Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
Inguinal and Perineal Necrotizing Fasciitis, A Rare Clinical Manifestation of Necrotizing Pancreatitis: Two Case Reports
Abbas Abdollahi, Majid Ansari*
Endoscopic and Minimally Invasive Surgery Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
*Corresponding author: Majid Ansari, Endoscopic and Minimally Invasive Surgery Research Center, Mashhad University of Medical Sciences, Mashhad, Iran, Tel: +989153230207; E-mail: [email protected].
Received Date: January 27, 2023
Published Date: February 28, 2023
Copyrights: Abdollahi A and Ansari M. © (2023).
ABSTRACT
Acute pancreatitis is a common cause of acute abdominal pain and is associated with several complications. Peripancreatic fluid collection is common, but necrotizing pancreatitis is not as common as it and both of them can be infected. Massive retroperitoneal collection due to necrotizing pancreatitis, which was first presented as necrotizing fasciitis of the inguinal and perineal regions, is an extremely rare presentation of necrotizing pancreatitis. Two cases of this manifestation that were undergone treatment by authors are reported in this article.
Keywords: Acute Pancreatitis, Necrotizing Fasciitis, Retroperitoneal Collection, Case Report.
INTRODUCTION
Retroperitoneal abscess is a rare clinical presentation and that is difficult to diagnose. It can result from various causes, such as pancreatitis, appendicitis, diverticulitis, trauma, malignancy, inflammatory bowel disease, pyelonephritis, spinal infection, peptic ulcer disease, and instrumentation [1]. Acute pancreatitis is a common gastrointestinal disorder [2]. Acute pancreatitis has no specific signs or symptoms, but it can present with nausea, vomiting, and abdominal pain [3,4]. Increased serum levels of amylase and lipase are observed. Serum CRP level and severity of acute pancreatitis have well correlation [3]. Necrotizing pancreatitis is seen in approximately10%–20% of patients with acute pancreatitis [5]. Severe necrotizing pancreatitis has a 20% and 40% mortality rate in patients with sterile necrosis and infected necrosis with multi-organ failure, respectively [6]. Acute pancreatitis etiologies include gallstones, alcohol consumption, trauma, and some medications [7]. Hyperlipidemia is another cause of acute pancreatitis in approximately 10% of cases [8]. According to the revised Atlanta classification 2012, there are two main presentations of acute pancreatitis: acute interstitial edematous pancreatitis which is presented more commonly and necrotizing pancreatitis. Peripancreatic fluid collections are not rare complication and are occurred in 30%-50% of both types of pancreatitis. In most cases, acute peripancreatic fluid collection and acute necrotic fluid collection resolve with conservative management. Surgical intervention is reserved for complications such as hemorrhage, rupture, infection, and fistula formation [7]. Pancreatic or peripancreatic tissue necrosis can become infected in about 30-70% of cases and lead to abscess formation. Necrotizing soft tissue infections are rare infections of the deep tissue and subcutaneous fat and are caused mostly by trauma or perforated visceral organs; however, they are rarely caused by infected retroperitoneal collections. Only three case reports have been published about complicated necrotizing pancreatitis with necrotizing soft tissue infection (NSTI). This complication has a high mortality rate and surgery is the cornerstone of therapy. One possible hypothesis is that cell death and fat necrosis occur after the release of pancreatic enzymes and the consequence is bacterial translocation into the tissue and infected collection [9]. Necrosis of the peripancreatic tissue can lead to the spread necrotic collections along the retroperitoneum, and in rare cases, it can develop into the scrotum [8,10]. One rare complication of necrotizing pancreatitis with mortality rate of 10% to 36% is emphysematous pancreatitis which is characterized by infected necrotic tissues with bubble of gas [11].
