Information Links
Related Conferences
Previous Issues Volume 8, Issue 9 - 2023
Incidence of Middle Mesial Canal in the Mandibular First Molar in the Tunisian Population: A Cone Beam Computed Tomography Analysis
Latifa Hammouda1,*, Hamed Harbi1, Sonia Zouiten1, Nabiha Douki2,Faten Ben Amor1
1Out-patient Department of the Dental Clinic of Monastir -Tunisia, Faculty of Dental Medicine of Monastir, Tunisia
2Dental Medicine Department of the Sahloul Hospital, Sousse-Tunisia, Faculty of Dental Medicine of Monastir, Tunisia
*Corresponding Author: Latifa Hammouda, Conservatrice Odontology and Endodontics resident, Out-patient Department of the Dental Clinic of Monastir -Tunisia, Faculty of Dental Medicine of Monastir, Tunisia; Tel: +21628247408; Email: [email protected]
Received Date: September 8, 2023
Publication Date: October 18, 2023
Citation: Hammouda L, et al. (2023). Incidence of Middle Mesial Canal in the Mandibular First Molar in the Tunisian Population: A Cone Beam Computed Tomography Analysis. Mathews J Case Rep. 8(9):125.
Copyright: Hammouda L, et al. © (2023)
ABSTRACT
Objectives: The purposes of this retrospective study were: 1) to assess the frequency of the middle mesial canals (MMCs) in the mandibular 1st molars and its anatomy configuration type in the Tunisian population using CBCT images 2) To correlate the incidence of MMCs with variables of sex, age and presence of a second distal canal. Materials and methods: 123 CBCT images were obtained, between December 2013 to October 2019, from the database of the department of out-patient department, faculty of dentistry, Monastir University. Mesial canals number and mesial canals system configuration CBCT were evaluated by Gallileos Viewer. 196 mature permanent first mandibular molars were included in this study. CBCT images were examined to detect the number of canals and canal configuration. The mesial root canal morphology was categorized and compared according to Vertucci and the Pomeranz classification for the MMCs configuration. Results: The incidence of the presence of MMCs in the first mandibular molars among the Tunisian population was 13.77 % (27/196). The differences in the distribution of MMCs based on sex and presence of a second distal canal were not significant (p>0.05). While MMC configuration types showed 62.96% (17/27) confluent anatomy merging with either the mesio buccal or mesio lingual canals; 29.62% (8/27) fin anatomy and only 7.4% (2/27) showed independent MMCs with separate orifices and apical foramen. The most common mesial root canal morphological type was type II (3-2) (63.63%). This study revealed that MMCs are located equidistant to both the mesio buccal and the mesio lingual canals in 16 cases (59.25%) and are located closer to the mesio buccal canals in 6 cases (22.22%). The frequency of the presence of third mesial canal in the mandibular molars decreases with age. Conclusion: The MM canals prevalence in mandibular 1st molars in the Tunisian population was 13.77 %. CBCT can be a helpful method in the identification and negotiation of this canal.
Keywords: mandibular first molar, Cone Beam Computed Tomography, middle mesial canal, morphology
Abbreviations: MMC: Middle Mesial Canal; MMCs: Middle Mesial Canals; MB: mesio-buccal; ML: mesio-lingual
INTRODUCTION
The success of endodontic treatment depends on the proper chemo mechanical preparation, and obturation of all root canal systems. Complete cleaning and shaping of lateral canals, ramifications, and intercanal communications is a critical step to facilitate healing of the periapical tissues [1,2].
In recent decades, the mesial root configuration of the first mandibular molars has been more widely studied. These roots have a mesiobuccal (MB) canal and a mesiolingual (ML) canal. The narrow communication between the two mesial canals, known as the isthmus, which formed of pulp tissue. Within the isthmus area, many anatomical configurations can be found. Barker et al. (Kuzekanani et al.) were the first authors who revealed the presence of a third mesial canal: the middle mesial canal (MMC) [1].
The MMC orifice ‘s mean diameter has been detected to be 0.16 mm, three times less than the principal mesial canal orifices’ diameter, which is 0.5 mm. The MMC has also the smallest overall volume, 0.20 ± 0.10 mm, in comparison with the main mesial canals (0.75 ± 0.20 and 0.88 ± 0.19 mm, respectively). As a result, it can be ignored in routine clinical inspection [2].
This inability to detect its presence and to adequately shape and obturate, it has been one of the important causes of failure in endodontic treatment of mandibular molars. Dentists must be vigilant of MMC incidence and adopt well-defined steps to locate, treat and obturate it correctly.
The incidence of MMC in mandibular molars has varied from 0.26 to 46.15% %, depending on different factors, including geographic region, age and sex [3].
CBCT has become very useful for initial diagnosis due to its low radiation dose associated to the high resolution. Nowadays, it is considered the gold-standard imaging technique to evaluate the complex anatomy system and to detect the presence of a MMC [4].
Therefore, the purpose of this study was to assess the prevalence of the MMC canal in the Tunisian population, using CBCT analysis and to correlate this incidence with specific variables including age, sex and the presence of a second distal canal.
