Previous Issues Volume 4, Issue 2 - 2019
Propranolol: A Therapeutic Alternative in Benign Hemangiomas in a General Hospital. Clinical Cases
Francisco José Granados Navas, Guillermo Padrón Arredondo
Department of Pediatrics and Surgery, General Hospital of Playa del Carmen, Mexico.
Received Date: May 28, 2019 Published Date: Jun 24, 2019
Corresponding Author: Francisco José Granados Navas, Department of Pediatrics and Surgery, General Hospital of Playa del Carmen, Constituyentes Avenue S/N, Ejido CP 77710, Playa del Carmen, Solidarity, Q Roo, Mexico.
Copyright © 2019 Granados Navas FJ
Citation: Granados Navas FJ. (2019). Propranolol: A Therapeutic Alternative in Benign Hemangiomas in a General Hospital. Clinical Cases. Mathews J Case Rep 4(2): 49.
ABSTRACT:
Introduction: Infantile hemangiomas are the most frequent benign tumors in the pediatric age; they are produced by the proliferation of endothelial cells of blood vessels. They run with two phases; a period of proliferation (in the first 4 and 6 months of age, although it can last up to 18 months) and then one of involution (over the course of the years, which is complete in 50% of childhood hemangiomas at the age of five years-old and 70% at the age of seven years-old).
Clinical cases: Seven patients with a clinical diagnosis of benign hemangioma of childhood. The recommended treatment period was nine months. Two cases presented early improvement at the 5th month of treatment and the rest completed the proposed 9th month schedule, observing a clear improvement in the lesions. At the end of the treatment, one patient required cosmetic surgery of the lesion in the right hemithorax, a procedure that was carried out without complications. The other three cases corresponded to: male six month old back injury; female 1 year lesion in the neck and supraciliary region of the left eye; and 2-year-old female with neck injury 1 month of propranolol treatment 2 mg/kg/day.
Discussion: The use of propranolol has been a priority for the treatment of childhood hemangiomas, its discovery to induce the regression of a facial infantile hemangioma, was while treating a patient with obstructive cardiomyopathy who was administered propranolol, discovery by the group of Leauté-Lebréze in 2008.
Keywords: Infantile Hemangioma; Propranolol.
INTRODUCTION
Benign hemangiomas are the most frequent benign neoplasms of childhood, they are produced by the proliferation of endothelial tissue, may be very little at birth, are characterized by having a proliferative phase and another involutional phase, and may present a slow and spontaneous regression (without treatment) in up to 70% of patients at the age of seven years-old (the involutional phase does not mean complete disappearance); sequelae have been observed in 20% to 40% of patients (scars, hypopigmentation, telangiectasias), mostly affecting the head and neck and most of them manifest as unique lesions, if evolution can be unpredictable to reach very large dimensions, even cause major complications. Its treatment has been controversial because most of the time its course is benign, however it has been suggested that the treatment must be individualized, assessing the location, the size of the lesion, the presence of ulceration or the involvement of other organs [1-3].
Clinical Cases
We present seven patients, treated at the pediatric surgery service with a clinical diagnosis of benign hemangioma of childhood. The parents were interviewed about important medical history and a complete physical examination and injury was performed. The start of medical management with propranolol at a dose of 2 mg/kg/day was proposed, in accordance with the international clinical practice guidelines for this pathology, all of them agreed. The ages of our patients ranged between 6 months and 6 years of age (5 female and 2 male) (Figures 1 and 2).
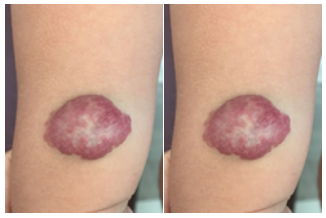
Figure 1: Male 1 year and 6 months of age with lesion on the anterior face of the distal third of the right arm, with 6 months of treatment with propranolol 2 mg/kg/day, favorable evolution, continues under treatment.

Figure 2: Female of 2 years-old with left infra-mandibular lesion, only 5 months of treatment with propranolol 2 mg/kg/day favorable evolution, continues under treatment.