CASE ONE
A 57 years old man was admitted to our emergency department (Ghaem Hospital, Mashhad). He had acute abdominal pain, nausea and vomiting and anorexia. He had no past medical history. After complete investigation, acute pancreatitis due to gallstones was diagnosed. The serum levels of amylase and lipase were 1065 and 699, respectively. After ten days of conservative treatment he was discharged. He was readmitted after one month with anorexia, abdominal distention, severe tenderness, and erythema in left inguinal region and scrotum. The patient underwent surgical debridement with a diagnosis of fasciitis necrosis. Computed tomography (CT) scan of the abdomen and pelvis was performed because of continuous pus discharge from the surgical incisions. A large retroperitoneal collection was found on CT scan (Figure 1). He underwent extraperitoneal drainage and debridement with two hockey stick incisions in right and left lower quadrant and about 1lit pus and necrosis was extracted. Fat necrosis has been reported in pathology. He was treated with broad spectrum antibiotics and multiple surgical debridements. The patient was discharged in good condition after 50 days.
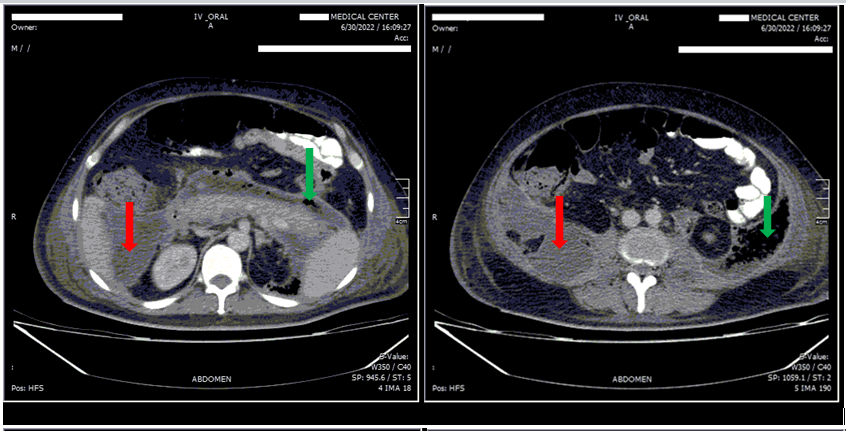
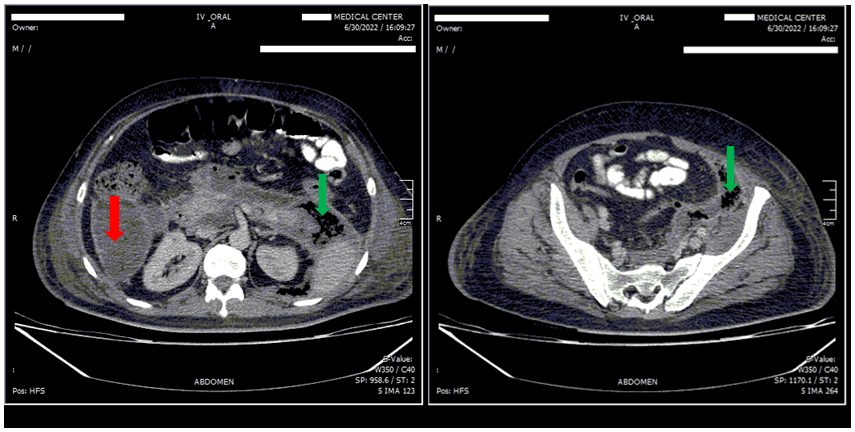
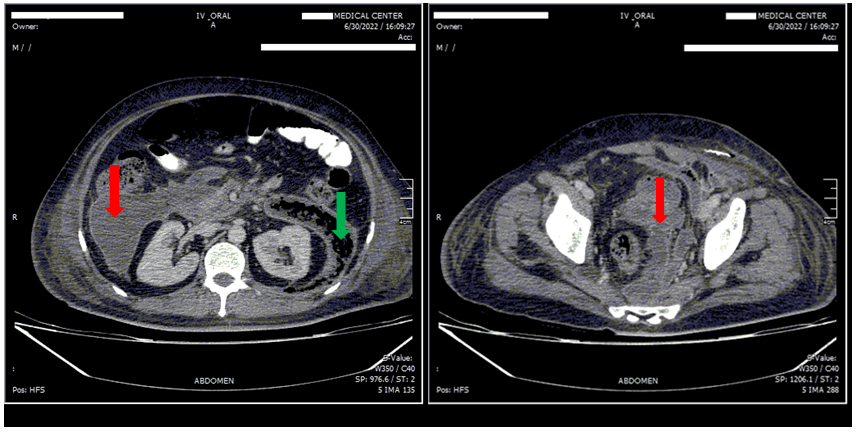
Figure 1. Abdominal and Pelvic CT scan with IV and Oral contrast.
