Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
Per-and Post-Operative Mortality in Patients Undergoing Exploratory Laparotomy at a General Hospital in Salvador-Bahia/Brazil
Lucas Chagas Aquino1, Patricia Ramos Borges Ferracioli2, Letícia Chagas Aquino3, André Luis Barbosa Romeo4, Wagner Ramos Borges5,*
1Resident doctor in radiology and imaging diagnosis Hospital Israelita Albert Einstein-São Paulo/Brazil and former medical student Escola Bahiana de Medicina e Saúde Pública, Salvador, Bahia, Brazil
2Pathologist doctor, Hospital Santo Amaro, Salvador, Bahia, Brazil
3Medical student, Escola Bahiana de Medicina e Saúde Pública, Bahia, Brazil
4General and digestive system surgeon, Professor of Escola Bahiana de Medicina e Saúde Pública and Universidade Unime Salvador/Bahia. Full Member Colégio Brasileiro de Cirurgiões, Master in Medicine and Human Health from Escola Bahiana de Medicina e Saúde Pública and preceptor surgeon at the Hospital Ana Neri of Universidade Federal da Bahia, Brazil
5Professor adjunct Escola Bahiana de Medicina e Saúde Pública, Salvador/Bahia, PhD in Medicine and Health–Faculdade de Medicina da Bahia da Universidade Federal da Bahia, vascular surgeon, preceptor doctor at Divisão de Cirurgia Vascular do Hospital Ana Neri da Universidade Federal da Bahia, full member Sociedade Brasileira de Angiologia e de Cirurgia Vascular and Colégio Brasileiro de Cirurgiões, Brazil
*Corresponding Author: Dr. Wagner Ramos Borges, Professor adjunct Escola Bahiana de Medicina e Saúde Pública, Salvador/Bahia, PhD in Medicine and Health–Faculdade de Medicina da Bahia da Universidade Federal da Bahia, vascular surgeon, preceptor doctor at Divisão de Cirurgia Vascular do Hospital Ana Neri da Universidade Federal da Bahia, full member Sociedade Brasileira de Angiologia e de Cirurgia Vascular and Colégio Brasileiro de Cirurgiões, Brazil, Phone: 5571992068592, ORCID: 0000-0001-8653-5265; E-mail: [email protected]
Received Date: November 15, 2023
Published Date: November 29, 2023
Citation: Aquino LC, et al. (2023). Per-and Post-Operative Mortality in Patients Undergoing Exploratory Laparotomy at a General Hospital in Salvador-Bahia/Brazil. Mathews J Cardiol. 7(2):30.
Copyrights: Aquino LC, et al. © (2023).
ABSTRACT
Background: Exploratory laparotomy is the use of the abdominal opening surgical maneuver to search for information and solve adverse problems through the operational environment. Very frequent in the urgency and emergency ambit, this centenary procedure ranks among the main abdominal surgeries. However, its high diagnostic capacity and wide therapeutic capacity, enhanced by current technoscientific advances, are opposed to the high mortality rates related by world literature. Objectives: Describe the per and postoperative mortality rate in exploratory laparotomies performed at a general hospital in Salvador-BA between June 2015 and June 2018, as well as present the clinical-surgical and epidemiological profile of patients who died due to such procedures. Methods: Observational, retrospective, descriptive, cross-sectional study that analyzes 1109 patients undergoing exploratory laparotomy in a general hospital in Salvador-BA. Data collection was performed using surgical records books, as well as patients' medical records. Mortality rate was investigated and, for those who die, epidemiological and clinical-surgical variables were studied in order to describe the profile. Results: 52 patients died (4.68%). It was possible to analyze the clinical-surgical and epidemiological profile in 46 patients. There was a male prevalence, with 34 men (73.9%); The most affected age group was between 19 and 49 years, corresponding to 21 patients (45.7%); Firearm projectile injury was observed in 17 patients (37%); Progression with infection in the postoperative period was reported in 12 patients (26.1%); 23 had septic shock as a cause of death (50%). Conclusion: High per and postoperative mortality rate was found in exploratory laparotomies. Regarding the patients who die, no relation was observed between the time of the procedures and the higher number of deaths. Surgical infection and consequent sepsis proved to be relevant complications among patients who died. The epidemiological and clinical-surgical profile differed from international literature, indicating variability in different contexts and different populations.
Keywords: Exploratory Laparotomy, Mortality, Epidemiological Profile, Clinical-Surgical Profile.
INTRODUTION
Laparotomy (λᾰπάρᾱ = flank; + τομή = cut) means “section of the flank” [1], however, in the concept of most surgeons, the term encompasses the surgical opening of the abdominal cavity. Thus, laparotomy is a surgical maneuver that aims to access the abdominal cavity through an incision in its wall. Among the various possibilities for its use, exploratory laparotomy stands out, which aims to apply the maneuver in order to obtain information not available through other means than surgery [1]. These are usually used in cases where clinical, laboratory and imaging tests are not conclusive regarding the diagnosis, or even in urgent or emergency situations when, due to the severity of the case, time should not be wasted using diagnostic tests several.
