Information Links
Related Conferences
Previous Issues Volume 8, Issue 9 - 2023
Post-Endodontic Restorations Using Direct Fiber-Reinforced Composite Resins: A Case Report
Latifa Hammouda1,*, Amira Kikly2, Fouad Brigui2, Ameni Chadlia Belghith2, Wided Glii2, Neila Zokkar3, Nabiha Douki3
1Endodontic Associate Professor, Dental Medicine Department of the Sahloul Hospital, Sousse-Tunisia, Faculty of Dental Medicine of Monastir, Tunisia
2Endodontic Resident Dental Medicine Department of the Sahloul Hospital, Sousse-Tunisia, Faculty of Dental Medicine of Monastir, Tunisia
3Endodontic Professor Dental Medicine Department of the Sahloul Hospital, Sousse-Tunisia, Faculty of Dental Medicine of Monastir, Tunisia
*Corresponding Author: Latifa Hammouda, Dental medicine department of the Sahloul Hospital, Sousse-Tunisia, Faculty of dental medicine of Monastir, Tunisia; Email: [email protected]
Received Date: September 8, 2023
Publication Date: October 25, 2023
Citation: Hammouda L, et al. (2023). Post-Endodontic Restorations Using Direct Fiber-Reinforced Composite Resins: A Case Report. Mathews J Case Rep. 8(9):124.
Copyright: Hammouda L, et al. © (2023)
ABSTRACT
Objectives: An endodontically treated tooth always poses a challenge for dentists while reconstruction using the post and core system. The objectives of this article are to describe the various properties of fiber-reinforced composite resins with an exploration of their failure causes. Methods: This paper describes the clinical steps involved in reconstruction of maxillary anterior teeth. Endodontic treatment was performed first, followed by the placement of a fiber-reinforced resin post. The crown was then reconstructed with a composite restoration. Result: a clinical and radiological follow-up was performed, showing the success of the reconstruction. Conclusion: Fiber posts have excellent properties, including elasticity, translucency, adaptability, tenacity, and resistance to traction and impact. They are also easy to apply, making them a viable alternative to traditional materials.
Keywords: Fiber post; restorative dentistry; Endodontically treated tooth; Fracture strength
INTRODUCTION
The principal objective of dental treatments is to maintain the lost function and appearance of teeth or dental hard tissues with adequate materials, while preserving the integrity of the tooth and its surrounding tissue [1]. When choosing a restorative material; It should be considered that it is the material that causes the least material loss in the tooth, is the most suitable for the structure of the tooth in terms of morphological and mechanical properties, and is biocompatible with the oral tissues.
The introduction of resin-based composites has brought significant advancements in the field of restorative dentistry. Composite resins offer several advantages, such as their aesthetic appeal, biocompatibility, and absence of mercury, low thermal conductivity, and support for dental tissues after caries removal. As a result, these materials are increasingly preferred by dentists. The Operative Dentistry Academy European Department (AODES) acknowledges composite resins as the preferred restorative material for minimally invasive procedures in posterior teeth, but they also highlight that the structural properties of these materials have not reached an optimal level yet. The longevity of composite resin restorations is influenced by their size, as larger restorations tend to have a shorter lifetime, with fractures being a common cause of failure, particularly in cases of extensive crown destruction. To overcome the limitations of using composite resins with the direct method for large restorations in the posterior region, there has been a growing trend towards utilizing fiber-reinforced composite resin restorations in dentistry [1–3].
Research on fiber reinforcement of dental materials dates back to around 60 years, with the initial use of glass fibers to strengthen acrylic resins in the 1960s. Over time, various types of fibers have been developed to improve the physical and mechanical properties of composite resins. Fiber-reinforced composite materials offer several advantages, including a low modulus of elasticity, good resistance to compression forces, translucency, and effective bonding with resin adhesives. Additionally, fibers act as stress breakers and stress dispersants, thereby increasing the resistance of restorative materials to mechanical forces and reducing polymerization shrinkage [1,4].
The success of composite restorations has been significantly improved with the use of fiber-reinforced composite materials. Thanks to advancements in their structures and their application with the biomimetic restoration technique, the indications for using composite resins as direct posterior restoration materials have expanded. This has led to greater effectiveness and reliability in dental restorations [5].
The aims of this article are to provide an explanation of the properties of fiber-reinforced composite resins with an exploration of their failure causes through a clinical case.
OBSERVATION
An 18-year-old male patient reported to the department of dentistry at the university hospital Sahloul with a chief complaint of sever destruction of lateral left upper incisor 22. Patient’s medical history was noncontributory. Patient gave a history of trauma for 4 days (Figures 1,2). Intraoral examination revealed an amelo-dentinal fracture with the pulp visible through transparency in 22 and the loss of more than half the crown. Intraoral periapical radiographs confirmed a clinical diagnosis (Figure 3).
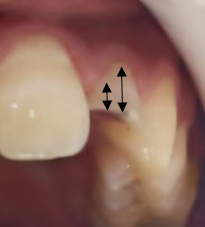
Figure 1: Pre-operative clinical view revealed amelo dentinal fracture with pulp exposure. Note the dentin in the cervical third guaranteeing the adequate ferrule height (black arrows)