The treatment period was 9 months, of which two cases presented early improvement at the 5th month of treatment and the remaining of the five patients finished the proposed 9-month schedule, observing a clear improvement in the lesions. The protocol proposed at the beginning of the treatment was: all of them were cited at the start week and at 4 weeks in search of alarm data, making a capillary glucose which was normal in all cases on the first appointment (weekly) of initiated the treatment) (Figure 3).

Figure 3: Female of 2 years-old, nose tip lesion and treatment for 9 months with propranolol 2 mg/kg/day, favorable evolution, to date without treatment.
At the control of the 4 weeks one patient presented nauseous state and vomiting so the parents suspended the administration of the medication. The dose is adjusted and restarted with good results in your tolerance. No other patient during the course of their treatment had any complication or side effect such as: bronchial hyperreactivity, gastrointestinal disorder, bradycardia, etc. At the end of the medication dose, one patient required aesthetic surgery of the lesion in the right hemithorax, a procedure that is carried out without complications (Figure 4).

Figure 4: Female with lesion in right hemithorax that required 9 months of treatment with propranolol and cosmetic surgery.
The other three cases corresponded to: male 6 months-old with back lesion; one year- old female with lesion in neck and supraciliary region of the left eye, and female of two years of age with neck lesion (without images).
DISCUSSION
The prevalence of infantile hemangiomas ranges from 4 to 5%. They are the most common benign tumors at this age and most of them regress without requiring treatment. Up to 80% of the hemangiomas reach their final size at three months of age [4].
Infantile capillary hemangiomas can cause damage to vital or sensory organs or cause facial deformities and within the treatment modalities we have corticosteroids as the first line of treatment, interferon alfa [5] and vincristine. Corticosteroids were traditionally considered the first-line treatment, indicated orally, systemically or intralesionally, they are thought to inhibit the production of vascular endothelial growth factor (VEGF) from hemangioma stem cells. Its effectiveness has been seen in the early proliferative phase, despite not knowing exactly its mechanism of action in this type of disease, its use is still in force, prednisone or prednisolone has been recommended 2 mg/day to 3 mg/day, however not there are studies that indicate optimal doses [6].
The use of propranolol has been a priority for the treatment of childhood hemangiomas, its discovery to induce the regression of a facial infantile hemangioma, was while treating a patient with obstructive cardiomyopathy who was administered propranolol, discovery by the group of Leauté -Lebréze in 2008 [7].
Other treatment modalities that have been used are: the pulsed laser, ideal in precursor lesions that manifest as reddish spots or to remove residual telangiectasias, however its greatest use is in ulcerated hemangiomas and its effectiveness is not effective in lesions deep, since the penetration of the laser is 1.2 mm to 1.5 mm [8].
Propranolol has been prescribed for 40 years, within its effects the vasoconstriction it has been proposed as the direct effect on hemangiomas, reflected as a change of coloration in the lesion, inhibits angiogenesis by decreasing the expression of proangiogenic factors, the growth factor of fibroblasts and vascular endothelial growth factor, and produces the apoptosis of endothelial cells, resulting in regression of the lesion [9].
For its use there are still undefined criteria, such as the duration of the treatment, which has been suggested to be at least 6 months. There is a recent consensus that suggests a dose of 1 mg/ kg/day to 3 mg/ kg/day, starting with a dose of 1 mg/kg/day, increasing progressively until reaching the desired dose, prior to the start of treatment, serum glucose must be determined, cardiological assessment, insist on bronchial problems where bronchospasm can be exacerbated. The absence of response should be evaluated after four weeks with treatment ≥2 mg/kg/day where we will consider these cases as resistant to treatment [10].
This last alteration of treatment has come to revolutionize the therapeutic approach of infantile hemangiomas, for having a high response rate with very few adverse effects, we must now consider propranolol the first line medication for its efficacy and safety in pediatric age 6 From the discovery of propranolol as an effective treatment for this pathology, multiple studies have been published supporting this medical management with different results about this treatment [11-17].
