Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2021
Secondary Nasolacrimalduct Obstruction Causing Persisting Epiphora
Kasim Aljanabi
ENT specialist, Sohar hospital, Oman
Corresponding Author: Kasim Aljanabi, ENT specialist, Sohar hospital, Oman, Tel: 96-896-671-203; E-mail: [email protected]
Received Date: November 11, 2020
Publication Date: January 25, 2021
Copyright: Aljanabi K. © 2021.
Citation: Aljanabi K. (2021). Secondary nasolacrimalduct obstruction causing persisting epiphora. Mathews J Case Rep. (6)1:66.
ABSTRACT
Epiphora secondary to nasolacrimal duct obstruction (NLDO) is a common condition and may affect quality of life usually it usually requires surgical intervention. NLDO may be multifactorial. Co-occurrence of endoscopic sinu-nasal anomalies can contribute and may be additional causes to NLDO as will be demonstrated in our case.
KEYWORDS: Epiphora; Nasolacrimal duct obstruction; Sinu-nasal anomalies
INTRODUCTION
Nasolacrimal duct obstruction is a common cause of epiphora. The most common cause of primary NLDO is chronic inflammation and fibrosis [1]. Secondary causes of NLDO are less common and diagnosis may require a more extensive workup. Correct diagnosis of the obstruction site and its nature is essential for choosing a treatment plan and surgical approach [2]. Recent reports suggest that obstructions of Hasner’s valve (inferior meatus, IM) are significantly more common in adults than previously appreciated [3,4]. In this paper, we will describe a nasal septal pathology that contributes to NLDO.
CASE HISTORY
We present a 40 year old gentleman with no background of medical illnesses. He was referred to our ENT clinic for left eye excessive tearing for two years duration. He was diagnosed by ophthalmology as distal nasolacrimal duct (NLD) obstruction and referred to us for endoscopic dacrocystorhinostomy (DCR). His complaint started a year after road traffic accident. He sustained mild facial injuries with epistaxis after hitting the steering wheel. He was discharged well after a thorough ENT, maxillofacial and neurosurgery consult. After one year he started to have excessive left sided epiphora associated with left sided nasal blockage sensation and occasional left sided blood stained nasal discharge. There were no symptoms of sinusitis, facial fullness, facial numbness, proptosis and neck swellings. He consulted ophthalmology for epiphora and their exam findings suggested distal NLD obstruction and referred to ENT for possible endoscopic DCR. Upon examination, his general exam was unremarkable. Local nasal exam noted to have significant reduce in misting during cold spatula test on the left side with positive Cottles sign on the left side. Nasal endoscopic exam as shown in (Figure 1) revealed severely deviated anterior nasal septum with caudal dislocation and sever spur impinging upon the inferior turbinate pushing it laterally. The nasopharynx exam was unremarkable. Neck and otology exam were unremarkable. Paranasal sinus (PNS) CT scan was ordered as shown in (Figure 2) which showed severely deviated anterior nasal septum with sever inferior spur pushing the inferior turbinate laterally causing the possibility of secondary mechanical NLD obstruction, paranasal sinuses and nasopharynx were clear. Septoplasty with intra operative NLD syringing and possibility of endoscopic DCR if obstruction persist after septal correction was suggested. Intra-operatively; Post septoplasty alone, NLD syringing noted to be patent and normal flow was observed from the NLD opening at the inferior meatus as shown in figure 3. His post-operative follow up was unremarkable and symptoms free.
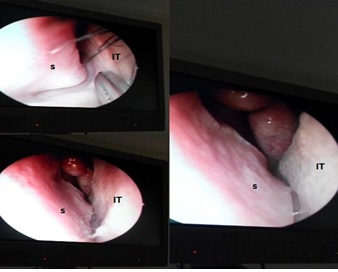
Figure 1: Endoscopic view of the left nasal cavity showing sever septal spur (S) impinging the inferior turbinate (IT).
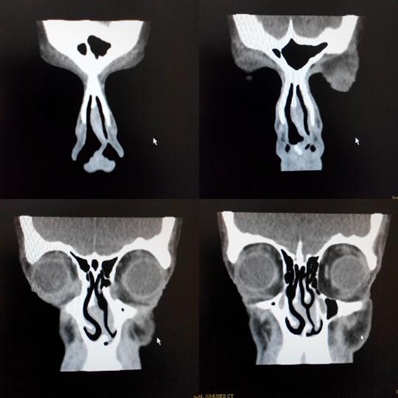
Figure 2: coronal CT scan showing sever deviated nasal septum with sever septal spur pushing the inferior turbinate laterally causing the possible NLD obstruction.

Figure 3: Intra operative nasal scope at the level of inferior meatus after medializing the inferior turbinate post septoplasty during eye syringing showing the free flow of saline (black star) through the NLD opening.