Exploratory laparotomy has followed the human evolutionary trajectory since ancient times, becoming routine from the mid-20th century onwards. Given this, its execution and technique have been improved for many decades, which has given this procedure a very high level of importance, both in relation to the historical context and in relation to the present day. Currently, exploratory laparotomy occupies a position among the main surgeries in the emergency environment, being an excellent and consolidated resource for surgeons when approaching the abdome [2].
It is a fact that exploratory laparotomy is capable of making a quick and accurate diagnosis, as well as, due to its broad resolving capacity, providing adequate therapy. Another characteristic is its broad spectrum of action, which can be used in different situations in which the clinical presentation, pathology and perioperative management vary considerably [3]. The use of exploratory laparotomy gains even more prominence at a time when, in the 21st century, there are hospital centers capable of guaranteeing adequate support for a better approach to patients, such as advanced technology, anesthesiological procedures, transfusion support, intensive care centers, among others.
Conduit, despite all the arsenal at its disposal and in contrast to elective laparotomy, exploratory laparotomy still presents high morbidity and mortality rates [4,5]. Furthermore, despite its consolidation in the surgical environment and its century-old nature, there is a lack of data related to per- and postoperative mortality in exploratory laparotomies [6].
This study aims, by describing the mortality rate of patients undergoing exploratory laparotomy in a general hospital in Salvador-BA, and the clinical-surgical and epidemiological profile of those who died following such procedures, to understand possible variables that led patients to death and, by avoiding them, reduce the occurrence of unfavorable outcomes.
In general terms, pre- and post-operative mortality has decreased considerably throughout the evolutionary process of medicine. Before the 1970s, values reached 10,603 per million, rising to 4,533 per million in the 1970s and 1980s, and culminating in 1,176 in the 1990s and 2000s [7]. Despite the considerable reduction in the per- and postoperative mortality rate from procedures in general, when exploratory laparotomies are studied, the numbers are still alarming and often surprising when related to the technological context of the 21st century. This becomes more worrying because it is a common procedure that is part of everyday life in the vast majority of surgical centers. The issue is so important that in January 2010, The Emergency Laparotomy Network was established, an association formed by more than 200 doctors covering 40 hospitals in the United Kingdom. This network aims to share ideas and solutions to improve care for patients undergoing laparotomy and thus obtain better results [6].
Per- and postoperative mortality rates for patients undergoing exploratory laparotomy range between 3.2% and 43.9% in the literature [2-6,8-11,17]. These numbers appear to be enormously discrepant due to the multifactorial nature of different situations and contexts, mainly with regard to epidemiology and the patient's clinical condition, promptness of care and medical-hospital training.
Regarding the epidemiological and clinical-surgical profiles of patients, two of the best-established factors as predictors of mortality in exploratory laparotomy are age and ASA classification [4,6]. A study carried out in the United Kingdom reported a mortality rate in the first 30 days of 14.9% in a total of 1,819 patients undergoing exploratory laparotomy, with 78% of deaths meeting at least one of the following criteria: age greater than 60 years or ASA classification greater than or equal to III [6]. The presence of comorbidities showed a direct relationship with mortality, that is, the more comorbidities the patient has, the higher the mortality rate may be. In 2017, Stevens et al. found, in their study on exploratory laparotomies, mortality rates of 4.25% in patients without comorbidities, 7.42% in those with one to four comorbidities and 19.29% in those with five or more [12]. Furthermore, another independent factor of morbidity and mortality is the emergency nature of the procedures to which patients are subjected [13].
In relation to the care provided by hospitals and their professionals, the surgical mortality rate is also related to the effectiveness and speed of indicating and carrying out the procedure, especially when it comes to emergency surgeries. Delays in operations have been associated with a higher risk of prolonged hospitalization as well as higher costs and higher mortality rates. Study carried out by McIsaac et al. showed that in 2,820 of 15,160 patients undergoing emergency surgeries there was some type of delay in carrying out the procedure. This group had a mortality rate of 4.9%, higher than the 3.2% rate of the group in which there was no delay [14]. Another factor that affects the mortality rate is post-operative management, from access to intensive care beds to optimizing the provision of patient services provided by nursing and physiotherapy [8,10]. A study carried out by Clarke et al. showed that there is an increase in the survival of patients with a prolonged stay in the CRPA compared to patients kept in a surgical Ward [8].
Given all the issues mentioned above, it becomes clear that exploratory laparotomy is a surgery associated with high mortality rates [3]. Although some factors related to such indices are beyond the control of medical care services, most of the predictors are within their reach and can be better controlled. It is known to the scientific community that reducing mortality rates in exploratory laparotomies requires strategies on the part of hospitals and surgical center teams, therefore it is necessary to identify difficulties and improve management in patient care, as well as the effectiveness of the servisse [3,8,14]. Furthermore, there is still a lack of data on pre- and postoperative mortality rates from exploratory laparotomies [6], which reinforces the importance of producing studies on the topic.
MATERIAL AND METHODS
This is an observational, retrospective, descriptive, cross-sectional study, carried out through the analysis of data from the registry of patients operated on in the surgical center of the Hospital Geral Roberto Santos (Salvador–Bahia–Brazil), the largest public hospital in Bahia, SUS reference for the entire state.
Patients undergoing exploratory laparotomy in the service's surgical center, from June 2015 to June 2018, were studied.
The population was selected from the surgical records book. All patients undergoing exploratory laparotomy in the indicated period were included, and patients whose data in the record books and/or medical records were insufficient to carry out the study were excluded, as well as situations in which information about the same patient proved to be duplicated.