Figure 2: Pre operative clinical view revealed the pulp exposure.

Figure 3: Intraoral periapical radiograph revealed coronal fracture of the 222 22 were indicated for pulpectomy, followed by glass fiber-reinforced composite resin post and composite buildups.
The treatment strategy was divided into 2 steps for 22: Endodontic treatment in the first consultation and construction of the restoration in the second step.
Step 1: The Endodontic treatment.
The pulp chamber was opened, pulp tissue was extirpated. The working length was then determined and recorded using an apex locator iPex. Preparation of the canal was carried out using rotary files, Fanta universal system. The root canal was abundantly irrigated with 2,5 % sodium hypochlorite and 17% EDTA solution with a manual agitation during the entire protocol. The canal was dried using paper points. Root canal obturation was performed using a master gutta-percha cone and an eugenate endodontic sealer. The access cavity was closed with a temporary filling (Figure 4).

Figure 4: Periapical radiograph after root canal retreatment 52
Step 2: The construction of restoration.
The preparation of the fiber-post space was performed 1 week after the endodontic treatment. Following the application of a rubber dam and the removal of temporary filling, the intra radicular post space is performed by drilling the canal with Largo drill n° 1 (7/10 mm in diameter) and n° 2 (9/10 mm in diameter) to remove endodontic obturation material, leaving in the apical third 5 mm of gutta percha to ensure apical tightness (Figures 5,6). Then, the size-matched drill corresponding to the type and diameter of the chosen post was selected (Figure 7). The post was sectioned two millimeters below the occlusal surface using a diamond disc (Figure 8). A radiography with a drill in place is made to control the drilling axis and depth (Figure 9). The selected post is then decontaminated into alcohol.

Figure 5: Retreatment of tooth 22 is performed up to WL- 5mm using Largo

Figure 6: Radiographic control after 22 retreatments.

Figure 7: Post space preparation.

Figure 8: clinical post fitting ((pre-cutting of post with diamond disc).

Figure 9: Post fitting (4mm intracoronal) + RX post in place.
The spaces made for the post were acid etched, rinsed with water, and dried (Figure 10): An endodontic needle can be used to facilitate rinsing of the apical part of the post space. The light-cured bonding is applied with a Microbrush® in the post space and dispersed by an air blast. The use of Microbrush® allows a better penetration of the adhesive along the prepared post space (Figures 12,13).

Figure 10: Intraradicular etching with 37% phosphoric acid gel.

Figure 11: Coronal etching with 37% phosphoric acid gel.

Figure 12: Application of adhesive with Microbrush at root canal level, then at coronal level.
Figure 13: Application of light-curing for 20 sec.
The coronal area was etched with 37% phosphoric acid gel on peripheral enamel then dentin for 30 and 15 seconds respectively (Figure 10). Then washed, and bonded using a light cure for 20 seconds.
Light curing is performed in 2 steps: 3 second light curing with a soft intensity to gelate the resin and to allow easy removal of the excess, followed by a 40 second light curing.