DISCUSSION
Epiphora is defined as excessive tearing and can be caused by anatomical lid problems like entropion, ectropion, lip malposition, and blepharitis but the most common cause of epiphora is the NLD obstruction which can occur anywhere along its course. The causes of NLD obstruction can be anatomic 70% and functional 30% [5]. The anatomic obstructions most commonly noted between the lacrimal sac and nasal cavity while functional obstructions are caused by either narrowing within the lacrimal system or a failure of the proximal pumping mechanism. To evaluate epiphora patients presenting for DCR, other causes of epiphora need to be excluded. Apurulent material coming from the lacrimal punctamwhile medial canthal palpation indicates obstruction of the nasolacrimal system, which warrants DCR.The lacrimal probing with a Bowman's lacrimal probe gives a detailed clinical picture to the level of blockage. A “hard stop” indicates that the probe has stopped against the lacrimal bone, suggesting a patent lacrimal system up to the lacrimal sac while “soft stop” indicates that the probe is stopped by soft tissue, suggesting either stenosis of the common canaliculus or a tight common canaliculus-sac junction. Syringing of the lacrimal apparatus will give further information. Radiologic evaluation of lacrimal obstructions begins with the dacryocystogram (DCG) and lacrimal scintilligraphy [6]. Unfortunately both tests were not available at our institute. Dacrocystorhinostomy (DCR) is a surgical procedure to bypasses the most distal portion of the lacrimal apparatus, creating a new outflow in the lateral wall of the nasal cavity instead of the inferior meatus opening. Thus, DCR is intended to manage obstructions of the lacrimal sac and duct. Endoscopic dacryocystorhinostomy (DCR) was first described in the otolaryngology literature by McDonogh [7] in 1989. Over the subsequent years, there has been a steady improvement in outcomes owing to advances in surgical technique, instrumentation, and comprehension of the anatomy. The surgical outcomes improved significantlyspecially, once the lacrimal sac was recognized to extend superiorly above the middle turbinate [8]. Today's endoscopic DCR is a reliable and effective technique that is equivalent and economically superior to external DCR in outcome measures [9,10]. Previously published series suggest that nasal mucosa hypertrophy and nasal septal deviation are common causes for NLDO [11,12] and they have found that it often co-exists with other pathologies of the inferior meatus. Failure to address both pathologies may leave the patient symptomatic as was suggested by Chan et al. [13]. We recommend that thorough nasal endoscopy must be done for every patient undergoing DCR to rule out such nasal pathologies that might contribute to secondary NLD obstruction. In conclusion inferior meatus obstruction is an underdiagnosed cause of epiphora. In selected cases of NLDO, diagnosis and treatment can be done endoscopically avoiding the need for dacryocystorhinostomy.
ACKNOWLEDGEMENTS
We thank ENT department in ibra hospital for their support. This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
REFERENCES
- Ohtomo K, Ueta T, Toyama T, Nagahara M. (2013). Predisposing factors for primary acquired nasolacrimal duct obstruction. Graefes Arch Clin Exp Ophthalmol. 251:1835–9.
- Golan S, Leibovitch I, Landsberg R. (2014). Unexpected pathologies in patients referred for endoscopic DCR. Eur Arch Oto-Rhino-Laryngol. 271:3053–8.
- Eloy P, Poirrier L, Nicoli T, Marlair C, Delahaut G, et al. (2012). Cystic dilation of the distal end of the nasolacrimal duct: underrated cause of epiphora in adults and its endoscopic treatment. Rhinology. 50:436–41.
- Pedram D, John M, Del Gaudio M. (2014). Inferior meatus surgery for distal nasolacrimal duct obstructions long-term outcomes and .treatment paradigm JAMA Otolaryngol Head Neck Surg. 140:736–41.
- Wormald PJ, Tsirbas A. (2004). Investigation and endoscopic treatment for functional and anatomical obstruction of the nasolacrimal duct system. Clin Otolaryngol Allied Sci. 29:352-356.
- Wormald PJ, Kew J, van Hasselt CA. (2000). Intranasal anatomy of the naso-lacrimal sac in endoscopic dacryocystorhinostomy. Otolaryngol Head Neck Surg. 123:307-310.
- Mc Donogh M. (1992). Endoscopic transnasaldacryocystorhinostomy: Results in 21 patients. S Afr J Surg. 30:107-110.
- Wormald PJ, Kew J, van Hasselt CA. (2000). Intranasal anatomy of the naso-lacrimal sac in endoscopic dacryocystorhinostomy. Otolaryngol Head Neck Surg. 123:307-310.
- Tsirbas A, Wormald PJ. (2004). Mechanical endonasaldacryocystorhinostomy versus external dacryocystorhinostomy. Ophthal Plast Reconstr Surg. 20:50-56.
- Anari S, Ainsworth G, Robson AK. (2007). Cost-efficiency of endoscopic and external dacryocystorhinostomy. J Laryngol Otol. 19:1-4.
- Rogers GA, Murchison AP, Wojno TH, DelGaudio JM. (2009). Inferior meatus endoscopy and directed treatment for epiphora: early experience with a novel approach. Otolaryngol Head Neck Surg. 140:579–84.
- Pedram D, John M, DelGaudio M. (2014). Inferior meatus surgery for distal nasolacrimal duct obstructions long-term outcomes and treatment paradigm. JAMA Otolaryngol Head & Neck Surg. 140:736–4.
- Chan DM, Golubev I, Shipchandler TZ, Nunery WR, Lee HH. (2014). Improving outcomes by combining septoplasty with primary external dacryocystorhinostomy. Am J Otolaryngol Head Neck Med Surg. 35:309-12.