CONCLUSION
Physicians in contact with the pediatric population, we have a primary role in the recognition and monitoring of vascular abnormalities of the newborn, in this particular case, infantile hemangiomas that require medical treatment, since this should be initiated as soon as possible (first month of life), it should be noted that after the suspension of propranolol there may be growth of the hemangioma, in which case it may be reintroduced again and usually a clinical improvement occurs again.
Conflict of Interests: None
Funding: This study did not receive funding.
REFERENCES
-
Kollipara R, Dinneen L, Rentas KE, Saettele MR, et al. (2013). Current classification and terminology of pediatric vascular anomalies. AJR Am J Roentgen. 201(5): 1124-1135.
-
Kilcline C and Frieden IJ. (2008). Infantile hemangiomas: How common are they? A systematic review of the medical literature. Pediatr Dermatol. 25(2): 168-173.
-
Balma-Mena A and Lara-Corrales I. (2012). Classification, management and complications of childhood hemangiomas. Acta Pediatr Costarric. 22: 7-13.
-
Léauté-Labrèze C, Harper JI and Hoeger PH. (2017). Infantile haemangioma. Lancet. 390(10089): 85-94.
-
Anger J, Carneiro RG, Pinus J, Ernesto JM, et al. (1998). The rebound effect in the treatment of complex hemangioma with interferon alpha 2A. Sao Paulo Med J. 116(5): 1826-1828.
-
Labastida-Gómez de la Torre O and Moreno-Vázquez K. (2016). Tratamientos actuales de hemangiomas infantiles. Dermatol Rev Mex. 60(4): 319-325.
-
Léauté-Labrèze C, Dumas de la Roque E, Hubiche T, Boralevi F. et al. (2008). Propranolol for severe Hemangiomas of infancy. N Engl J Med. 358(24): 2649-2651.
-
Stier MF, Glick SA and Hirsch RJ. (2008). Laser treatment of pediatric vascular lesions: Port wine stains and hemangiomas. J Am Acad Dermatol. 58(2): 261-285.
-
Kramer D, Muñoz P, Alfaro P, Aranibar DL, et al. (2010). Propranolol in the Treatment of Childhood Hemangiomas. Rev Chil Pediat. 81(6): 523-530.
-
Germán R, Palermo, Zacarías P and Coa N. (2015). Propranolol in the treatment of periocular hemangioma. Presentation of a clinical case. Arch Venez Puericult Ped. 78(4): 120-122.
-
Léauté-Labrèze C, Hoeger P, Mazereeuw-Hautier J, Guibaud L, et al. (2015). A randomized, controlled trial of oral propranolol in infantile hemangioma. N Engl J Med. 372: 735-746.
-
Ahogo CK, Ezzedine K, Prey S, Colona V, et al. (2013). Factors associated with the relapse of infantile haemangiomas in children treated with oral propranolol. Br J Dermatol. 169(6): 1252-1256.
-
Shehata N, Powell J, Dubois J, Hatami A, et al. (2013). Late rebound of infantile hemangioma after cessation of oral propranolol. Pediatr Dermatol. 30(5): 587-591.
-
Tan CE, Itinteang T, Leadbitter P, Marsh R, et al. (2015). Low-dose propranolol regimen for infantile haemangioma. J Paediatr Child Health. 51(4): 419-424.
-
Lou Y, Peng WJ, Cao Y, Cao DS, et al. (2014). The effectiveness of propranolol in treating infantile haemangiomas: A meta-analysis including 35 studies. Br J Clin Pharmacol. 78(1): 44-57.
-
Angera J, Mesquita de Oliveira E and Gabelb J. (2019). Effectiveness of fixed doses of propranolol in the treatment of hemangiomas regardless of child’s weight gain: A case report. Rev Paul Pediatr. pii:S0103-05822019005008104.
-
Antaya RJ. (2019). Infantile Hemangioma. Drug and Dis Dermatol. https://emedicine.medscape.com/article/1083849-overview.