Data collection was carried out from June 2019 to November 2019, using the surgical record book, complemented with data from the patients' medical records.
The storage and statistical analysis of the collected data were carried out using the Statistical Package for Social Sciences (SPSS) software.
The work was approved by the CEP of Hospital Geral Roberto Santos/Bahia: number: 3,414,915.
RESULTS
1,109 exploratory laparotomies were performed during the period, of which 52 (4.68%) resulted in death as a pre- or post-operative outcome.
Due to the unavailability of the death certificate, as well as the loss of the medical records of 6 of the 52 patients, data analysis and the epidemiological and clinical-surgical profile were carried out on 46 patients.
The age of the patients was divided into age groups. Thus, of the 46 patients studied, 5 (10.9%) were between 1 and 18 years old, 21 (45.7%) between 19 and 49 years old, 12 (26.1%) between 50 and 64 years old, 7 ( 15.2%) between 65 and 79 years old and 1
(2.2%) over 80 years old (Graph 1). A predominance of men was also observed, with 34
male patients, which corresponds to 73.9% of the study population.
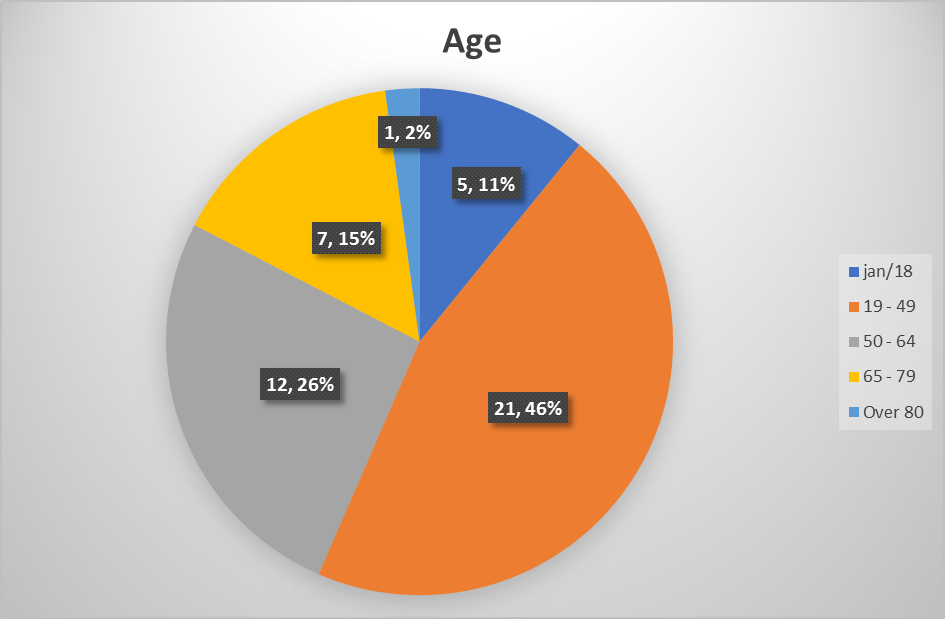
Graph 1. Distribution of patients (by age group) undergoing exploratory laparotomy who died pre- and post-operatively in a reference service; Salvador–Bahia, 2015 to 2018.
Regarding comorbidities, the statistical analysis showed that 5 (10.9%) were diabetic patients, 1 (2.2%) had heart failure with NYHA>2, 2 (4.3%) had arrhythmias, 2 (4.3%) reported a history of coronary artery disease, 3 (6.5%) had dialysis chronic kidney disease and 2 (4.3%) had non-dialysis chronic kidney disease (Graph 2). However, in 28 (60.9%) patients, due to incomplete data, it was not possible to infer the presence of other comorbidities or their absence.
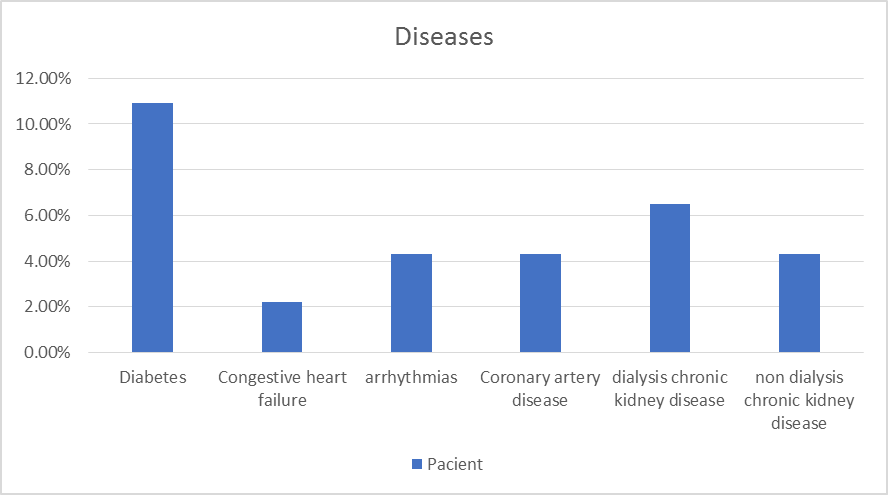
Graph 2. Prevalence of comorbidities in patients undergoing exploratory laparotomy who died pre- and post-operatively at the reference service; Salvador–Bahia, 2015.
