Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2023
Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) by Supposed Coronary Thromboembolism by Patent Foramen Ovale (PFO). Should the PFO be Closed?
Mourad Haj Abdo,* Hogir Housen, Matej Holly, Katharina sophie Zistler, Karlheinz Seidl
Clinic of the Cardiology and Intensive Care Unit, Clinic of Ingolstadt, Germany
*Corresponding author: Mourad Haj Abdo, Clinic of the Cardiology and Intensive Care Unit, Clinic of Ingolstadt, Germany, Tel: +49491741985933; E-mail: [email protected].
Received Date: Jaunary 19, 2023
Published Date: Jaunary 31, 2023
Citation: Mourad HA, et al. (2023). Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) by Supposed Coronary Thromboembolism by Patent Foramen Ovale (PFO). Should the PFO be Closed? Mathews J Case Rep. 8(1):85.
Copyrights: Mourad HA, et al. © (2023).
INTRODUCTION
Myocardial infarction is defined as the presence of myocardial injury with elevated levels of heart biomarkers [1]. The important stones in the diagnosis are electrocardiogram, coronary care units, coronary angiography, reperfusion therapies, and troponin assays [2,3]. MINOCA has many causes: plaque disruption, coronary artery spasm, coronary thromboembolism, coronary dissection, myocarditis, and takotsubo cardiomyopathy [4]. In our case, we introduce a patient, who had a myocardial infarction with ST elevation at admission. She had a coronary angiogram, coronary artery disease, and microvascular disease were excluded. As a cause of myocardial infarction, coronary thromboembolism is supposed.
CASE REPORT (HISTORY/CLINICAL EXAMINATION)
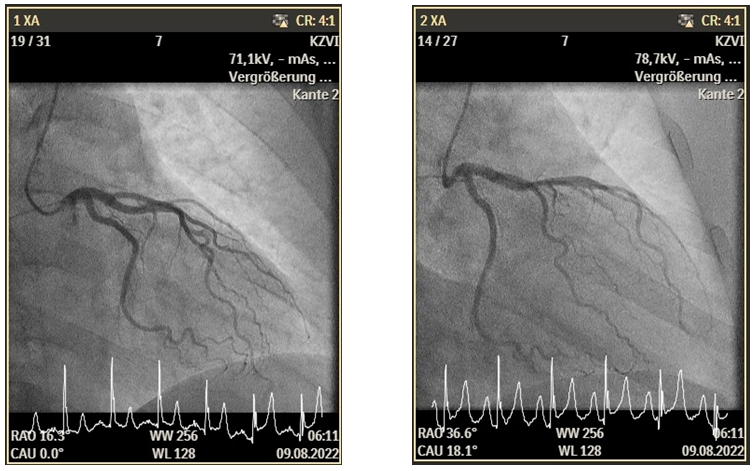