Figure 14: Injection of Dual-Cure resin (post pre-coated with resin, then slowly inserted and the coronal part filled at the same time) + light-curing for 40 sc
Light-cure restorative composite is placed by increment in the coronal part using the anterior stratification technique:
- Application of translucent enamel composite (A1) (IPS empress direct) to reproduce the palatal wall and new incisal edge of the teeth with the aid of the silicone index. The composite resin was light cured in position for 20 seconds (Figure 15).
- Application of dentin shade (A3) to create mamelons and reproduce the region that corresponds with the deepest dentin. Dentin can be applied and placed precisely in relation with the future incisal edge (Figure 16).
- Application of shades A1 and High Value for the layer that corresponds to the facial surface (Figure 16).
- Artificial enamel of the final desired shade is applied from the cervical third to the middle and the incisal thirds.
All composites were carefully applied with a flat spatula. Increments of composite resin were light cured for 20 seconds for each layer. A Mylar strip was placed interproximally and pulled through to help create a tight contact point and the correct facial embrasure forms.
Then, both the facial and palatal faces were light cured for 40 seconds (Figure 17). Finally, A coarse-gritted disk was used to produce the primary anatomy and achieve symmetry between similar teeth. The final finishing and polishing were done with finishing burs. Occlusal interferences were removed (Figure 18).

Figure 15: Palatal wall: A1 shade (IPS empress direct set).
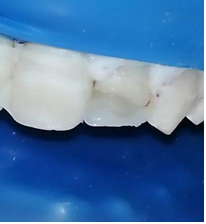
Figure 16: Dentin body (A3 shade) and outer enamel layer.

Figure 17: Bite control and resin finishing.