There was a prevalence of firearm projectile injury (PAF) in 17 (37%) of the patients who died.
Patients were referred to the operating room in 27 (58.7%) cases from the emergency room, in 6 (13%) from the ICU, in 8 (17.4%) from the wards and in 5 (10.9%) from other locations (Graph 3). Laparotomies were performed as a surgical re-approach procedure in 21 patients (45.7%).
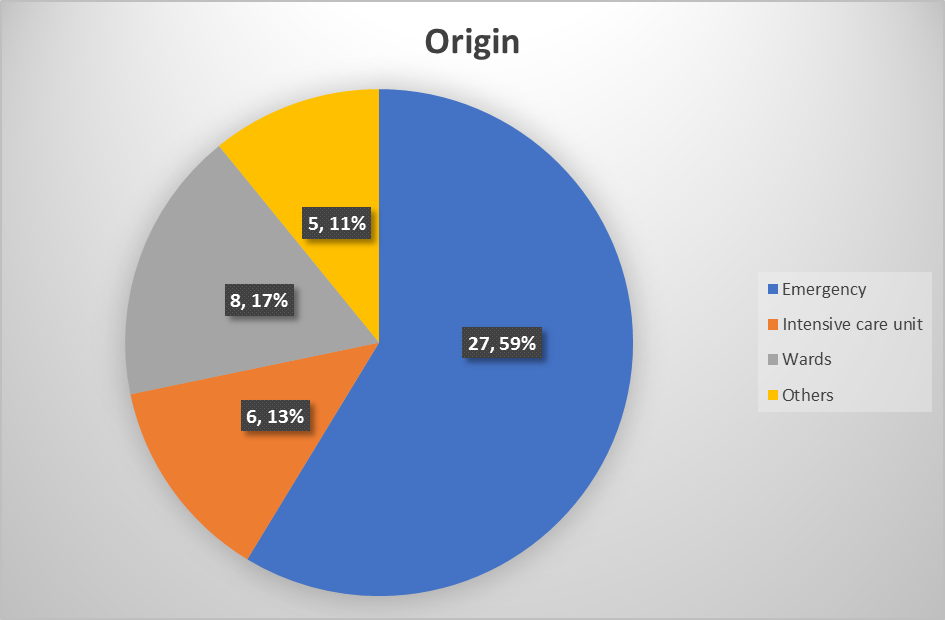
Graph 3. Study of the origin of patients undergoing exploratory laparotomy who died pre-and post-operatively in the reference service; Salvador–Bahia, 2015 to 2018.
The classification of physical status according to the ASA scale (American Society of Anesthesiologists) was obtained through the analysis of the evaluation of the pre-anesthetic record of each patient studied, so that 13 (28.3%) presented ASA I or II, 9 (19.6%) ASA III, 10 (21.7%) ASA IV, 7 (15.2%) ASA V and in 7 (15.2%) cases the ASA was not described (Graph 4).
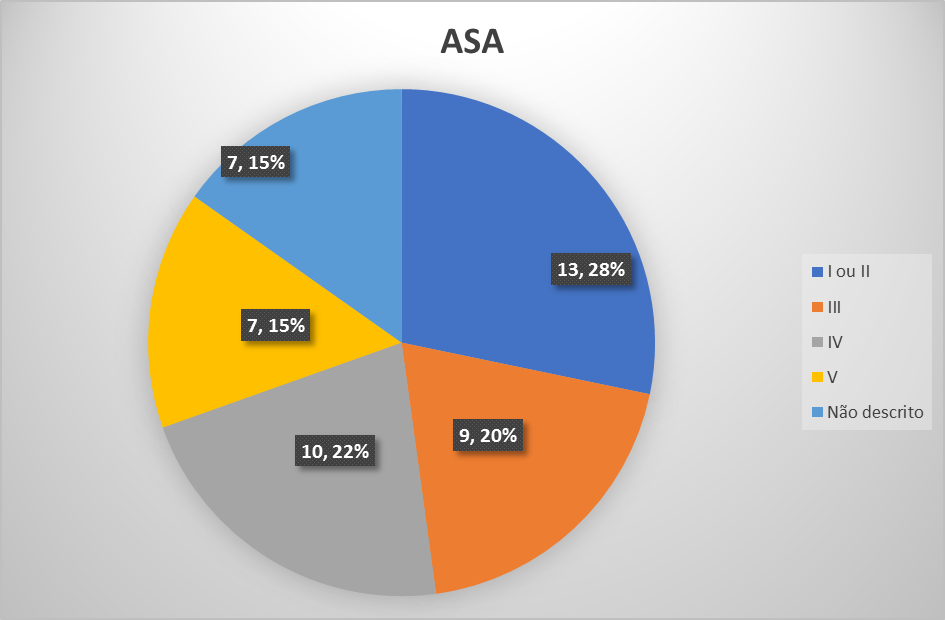
Graph 4. ASA physical status classification in patients undergoing exploratory laparotomy who died pre-and post-operatively at the reference service; Salvador–Bahia, 2015 to 2018.