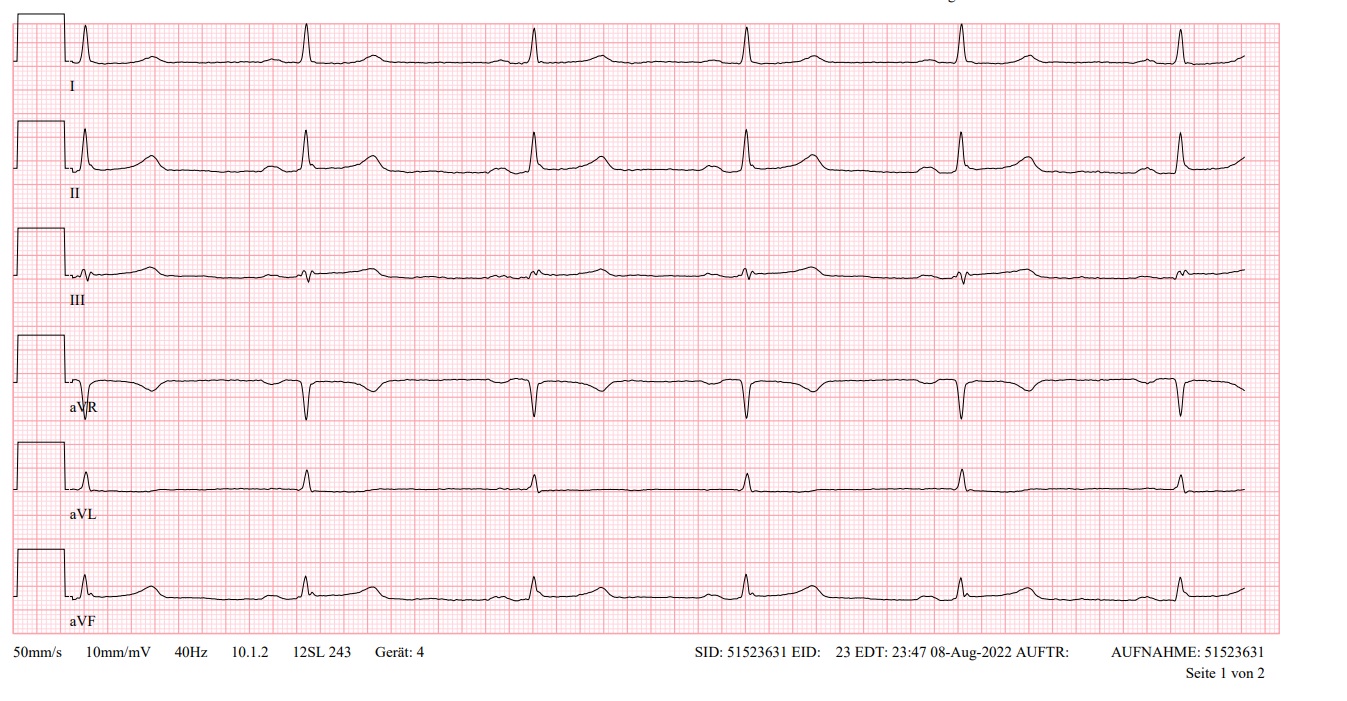
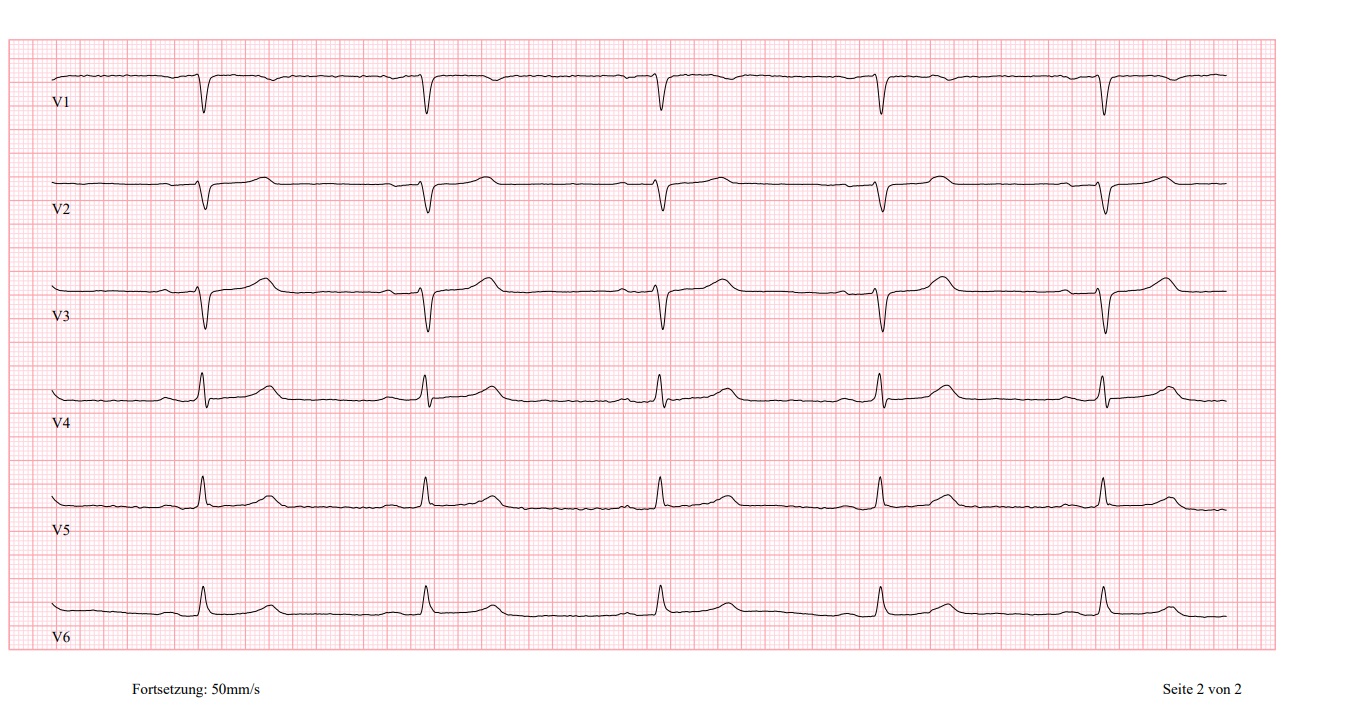
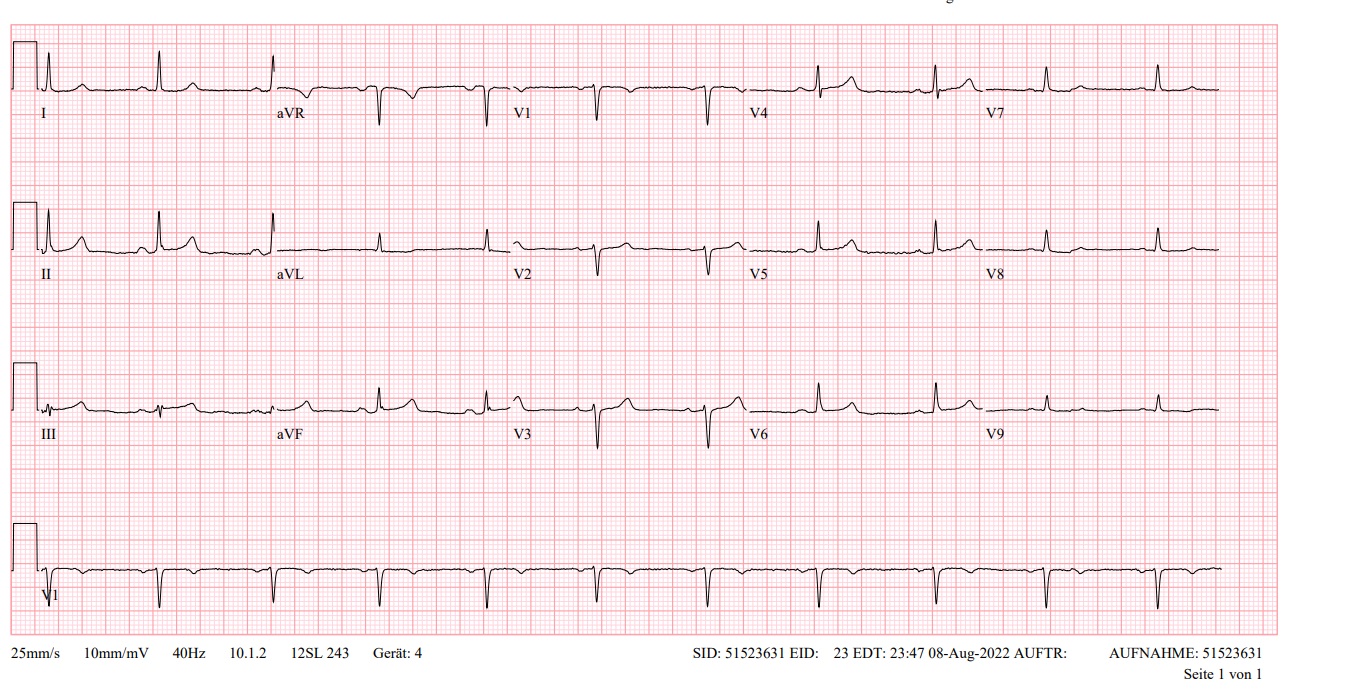
A 47-year-old female presented to our Emergency Department (ED) because of typical chest pain, the patient has never this pain, at admission day was the first time. This patient has no previous history of DM or hypertension. An electrocardiogram was performed, which showed sinus rhythm with ST elevation in II, III, and AVF. This Patient has a hs-TNI at 7ng/dl at hour 0 (normal 2.3-11.6 ng/l), 4 hours after the admission was hs-TNI at 600 ng/dl. The coronary angiogram was without a significant epicardial coronary artery disease. For further evaluation, we measured the microcirculatory resistance (IMR=15) and coronary flow reverse (CFR =3,7) which were not pathologic (Figure 1).