Extremely large retroperitoneal collection from pancreas to the pelvis, includes: fluid collection (red arrows), and gas bubble (green arrows).
CASE TWO
A 62 years old woman was admitted to emergency department with acute abdominal pain, nausea, and anorexia. The patient had past medical history of ischemic heart disease and hypertension. After a complete investigation, acute pancreatitis due to gallstones was diagnosed for her. The patient was discharged from that center after eight days. After 14 days she was readmitted in our emergency department (Ghaem Hospital, Mashhad) with anorexia, abdominal distention, severe tenderness, and erythema in the right inguinal region and right flank. CT scan of abdomen and pelvis was performed (Figure 2). A large right retroperitoneal collection was found on CT scan. First, she underwent percutaneous guided drainage, but it was not effective, therefore, she underwent extraperitoneal drainage and debridement with a right hockey stick incision and 400 cc pus, and necrosis was extracted. The pathology report indicated the presence of fat necrosis. She received broad spectrum antibiotics, and underwent two times surgical debridements. Unfortunately, after two days of second surgery, the patient died due to myocardial infarction and cardiac arrest.
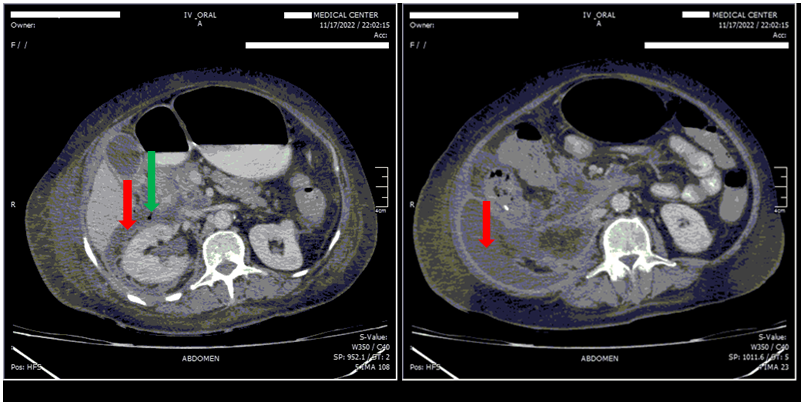
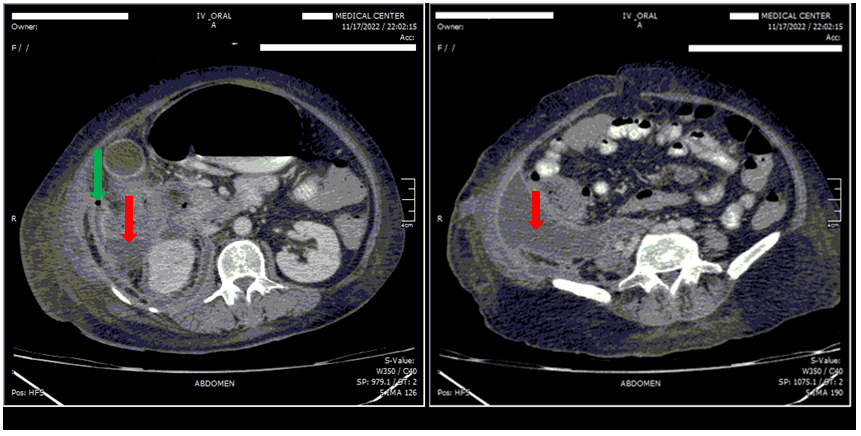
Figure 2. Abdominal and Pelvic CT scan with IV and Oral contrast.