Per-and postoperative deaths related to exploratory laparotomies were also subjected to temporal analysis, taking into account the date of surgery, as well as the start time of the surgery. The “date” variable was divided into 12 groups, referring to the months of the year, and the “time” variable was divided into 2 groups, the first referring to the time from 7:00 a.m. to 6:59 p.m., and the second to the time from 7 p.m. :00h to 6:59h, as medical shifts are usually divided. Thus, it was found that 5 (10.9%) deaths occurred in January, 3 (6.5%) in February, 7 (15.2%) in April, 2 (4.3%) in May, 6 (13%) in June, 3 (6.5%) in July, 4 (8.7%) in August, 2 (4.3%) in September, 4 (8.7%) in October, 7 (15, 2%) in November and 3 (6.5%) in December. No deaths related to the study were recorded in March (Table 01). Regarding times, a frequency of 52.1% (24 surgeries) was observed for the interval between 7:00 am and 6:59 pm and 47.9% (22 surgeries) for the interval between 7:00 pm and 6:59 am.
Table 1. Temporal distribution (months) of the dates of exploratory laparotomies of patients who died pre- and post-operatively in the reference service; Salvador – Bahia, 2015 to 2018
|
Month of year |
Frequency |
|
|
N |
% |
|
|
01 |
5 |
10,9 |
|
02 |
3 |
6,5 |
|
03 |
0 |
0 |
|
04 |
7 |
15,2 |
|
05 |
2 |
4,3 |
|
06 |
6 |
13 |
|
07 |
3 |
6,5 |
|
08 |
4 |
8,7 |
|
09 |
2 |
4,3 |
|
10 |
4 |
8,7 |
|
11 |
7 |
15,2 |
|
12 |
3 |
6,5 |
|
Full |
46 |
100 |
Table 2. Duration of the procedure (in hours) and length of stay (in days) of patients undergoing laparotomy who died pre- and post-operatively at the reference service; Salvador – Bahia, 2015 to 2018
|
|
Value |
|||
|
Variable |
Average |
Median |
standard deviation |
nterquartile range |
|
Time (hours) |
3,3 |
3,0 |
2,448 |
2,0 |
|
Time of hospitalization (days) |
8,43 |
2,5 |
13,612 |
6,0 |
Postoperatively, 12 (26.1%) patients developed some type of infection.
Regarding the causes that led to death, 18 (39.1%) patients died due to hemorrhagic shock, 23 (50%) due to septic shock, 1 (2.2%) due to spinal cord shock, 1 (2.2% ) due to cardiogenic shock, 1 (2.2%) due to ventricular tachycardia, 1 (2.2%) due to acute myocardial infarction and 1 (2.2%) as a result of mesenteric ischemia (Graph 5).
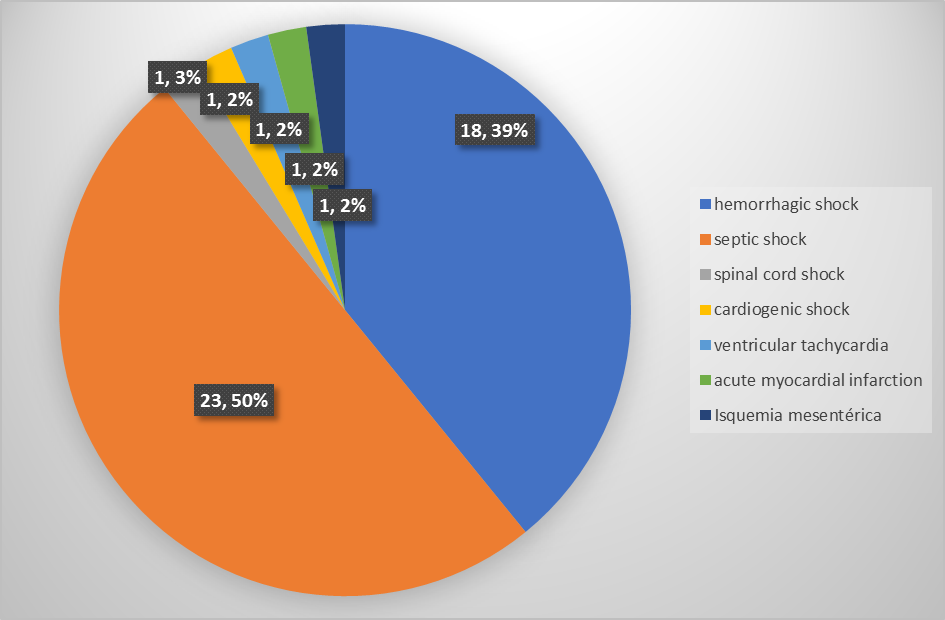
Graph 5. Distribution of causes of death of patients undergoing exploratory laparotomy who had pre-and post-operative evolution in the reference service; Salvador–Bahia, 2015 to 2018.
DISCUSSION
During the study period, 1,109 exploratory laparotomies were performed, of which 52 showed peri- or postoperative death as an outcome, equivalent to 4.68% of procedures. During the same period and in the same hospital studied, 22,493 surgeries were performed with 116 deaths, resulting in an overall surgical mortality rate of 0.51%. The difference between general surgical mortality and mortality in patients undergoing exploratory laparotomies is also observed in the literature, resulting from numerous factors [8]. The first of these is the severity of the patients who undergo the procedure under analysis in this study, as it is natural that those indicated for exploratory laparotomies generally present with greater clinical severity when compared to others scheduled for elective surgeries, thus reflecting directly on the pre- and postoperative mortality rate. Furthermore, as it is usually a major surgery, exploratory laparotomy generates a greater impact on the body compared to less invasive surgeries, as well as presenting a higher rate of complications.