MATERIALS AND METHODS
This descriptive study was approved by the external consultation department of Monastir dental clinic and was conducted in a private radiology center in Sousse, Tunisia. The CBCT images were obtained from patients, as part of the routine dental examination, diagnosis, and treatment strategy. Thus, who needed implant treatment, oral surgery, orthodontic treatment or endodontics treatment. This retrospective study was approved by the out-patient department.
CBCT scans of 123 patients between December 2013 and October 2019 were collected. In order to the included criteria in this study, the following must be evident on the images of the mandibular first molars:
- lack of root canal obturation
- absence of coronal restorations
- No open apices or radicular resorption;
- Lack of post and core restorations (which may obscure the imaging study)
- Images with high quality and resolution (images with a small field of view), and lack artefacts.
A total of 123 CBCT images were evaluated by Galileos Viewer program. The included images of first mandibular molars were analyzed on the screen in panoramic, sagittal, axial and coronal planes. The MMC was noted only when it could be clearly seen in more than one plane, especially in the axial and coronal views.
The mesiobuccal and mesiolingual canals configuration was initially evaluated by Vertucci classification. The configuration of MMC was determinate according to Vertucci classification and Pomeranz classification.
Data were assessed by SPSS software with Chi square statistical test (α=0.05). This test was used to identify significant difference with: sex (male versus female), age (age < 40 versus age ≥ 40 years) and the presence of second distal canal.
RESULTS AND DISCUSSION
The CBCT images of the first mandibular molars of 123 patients (46 males and 77 female) were observed, and 98 CBCT images met the inclusion criteria with 196 first mandibular molars, among which 27 CBCT images contained MMC. The incidence of MMCs in the sample studied was 13.77%.
The percentage of the MMC in the males and females were 15 and 12 (32.6% vs. 15.58%), respectively. The difference between the two genders was not statistically significant (Chi square, P = 0.28) (P > 0.05).
In this study, the age ranged from 14 years to 63 years. In the teeth with middle mesial canal, the incidence rates of Types I and II canal’s configuration were 18.51% (5 MFMs) and 81.48% (22 MFMs) respectively.
A second distal canal was present in 55.55% (15/27) of the teeth with an MM canal.
Fifteen mandibular first molars with an MMC had 2 distal canals and eleven mandibular first molars with an MM canal had 1 distal canal. Only 1 first mandibular molar with a MM canal had 3 distal canals. Among teeth without an MM canal, 57.39% (97/169) had a second distal canal.
No significant difference exists in the presence of a second distal canal between the teeth with an MMC and those without it (P= 0.619) (P > .05).
Among the 27 MM canals, 17 (62.96%) showed ‘‘confluent’’ anatomy, 2 (7.4%) showed ‘‘independent’’ anatomy, and 8 (29.62%) showed ‘‘fin’’ anatomy (no separate orifice).
In those teeth with ‘‘confluent’’ anatomy, 10 joined the MB canal and 7 joined the ML canal.
This study revealed that MMCs are located equidistant to both the mesio buccal and the mesio lingual canals in 16 cases (59,25 %) and are located closer to the mesio buccal canals in 6 cases (22.22%).
The distribution of MM canals based on sex, age, and presence/absence of a second distal canal is shown in Tables 1,2 and 3.
Table 1: The incidence of middle mesial canals in mandibular first molars of different sex.
|
|
Male |
Female |
Total |
|
With MMC |
32.6 % (15) |
15.8 % (12) |
21.95 % (27) |
|
Without MMC |
63.26 % (31) |
84.41 % (65) |
78.04 % (96) |
|
Total |
37.39 % (46) |
62.6 % (77) |
100% (123) |
|
|
< 20 |
21-40 |
> 40 |
Total |
|
With MMC |
14.81 % (4) |
74.07 % (20) |
11.12 % (3) |
13.77 % (27) |
|
Without MMC |
4.73 % (8) |
68.63 % (116) |
26.62 %(45) |
86.22 % (169) |
|
Total |
6.12 % (12) |
69.38 % (136) |
24.48 % (48) |
100 % (196) |
|
|
2 distal canals |
1 distal canal |
3 distal canals |
Total |
|
With MMC |
55.55 % (15) |
40.74% (11) |
3.7 % (1) |
13.77% (27) |
|
Without MMC |
72.18 %(122) |
26.62 %(45) |
1.18% (2) |
86.22% (169) |
|
Total |
69.89 % (137) |
28.57 % (56) |
1.53% (3) |
100% (196) |
Mandibular first molars (MFMs) are one of the most common endodontically treated teeth in clinical practice. They are the first teeth to erupt, as a result they are more susceptible to aggressions such as tooth decay and trauma [5].
They often have two roots (mesial and distal) and three canals. The mesial root usually presents a vestibular and lingual canal. The distal root commonly has only one central root canal (Vertucci).