Large right retroperitoneal collection from pancreas to the pelvis, includes: fluid collection (red arrows), and gas bubble (green arrows).
DISCUSSION
Acute pancreatitis has a wide range of presentations, ranging from mild and self-limiting diseases to severe and life-threatening situations [12]. Acute pancreatitis incidence is approximately 33-74 cases per 100000 people per year, and severe disease is seen in about 20% of cases [13]. Necrotizing pancreatitis is classified as sterile or infected. Infection is diagnosed with clinical findings and also CT scan criteria like gas in extraluminal space [14]. Similarly in our two case reports, retroperitoneal gas was found in the extraluminal space. Currently, a less invasive procedure called the step-up approach is the first line of treatment for drainage and debridement in necrotizing pancreatitis. This approach includes percutaneous drainage, endoscopic transgastric necrosectomy, and video-assisted retroperitoneal debridement. Open surgical necrosectomy and debridement are considered when other therapeutic options fail [6]. In this report, open surgery was selected for one patient after percutaneous drainage failed and the clinical condition worsened; in the other patient, due to massive extension of necrosis in the retroperitoneum, the step-up approach was not selected.
Necrotizing soft tissue infection is rare, with an approximately 25% mortality rate. It can be classified as polymicrobial which is the most frequent types and the other type is monomicrobial which is caused, most commonly by group a streptococcus. However, complicated pancreatitis is an extremely rare source of necrotizing soft tissue infection. Although the presence of bacteria is needed to diagnose necrotizing soft tissue infection, culture negative patients have reported, and in this situation, clinical and surgical suspicion is really important [9] In our two cases, polymicrobial infected collections was seen in one case, included; Citrobacter Koseri, Klebsiella Pneumoniae, and Enterobacter, but in the other patient the culture was negative (female patient).
Liquid collection in retroperitoneal space can descend to the scrotum and lead to edema of the scrotum and inguinal region, which is called pancreatic hydrocele, but it is not common [8]. Most patients with pancreatic hydrocele improve with treatment of pancreatic inflammation without surgery, and abscess formation is rare. If an infectious collection is suspected, Fournier’s gangrene is an important differential diagnosis, and that is necrotizing fasciitis of the perineum and external genitalia [8,10]. In this report, the male patient ҆s first differential diagnosis was Fournier’s gangrene, but after the first surgery and CT scan due to continued pus discharge, the necrotizing pancreatitis diagnosis was confirmed.
One study on 20 patients with necrotizing pancreatitis who underwent retroperitoneal laparostomy (right or left lateral incision under the twelfth rib) for drainage and debridement showed a mortality rate of 20%. In addition, fistula formation was reported in 15% of cases. However, this approach does not pose a risk of peritoneal contamination [15]. Retroperitoneal drainage and debridement through the flank incision is an effective technique, however it is recommended for unilateral retroperitoneal collection [16]. In this study, retroperitoneal debridement and drainage were performed through retroperitoneal laparostomy, and no peritoneal contamination or fistula formation was observed. In addition this approach performed in unilateral and bilateral retroperitoneal collection successfully.
CONCLUSION
Necrotizing pancreatitis is one of the mortal clinical presentations of acute pancreatitis. In addition fasciitis necrosis, Fournier’s gangrene and scrotal abscess are extremely rare clinical manifestation of necrotizing pancreatitis. However, it is important to be aware of this rare and mortal complication. Retroperitoneal laparostomy is a good surgical approach for debridement and drainage with no peritoneal contamination, when step-up approach fails or does not applicable. Other studies are needed to be more aware of this rare complication.