When comparing the results of this study with the data shown in the literature, when performing exploratory laparotomies, a mortality rate (4.68%) was observed close to the lower limit of the results obtained in the scientific literature on the subject (between 3.2% and 43.9%) [2-6,8,10,11]. This, however, does not reflect the efficiency and quality of pre- and post-operative management of the various emergency services, as the patients' epidemiology, clinical picture, promptness of care, intraoperative procedures taken at the time of laparotomy and care pre- and postoperative periods have a great impact on the outcome. The vast majority of studies have as sample selection only patients undergoing exploratory laparotomy in urgency or emergency. In this study, however, the data are insufficient to allow this differentiation due to the fact that it encompasses exploratory laparotomies performed in urgency and emergency, as well as those scheduled electively.
Therefore, it is natural that these are related to a lower mortality rate compared to the former, which is corroborated by Columbus et al. who compared elective and emergency surgeries and reported that emergency surgeries are associated with higher rates of medical errors, complications and deaths [15]. Therefore, it is expected that the exclusive selection of exploratory laparotomies performed in emergency situations will be accompanied by a higher mortality rate. Tan et al. published, in a multicenter study, through the selection of patients undergoing only emergency exploratory laparotomies, a study finding a mortality rate of 13.6% in surgical centers in England and 6.9% in services in New York [5]. In turn, Saunders et al. also restricted their work to the analysis of emergency exploratory laparotomies, observing a mortality rate of 14.9% [6].
It is possible to observe a considerable difference between the mortality reported in the various studies cited and in the present study (4.68%). Despite the multifactorial nature of this variable, this study analyzed patients undergoing elective laparotomies and in an urgent/emergency setting, while the literature usually analyzes patients operated only in an urgent/emergency setting. The vast majority of studies used in the literature review come from countries with a high HDI index and a high outlook on life. In the study carried out in the United Kingdom by Saunders et al, it was reported that 65.5% of patients were over 60 years of age, establishing a relationship of a 4% increase in the mortality rate for every 10 years of life [6]. There is a natural higher probability of complications and even death in such patients, also depending on their pre-operative comorbidities. On the other hand, the majority of deaths reported in the present study (45.7%) correspond to the population between 19 and 49 years old, which makes us observe a low prevalence of the elderly population among the patients studied; Furthermore, there is a high incidence (37%) of patients who died as a result of laparotomies due to gunshot wounds, a phenomenon that mainly affects younger age groups. According to IBGE data in 2018, the year in which data collection for this study was carried out, Brazil had a prevalence of 9.22% of people aged 65 or over, compared to 18.3% of the same age group in 2018 in the Kingdom United Kingdom according to the Office National Statistics, which is the largest independent producer of official statistics in the United Kingdom. In other words, the Brazilian population is younger than the British.
Regarding the epidemiological profile of patients who died, it was possible to observe a prevalence of males (73.9%), as well as the age group of young adults, between 19 and 49 years old (45.7%). Such data demonstrate a strong divergence between the results of the study and the results of the international literature, which generally show a higher frequency of the elderly population and a greater balance between genders. In 2014, research carried out in Germany by Watt et al. which also analyzes mortality in exploratory laparotomies, males represented 40.9% of patients who died, and the most prevalent age group was elderly people over 80 years old (48.9%) [11]. In turn, Clarke et al., in a similar study in the United Kingdom, found a higher prevalence of males (62.5%) among deaths, as well as elderly patients over 80 years old (41.7%) [8].
In addition to these issues, another fact to be highlighted is the high frequency of firearm projectile injuries (37%) among deaths. This element also appears to be something new in relation to those presented in the literature, given that no work cites this issue as a variable. It is possible, therefore, to see a probable relationship between sex, age and prevalence of firearm projectile injuries given the different life contexts experienced by the population of Brazil and the European countries in which the reference studies were carried out. According to the 2018 Violence Atlas, based on data from the Ministry of Health, Brazil reached the mark of 30 murders per 100,000 inhabitants for the first time in history, which corresponds to 30 times the rate observed in Europe. The Atlas also explains the greater epidemiological involvement in the young and male population, and mentions that 71% of the homicides observed were committed with firearms [16]. Therefore, the discrepancy between the European and Brazilian scenarios in relation to violence and exposure to its factors is explicit.
From a regional perspective, Costa et al. analyzed homicide mortality in the city of Itabuna-BA from 2000 to 2012 and established a relationship between the variable and gender and age group. The researchers found that approximately 95% of homicides occurred among the male population, with adolescents and young adults, between 15 and 39 years old, being the most affected age group, reaching the 88% mark in 2012. Furthermore, it was possible to observe that firearms were the most used instrument in such homicides (83%) [17]. Therefore, the relationship observed in this study between young male adults and the high prevalence of firearm injuries is justified given the greater exposure of this population to the hostile scenario experienced in Brazilian cities.