Figure 18: Final result.
DISCUSSION
Permanent teeth are subjected to a lot of force during normal activities: a maximum force of 90 KGF during biting and a force ranging from 7 to 15 KGF in the chewing. For a restored tooth to be effective, it must be able to withstand these forces over time, particularly to shear forces for anterior teeth [4]. As a result, the direct fiber-reinforced composite resins should resemble dentin and have a proper the forces evenly along the root. Less stress is transferred from the post to the dentin when a fiber post used has a similar elastic modulus to radicular dentin. The modulus elasticity of fiber-reinforced composite posts (FRCP) is close to that of dentin [5,6]. Dentinal bonding is thought to create a homogeneous e mono-entity dentin-post-core system, which would improve the force distribution along the root under.
A greater flexural strength, greater ease of handling, applications in high function-bearing zone, esthetic appearance for young patients and the capacity to attach to any composite are the advantages that glass fiber posts have over other posts [7]. This case report revealed an excellent retention within the canal for a considerable long time. This makes it the preferred technique for badly mutilated anterior teeth, as it is more likely to succeed than other types of posts.
In the other hand, successfully identifying the indication for FRCP is one of the most important steps in avoiding the risk of failure. In our case, despite the persistence of more than three residual walls, each with a thickness and length of more than 1 mm, with a supragingival cervical margin. Switching to full coverage prosthesis is preferable to the RCRP performed. In the anterior sectors, bending forces on the palatal surfaces are important, under the action of shear forces, during the incision and anterior guidance movements [1,6]: this creates a significant lever arm on the underlying prosthetic element [8]. Therefore, it is recommended to use a material with good mechanical resistance to shear and bending in the anterior sector, which is the case for fiber posts, but not for composite resins. This is the case in this article, as the fracture line coincides with the occlusion.
Preserving radicular dentin is essential, and therefore, the canal should not be significantly enlarged beyond the shape created during root-canal instrumentation [9]. In our case, the instrumentation involved the use of a final instrument with a 4% taper, combined with chemical disinfection.
To be able to bond the composite resin and the fiber post in the same session, the filling must be done with warm vertical compaction technique associated to an epoxy-resin root canal sealer [10]. If the obturation is usually done with a cement based on eugenol, cleaning the intracoronal and intraradicular surfaces is essential to obtain perfectly clean surfaces and thus meet the requirements of adhesion [9,10]. The debris of endodontic filling materials that persist on the canal walls are not suitable for bonding. A rigorous cleaning protocol is applied to eliminate these surface contaminations.
In this case report, the root canal filling was made with a eugenate endodontic sealer. In the first step, a mechanical cleaning is performed with the Largo drills and the use of diamond ultrasonic inserts. In a second step, a 17% ethylene diamine tetraacetic acid (EDTA) rinse is used to remove dentin mud, followed by decontamination with chlorhexidine for its antibacterial properties.
Preserving radicular dentin is essential, and therefore, the canal should not be significantly enlarged beyond the shape created during root-canal instrumentation [9]. In our case, the instrumentation involved the use of a final instrument with a 4% taper, combined with chemical disinfection. Regarding the insertion depth of root canal posts, guidelines generally recommend that the post length should match the clinical crown height. Additionally, the post length should occupy approximately one half to two-thirds of the root, while the post length itself should be about half of the length of the root that is supported by bone [3]. Sorensen and Martinoff found a success rate of 97% when the post length was at least equal to the crown height [11]. In this report, a fiber post with a length corresponding to 2/3 of the root was used. A 6 mm length of Gutta-percha was retained to ensure apical sealing. The fiber was chosen to float inside the canal in order not to be in contact with the dentin walls and to be surrounded by the reconstitution resin. But in a way that leaved space to inject a thin layer (from 1 to 1,3 mm) of dual-resin [10].
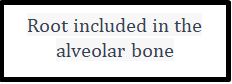
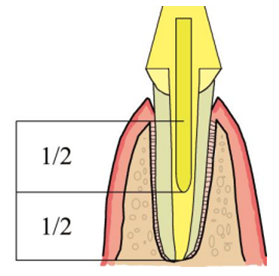
Schema 1: Length of the post according to the alveolar bone.
The integrity, size, density, and distribution of the fibers as well as the type of bond between the matrix and the fibers have been identified as the determining variables for the various flexural strengths [11]. In this case, the fiber post was chosen to "float" in the canal space, thus avoiding the risk of fracture due to the wedge effect [9,11]. The composite resin must be injected into the space so as to fill it completely without leaving any voids [5]. Dyer et al. [12] found that the placement and orientation of different fiber types can affect the fracture stress of FRCP. They showed that test specimens with unidirectional glass fiber reinforcement have increased flexural rigidity, which leads to a higher breakdown load for the post.
In addition, the quality of the bonding, and therefore the adhesion of the different interfaces involved in the assembly (post/bonding system, bonding system/root dentin) determines the long-term success of the restoration [13,14].
