide patients with the optimum management. CONCLUSION SMJN still remains an interesting and important physical sign. Along with the more common sites of origin, primary pulmonary malignancies should also be considered and actively excluded when a case of SMJN is encountered. CONSENT Informed written consent was obtained from the patient for publication of this case and accompanying images. FOOT NOTES CONFLICT OF INTERESTS Authors have no conflict of interests. REFERENCES 1. Falchi M, Cecchini G, Derchi LE. (1999). Umbilical metastasis as first sign of cecal carcinoma in a cirrhotic patient (Sister Mary Joseph nodule). Report of a case. Radiol Med. 98:946. 2. Fratellone PM, Holowecki MA. (2009). Forgotten node: a case report. World J Gastroenterol. 15:4974-4975. 3. Dar IH, Kamili MA, Dar SH, Kuchaai FA. (2009). Sister Mary Joseph nodule-A case report with review of literature. J Res Med Sci. 14(6):385-387. 4. Deb P, Rai RS, Rai R, Gupta E, Chander Y. (2009). Sister Mary Joseph nodule as the presenting sign of disseminated prostate carcinoma. J Cancer Res Ther. 5:127-9. 5. Wang F, Chen H, Zhang X. (2011). Sister Mary Joseph's nodule derived from lung cancer. Indian J Dermatol Venereol Leprol. 77:609–11. 6. Charoenkul V, Del-Campo A, Derby A, Hodgson WJ, Mc Elhinney AJ. (1977). Tumors of the umbilicus. Mt Sinai J Med. 44:257-62. 7. Chalya PL, Mabula JB, Rambau PF, McHembe MD. (2013). Sister Mary Joseph’s nodule at a University teaching hospital in northwestern Tanzania: a retrospective review of 34 cases. World J Surg Oncol. 11(1):151. 8. Panaro F, Andorno E, Di Domenico S, Morelli N, Bottino G, et al. (2005). Sister Joseph's nodule in a liver transplant recipient: Case report and mini-review of literature. World J Surg Oncol. 3(1):4. 9. Gabriele R, Conte M, Egidi F, Borghese M. (2005). Umbilical metastasis: current viewpoint. World J Surg Oncol. 3(1):13. 10. Chen P, Middlebrook MR, Goldman SM, Sandler CM. (1998). Sister Mary Joseph nodule from metastatic renal cell carcinoma. J Comput Assist Tomogr. 22:756–757. 11. Tso S, Brockley J, Recica H, Ilchyshyn A. (2013). Sister Mary Joseph's nodule: an unusual but important physical finding characteristic of widespread internal malignancy. Br J Gen Pract. 63(615):551-552.