With regard to pre-surgical origin, most of those who died were referred to the surgical center from the emergency department (58.7%). This issue may be a reflection of the fact that emergency surgeries have higher mortality rates. Watt et al. refer, regarding mortality in exploratory laparotomies, that emergency hospitalizations are associated with worse results and higher mortality when compared to elective surgeries [11]
The criteria used in the ASA are one of the best-established factors as predictors of mortality in exploratory laparotomies. Study carried out by Eugene et al. verified 38,830 patients undergoing emergency exploratory laparotomy, observing an increasing mortality rate according to the value of the ASA criteria; reported 2.6% mortality in patients classified as ASA I or II, 9.9% ASA III, 30.8% ASA IV and 58.8% for ASA V [9].
One of the limitations of the current study is the lack of epidemiological and clinical-surgical data, including the ASA criteria, for the total number of procedures performed. Such information was only available for the 46 patients who died, not covering the remaining 1,063 exploratory laparotomies that did not result in death. In this way, the data prove to be limiting for the establishment of possible relationships with mortality, and consequently for comparative analyzes of inferences with the existing literature. The study findings show, among deaths, a slight difference in the number of patients classified as ASA I or II (28.3%) when compared to those classified as ASA IV or V (36.9%). In the literature this difference is much more pronounced, as for example in the study by Saunders et al. in which the frequencies of ASA I or II reached the mark of 8.5% among patients who died, compared to 54.2% of ASA IV or V [6]. In addition to the limitation due to the incomplete nature of the data, the results related to the ASA criteria in the present research still lose part of their value due to the lack of specification of the ASA criteria in the medical records of 15.2% of the studied population. This brings up a question of external no relevant discrepancy was observed between the frequencies of surgery times leading to death. The shift between 07:00h and 18:59h presented 52.1% of deaths compared to 47.9% that occurred in the shift between 19:00h and 06:59h. However, in some studies on the topic, a higher prevalence of deaths was found during non-business hours. Study carried out by Clarke et al. chronologically divided the performance of exploratory laparotomies into two shifts: business hours (between 8:00 am and 5:59 pm on weekdays) and non-business hours (between 6:00 pm and 7:59 am on weekdays and weekends) and observed a prevalence of 70.8% of deaths in procedures performed during non-business hours [8]. Despite this, in no research in which a disparity was found between the frequencies of deaths in relation to the time of surgery, the data were sufficient to establish a direct association with a higher mortality rate. Therefore, the results of the present study are in line with some data found in the literature, bringing a new perspective on this analysis, but without excluding the possibility of the existence of an eventual relationship between the time of surgery and the mortality rate.
In the analysis of the length of stay of patients who died during or after exploratory laparotomies, the mean and median were found, respectively, to be 8 days and 10 hours, with a standard deviation of 13 days and 15 hours, and 2 days and 15 hours, with an interval 6-day interquartile. These data reveal that more than 50% of the studied population had a hospital stay of less than or equal to 2 days and 12 hours, although some patients, with prolonged stays, had a strong influence on the median value, increasing it to 8 days and 10 hours. The shorter hospital stay may be related to the severity of the clinical condition of most patients, associated with the fact that 50% of deaths occurred in the operating room, due to the emergency/severity of the different situations.
In the study by Clarke et al. [8], the median was used as an element of analysis for the results regarding the patients' hospital stay. A median of 11 days was observed for survivors, with an interquartile range of 14 days, and 4 days and 12 hours for patients who died, with an interquartile range of 10 days. In a comparative balance with the present study, a lower median value of deaths (2 days and 12 hours) is observed in relation to the medians found in the study carried out by Clarke et al. (4 days and 12 hours and 11 days) [8]. In this way, precedence is opened for the survey of possible issues that led to such divergence, such as discrepancies between the level of severity of patients, or even between the quality of hospital services offered to them.
Another relevant finding to be highlighted in this study in relation to the results is the high rate of infection as a surgical complication (26.1%) in patients who died postoperatively. In research carried out in India, infection was also the most prevalent setback (26.6%) in the evolution of exploratory laparotomies studied by Gejoe et al. [2]. This variable becomes even more alarming when added to the fact that 50% of deaths, including intra-and postoperative deaths, were caused by septic shock. In the United States, during an analysis of morbidity and mortality from emergency traumatic exploratory laparotomies, Tan et al. found septic shock as the cause of death in 5.4% of cases [5].
The fact that the sample selection of the aforementioned research only encompasses trauma victims causes interference when comparing results, because the most frequent cause of death in trauma victims is hemorrhagic shock, which can reduce the prevalence of trauma. Septic shock as an answer to this question. However, most of the deaths studied here are also related to trauma, which reduces the population differences between the studies compared to the striking difference of almost 10 times the prevalence, proportionally, of septic shock as the cause of death. Although both studies are small and unicentric, the criticism and reflection on the high prevalence of septic shock as a cause of death in current research is valid, since a large part of these deaths can be characterized as preventable. This point deserves attention, since, in the 21st century, sepsis prevention and control practices and protocols are highly widespread around the world, providing health professionals with much greater control over this condition and possible evolution.
This study has some limitations, including its unicentric nature, as well as the low number of patients analyzed. Therefore, the data presented here has neither the intention nor the power to promote generalizations, much less to define conduct. Furthermore, in a more focused view of the topic, the inability to disjudge [18].