For RCRP, the bonding mode was performed by creating a micromechanical and physico-chemical bond. Different studies indicated that the bonding interface posed greater challenges in the apical root dentin compared to the coronal dentin. This difficulty can be attributed, in part, to the morphological distinctions between the two, such as the decreased number, density, and diameter of dentinal tubules [5,11]. This could explain the occurrence of increased adhesion in most coronal sections.
In comparison to self-etching adhesive solutions, the use of etch-and-rinse adhesives produced more resin tags and a thicker hybrid layer. Bond strengths were greatly impacted by moisture control following the application and removal of phosphoric acid as well as by the resin's insufficient penetration of the dentin [15]. Self-etching devices, in contrast, are typically used on dry dentin, do not call for washing the acid, and may therefore be less technique-sensitive. However, there could be interactions between self-etching adhesive systems and the smear layer that remains in the prepared root canal [5]. Additionally, the self-etching adhesive systems' ability to develop patterns of degradation at the resin-dentin interface because of water absorption and increased collagenolytic activity may have a negative impact on how long adhesively bonded posts last [16]. In this case, A dual-cure injectable resin was used, allowing for a homogeneous distribution in the root canal space.
CONCLUSION
Due to an improved performance of adhesive systems, fiber post reconstructions are now reliable and present a reproducible protocol. They must be part of treatment armamentarium to restore endodontically treated teeth. Furthermore, glass fiber posts whose module of elasticity is close to that of dentin are an interesting alternative to metal posts which are often too rigid and responsible for root fractures frequently fatal. A fiber post reconstruction can become loose but the root will be often conserved. At present, easy-of-use “all in one” self-etch and self-adhesive composites are often used for bonding posts. However, the choice of reconstruction type must be determined following to a careful analysis of the clinical situation. There is no unique treatment that fits to all clinical situations. A selected treatment should be a technical solution the best adapted to each clinical case.
REFERENCES
- Tiu J, Belli R, Lohbauer U. (2021). Thickness influence of veneering composites on fiber-reinforced systems. Dent Mater. 37(3):477‑485.
- Agarwal P, Nayak R, Elangovan G. (2018). A Predictable Aesthetic Rehabilitation of Deciduous Anterior Teeth in Early Childhood Caries. Case Rep Dent. 2018:e1742529.
- Naumann M, Schmitter M, Frankenberger R, Krastl G. (2018). Ferrule Comes First. Post Is Second! Fake News and Alternative Facts? A Systematic Review. J Endod. 44(2):212‑219.
- Sorrentino R, Di Mauro MI, Ferrari M, Leone R, Zarone F. (2016). Complications of endodontically treated teeth restored with fiber posts and single crowns or fixed dental prostheses a systematic review. Clin Oral Invest. 20(7):1449‑1457.
- Mehta SB, Bronkhorst EM, Lima VP, Crins L, Bronkhorst H, Opdam NJM, et al. (2021). The effect of pre-treatment levels of tooth wear and the applied increase in the vertical dimension of occlusion (VDO) on the survival of direct resin composite restorations. J Dent. 111:103712.
- Aminian A, Leven AJ, Ashley MP. (2023). Indications for the use of direct composite restorations in the management of tooth wear. Br Dent J. 234(6):395‑399.
- Sonkaya E, Bakır Ş, Bakır EP. (2020). Elution of residual monomers from dental composite resins. Biomed Res. 31 (5): 148-154.
- Wandscher VF, Bergoli CD, de Oliveira AF, Kaizer OB, Souto Borges AL, Limberguer Ida F, et al. (2015). Fatigue surviving, fracture resistance, shear stress and finite element analysis of glass fiber posts with different diameters. J Mech Behav Biomed Mater. 43:69-77.
- Figueiredo FED, Martins-Filho PRS, Faria-e-Silva AL. (2015). Do Metal Post–retained Restorations Result in More Root Fractures than Fiber Post–retained Restorations? A Systematic Review and Meta-analysis. J Endod. 41(3):309‑316.
- Avcılar İH, Bakır Ş. (2023). Use of fiber-containing materials in restorative dentistry. J Dent Sci Education. 49‑54.
- Garlapati TG, Krithikadatta J, Natanasabapathy V. (2017). Fracture resistance of endodontically treated teeth restored with short fiber composite used as a core material—An in vitro study. J Prosthodont Res. 61(4):464‑470.
- Schwartz RS, Robbins JW. (2004). Post Placement and Restoration of Endodontically Treated Teeth: A Literature Review. J Endod. 30(5):289‑301.
- Tanner J, Tolvanen M, Garoushi S, Säilynoja E. (2018). Clinical Evaluation of Fiber-Reinforced Composite Restorations in Posterior Teeth - Results of 2.5 Year Follow-up. Open Dent J. 12:476‑485.
- Mehta SB, Lima VP, Bronkhorst EM, Crins L, Bronkhorst H, Opdam NJM, et al. (2021). Clinical performance of direct composite resin restorations in a full mouth rehabilitation for patients with severe tooth wear: 5.5-year results. J Dent. 112:103743.
- Khan SIR, Ramachandran A, Alfadley A, Baskaradoss JK. (2018). Ex vivo fracture resistance of teeth restored with glass and fiber reinforced composite resin. J Mech Behav Biomed Mater. 82:235‑238.
- Frankenberger R, Winter J, Dudek MC, Naumann M, Amend S, Braun A, et al. (2021). Post-Fatigue Fracture and Marginal Behavior of Endodontically Treated Teeth: Partial Crown vs. Full Crown vs. Endocrown vs. Fiber-Reinforced Resin Composite. Materials. 14(24):7733.