.png)
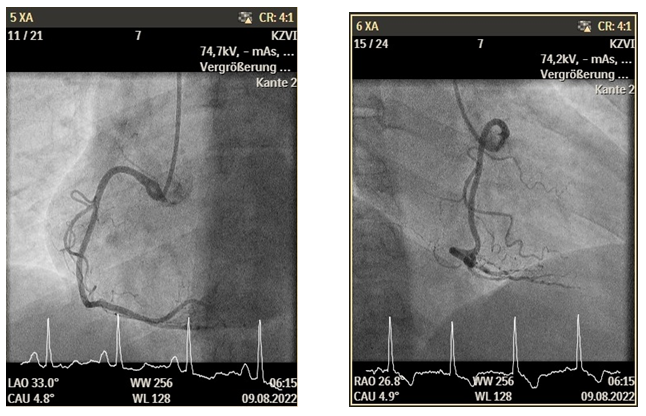
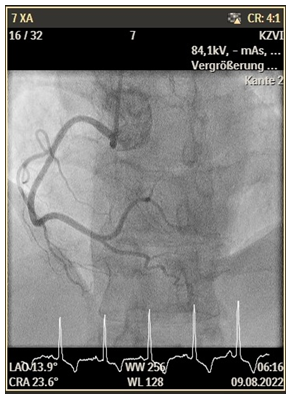
Figure 1. TEE Bilder.
An arterial blood gas showed the following results: pH 7.4 (normal 7.35-7.45), pO2 118 (normal 71-104 mmHg) pCO2 29 (normal 37-43 mmHg), bicarbonate 25.9 (normal 22-26 mmol/L), lactate 1.4 (normal 0.5-2.5 mmol/L), sodium 133 (normal 134-144 mmol/L), potassium 2.7 (normal: 3.5-5.5 mmol/L). The patient suffered from hyperventilation by the stress. Using cardiac-MRI showed a suspected intramural scar in the inferior wall of the heart, Myocarditis and Takotsubo cardiomyopathy were excluded (Figure 2).
.png)
Figure 2. Tees.
In the next day, we have done transesophageal echocardiography (TEE), which showed a patent foramen ovale (PFO). There was no event for left atrial appendage thrombosis, valvular vegetations or Myxoma (Figure 3). The Echocardiographic showed a good systolic ejection fraction of left and right ventricle. Due to the presentation of acute coronary thrombosis and the absence of plaque or vasospasm, a paradoxical embolism or hypercoagulable state was suspected. An autoimmune and thrombophilia screen was conducted and showed no evidence of hypercoagulability.
.png)
Figure 3. Tees.
EKG
DISCUSSION
PFO is common abnormality affecting between 20 % and 35 % of the people [4]. The most of people are asyptomatic, but in some, PFO can enable a paradoxical embolus and cause a thromboemolisation [5]. The majority of paradoxical coronary artery embolism occurrences are missed clinically and remain undiagnosed. High clinical suspicion is required to make the diagnosis. It is an important diagnosis to make as it has an impact on management and prognosis [6,7].
The case was discussed at a heart team meeting and the decision was made to offer the patient percutaneous closure of the PFO. Successful PFO closure was performed using an 18 mm Amplatzer occluder with no acute complications.
CONCLUSION
Paradoxical coronary embolism is a rare cause of acute coronary syndrome. Once suspected, careful imaging including TEE is important for a presumptive diagnosis. In addition to acute management of acute coronary syndrome, PFO closure to prevent recurrent thromboembolism should be considered.
REFERENCES
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD, et al. (2012). Third universal definition of myocardial infarction. Eur Heart J. 33(20):2551-2567.
- Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC), Steg PG, James SK, Atar D, Badano LP, Blo¨mstrom-Lundqvist C, et al. (2012). ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 33(20):2569-2619.
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, et al. (2017). ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 38(3):143-153.
- DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, et al. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med. 303(16):897-902.
- Calvert PA, Rana BS, Kydd AC, Shapiro LM. (2011). Patent foramen ovale: anatomy, outcomes, and closure. Nat Rev Cardiol. 8(3):148-160.
- Giblett JP, Abdul-Samad O, Shapiro LM, Rana BS, Calvert PA. (2019). Patent foramen ovale closure in 2019. Interv Cardiol. 14(1):34-41.
- Saver JL, Carroll JD, Thaler DE, Smalling RW, MacDonald LA, Marks DS, et al. (2017). Long-term outcomes of patent foramen ovale closure or medical therapy after stroke. N Engl J Med. 377(11):1022-1032.