CONCLUSION
High pre-and postoperative mortality rates were observed in the analysis of exploratory laparotomies. In the study of procedures that resulted in death as an outcome, no relationship was observed between the time of performance and a higher number of deaths. Surgical infection and consequent sepsis proved to be a relevant surgical complication among patients who died. The epidemiological and clinical-surgical profile of this population was, in part, divergent from the results presented in the world literature, indicating respect for contextual and population particularities. It is necessary to produce larger studies, as well as meta-analyses on the topic so that there is greater consistency and basis in determining mortality predictors.
FINANCIAL SUPPORT
None.
CONFLICTS OF INTEREST
No conflicts of interest declared concerning the publication of this article.
REFERENCES
- De Fátima M. et al. (2011). Laparotomia. Medicina (Ribeirão Preto). 44(1):33-41. Available at: http://revista.fmrp.usp.br/2011/vol44n1/Simp3_Laparotomia.pdf.
- Gejoe G, Yadev I, Rahul M. (2017). Emergency Laparotomies at a Tertiary Care Center-a Hospital-Based Cross-Sectional Study. Indian J Surg. 79(3):206-211.
- Kiernan AC, Waters PS, Tierney S, Neary P, Donnelly M, Kavanagh DO, et al. (2018). Mortality rates of patients undergoing emergency laparotomy in an Irish university teaching hospital. Ir J Med Sci. 187(4):1039-1044.
- Cook TM, Day CJ. (1998). Hospital mortality after urgent and emergency laparotomy in patients aged 65 yr and over. Risk and prediction of risk using multiple logistic regression analysis. Br J Anaesth. 80(6):776-781.
- Tan BHL, Mytton J, Al-Khyatt W, Aquina CT, Evison F, Fleming FJ, et al. (2017). A Comparison of Mortality Following Emergency Laparotomy Between Populations From New York State and England. Ann Surg. 266(2):280-286.
- Saunders DI, Murray D, Pichel AC, Varley S, Peden CJ; UK Emergency Laparotomy Network. (2012). Variations in mortality after emergency laparotomy: the first report of the UK Emergency Laparotomy Network. Br J Anaesth. 109(3):368-375.
- Bainbridge D, Martin J, Arango M, Cheng D; Evidence-based Peri-operative Clinical Outcomes Research (EPiCOR) Group. (2012). Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 380(9847):1075-1081.
- Clarke A, Murdoch H, Thomas MJ, Cook TM, Peden CJ. (2011). Mortality and postoperative care after emergency laparotomy. Eur J Anaesthesiol. 28(1):16-19.
- Eugene N, Oliver CM, Bassett MG, Poulton TE, Kuryba A, Johnston C, et al. (2018). Development and internal validation of a novel risk adjustment model for adult patients undergoing emergency laparotomy surgery: the National Emergency Laparotomy Audit risk model. Br J Anaesth. 121(4):739-748.
- Harvin JA, Wray CJ, Steward J, Lawless RA, McNutt MK, Love JD, et al. (2016). Control the damage: morbidity and mortality after emergent trauma laparotomy. Am J Surg. 212(1):34-39.
- Watt DG, Wilson MS, Shapter OC, Patil P. (2015). 30-Day and 1-year mortality in emergency general surgery laparotomies: an area of concern and need for improvement? Eur J Trauma Emerg Surg. 41(4):369-374.
- Stevens CL, Brown C, Watters DAK. (2018). Measuring Outcomes of Clinical Care: Victorian Emergency Laparotomy Audit Using Quality Investigator. World J Surg. 42(7):1981-1987.
- Stahlschmidt A, Novelo B, Alexi Freitas L, Cavalcante Passos S, Dussán-Sarria JA, Félix EA, et al. (2018). Preditores de mortalidade intra‐hospitalar em pacientes submetidos a cirurgias não eletivas em um hospital universitário: uma coorte prospectiva [Predictors of in-hospital mortality in patients undergoing elective surgery in a university hospital: a prospective cohort]. Braz J Anesthesiol. 68(5):492-498.
- McIsaac DI, Abdulla K, Yang H, Sundaresan S, Doering P, Vaswani SG, et al. (2017). Association of delay of urgent or emergency surgery with mortality and use of health care resources: a propensity score-matched observational cohort study. CMAJ. 189(27):E905-E912.
- Columbus AB, Morris MA, Lilley EJ, Harlow AF, Haider AH, Salim A, et al. (2018). Critical differences between elective and emergency surgery: identifying domains for quality improvement in emergency general surgery. Surgery. 163(4):832-838.
- ECONÔMICA II RESEARCH. (2018). Atlas da Violência. IPEA-Instituto de pesquisa econômica aplicada. 126(1):21. Available at: https://www.ipea.gov.br/portal/images/stories/PDFs/relatorio_institucional/180604_atlas_da_violencia_2018.pdf.
- Costa FA, da Trindade RF, dos Santos CB. (2014). Deaths from homicides: a historical series. Rev Lat Am Enfermagem. 22(6):1017-1025.
- Pimentel SK, Sawczyn GV, Mazepa MM, da Rosa FG, Nars A, Collaço IA. (2015). Risk factors for mortality in blunt abdominal trauma with surgical approach. Rev Col Bras Cir. 42(4):259-264.