ETHICAL APPROVAL
Due to hospital ethical board approval investigation, this case report did not meet the criteria for human subject research.
CONSENT
Written informed consent was obtained from the patients for publication of this case reports and accompanying images.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This case reports did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
- Bansal R, Barakat M, Chun S, Rosberger S, Baum J, Tiba M. (2018). A Case of Unresolved and Worsening Retroperitoneal Abscess. Case Rep Gastrointest Med. 2018:6740734.
- Zhong X, Gong S. (2017). Fatal cerebral hemorrhage associated with acute pancreatitis: A case report. Medicine (Baltimore). 96(50):e8984.
- Chen JH, Chern CH, Chen JD, How CK, Wang LM, Lee CH. (2005). Left flank pain as the sole manifestation of acute pancreatitis: a report of a case with an initial misdiagnosis. Emerg Med J. 22(6):452-453.
- Bălănescu NR, Topor L, Ulici A, Djendov FB. (2013). Acute pancreatitis secondary to hyperlipidemia in an 11-year-old girl: a case report and review of literature. J Med Life. 6(1):2-6.
- Chida K, Ishido K, Sakamoto Y, Kimura N, Morohashi H, Miura T, et al. (2022). Necrotizing pancreatitis complicated by retroperitoneal emphysema: two case reports. Surg Case Rep. 8(1):183.
- Sorrentino L, Chiara O, Mutignani M, Sammartano F, Brioschi P, Cimbanassi S. (2017). Combined totally mini-invasive approach in necrotizing pancreatitis: a case report and systematic literature review. World J Emerg Surg. 12:16.
- Hui D, Hutchinson C, Maine R, Raff L. (2019). A Case of Spontaneous Intraperitoneal Rupture of an Acute Necrotic Fluid Collection Associated with Necrotizing Pancreatitis. Am J Case Rep. 20:459-464.
- Sutalo N, Dragisic V, Miskovic J, Soljic M. (2019). Scrotal abscess as the first symptom of fatal necrotizing pancreatitis. Saudi Med J. 40(11):1167-1170.
- Vervaecke A, van Ierssel S, Vissers G, Macken E, Op de Beeck B, Tondu T, et al. (2022). Necrotizing soft tissue infection of the upper leg as first presentation of necrotizing pancreatitis: a case report. Acta Gastroenterol Belg. 85(3):518-521.
- Chang YH, Weng SY, Shiue SJ, Cheng CL, Wu MS. (2020). Hydrocele in recurrent acute pancreatitis caused by testicular venous obstruction: A case report of a rare complication (CARE-compliant). Medicine (Baltimore). 99(18):e19738.
- Lee SH, Paik KH, Kim JC, Park WS. (2021). Percutaneous endoscopic necrosectomy in a patient with emphysematous pancreatitis: A case report. Medicine (Baltimore). 100(46):e27905.
- Greenberg JA, Hsu J, Bawazeer M, Marshall J, Friedrich JO, Nathens A, et al. (2016). Clinical practice guideline: management of acute pancreatitis. Can J Surg. 59(2):128-140.
- Garg PK, Singh VP. (2019). Organ Failure Due to Systemic Injury in Acute Pancreatitis. Gastroenterology. 156(7):2008-2023.
- Sarr MG. (2013). 2012 revision of the Atlanta classification of acute pancreatitis. Pol Arch Med Wewn. 123(3):118-124.
- Van Vyve EL, Reynaert MS, Lengele BG, Pringot JT, Otte JB, Kestens PJ. (1992). Retroperitoneal laparostomy: a surgical treatment of pancreatic abscesses after an acute necrotizing pancreatitis. Surgery. 111(4):369-375.
- Sriussadaporn S. (2005). Retroperitoneal Approach for Surgical Treatment of Infected Pancreatic Necrosis. THAI Journal of SURGERY. 26:22-26.