Middle mesial canal (MMC) is an additional canal in mandibular molars that is frequently missed due to unawareness about its presence and its low incidence in different populations (Navarro et al.). The percentage rate of MMCs in MFMs varied from 0.26 to 46.15% [6].
Inability to locate and treat the MMC could allow rest of pulp tissue and bacteria to resist in this canal. As a result, periapical inflammation persists causing the failure of the endodontic treatment. This is particularly observed when this is an independent canal type according to the Pomeranz classification (Pomeranz et al.).
Pomeranz et al. classified the MMC into 3 categories (Pomeranz et al.) [8] (Figure 1):
*Independent: The canal has a separate orifice and continues independently without any communication with the mesiobuccal or mesiolingual canals all the way to the apex. (Figure 1 A)
*Confluent: The canal fuses, and then continues with the one of mesiobuccal or mesiolingual canal. (Figures 1 B, C)
*Fin: Along its path, this canal is joined by an isthmus with the mesiolingual or mesiobuccal. As a result, during mechanical preparation, the instrument could pass freely between the mesiolingual or mesiobuccal canal and the MMCs. (Figure 1 D)
The most common type of MMC is: confluent, fin then independent type [1,7].
The first case of three mesial canals with separate orifice and foramen was revealed by Vertucci and Williams [8].
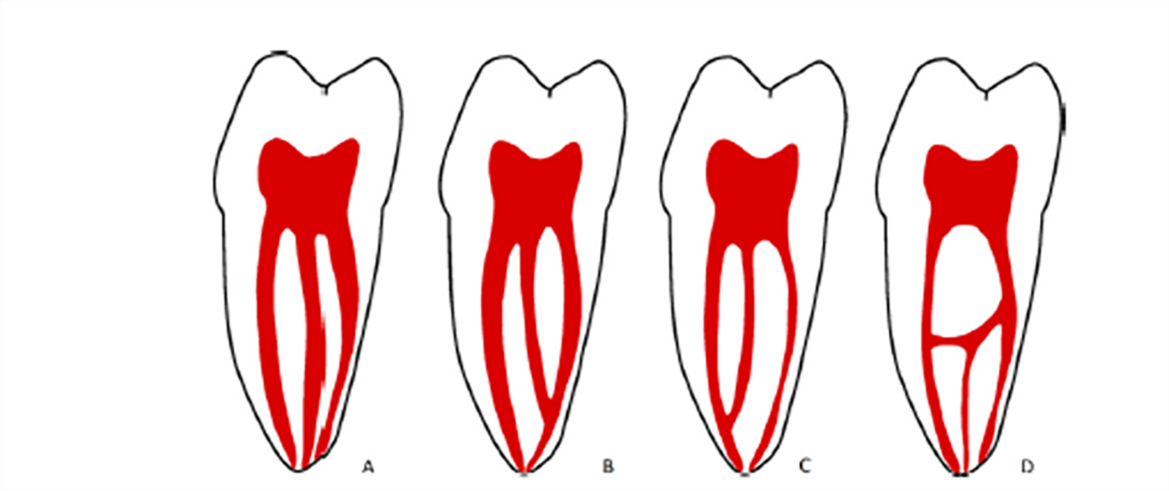
Figure 1: Pomeranz et al. (1981) A) Independent, B) Confluent with MB canal
C) Confluent with ML canal, D) Fin. [9]
Numerous studies have looked at the presence and prevalence of the MMC canal in the first mandibular molars. They have discussed various techniques to identify these canals in vitro and in vivo: ex vivo cross section preparation, clearing, staining, micro–computed tomographic imaging, photomicrographs, and retrospective studies, probing the floor of the pulp chamber to locate root canal orifices (endodontic microscope or an endoscope) [10]. Other reports have suggested using magnification, localization with burs or ultrasonic, enhanced illumination, the ‘‘champagne bubble’’ test, and fiberoptic lighting as tools to detect the additional canals [10].
Conventional intraoral periapical radiographs are essential for the determination of the canal configuration. However, it has its inherent limitation to assess the root canal system completely and to detect an additional canal. More recently, the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology recommended limited field of image CBCT imaging as the view modality of choice for various cases, including the treatment of teeth with the potential for additional canals (American Association of Endodontists et American Academy of Oral and Maxillofacial Radiology, « Use of Cone-Beam Computed Tomography in Endodontics Joint Position Statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology »
Cone-beam computed tomographic (CBCT) imaging showed 3-dimensional imaging of teeth with complex anatomy, such as mandibular molars, with excellent resolution using a relatively low dose of radiation [3,11]
In the literature, a wide variation in the incidence of MMC can be noticed. The study design, procedures and the sample ethnicity, lead to this variation.
In this report, the MMC was present in 27 of 196 (13.77%) first mandibular molars. Our results are in accordance with a similar report by Srivastava et al. (2018) who found an incidence of 18.2% when assessing the CBCT images of 130 Saudi patients [12]. The same for Mohammed E. Rokaya et al. (2022), who found an incidence of 10.79% in the first mandibular molar from the CBCT images of 1650 Egyptian’s patients [13]. Yeqing Yang et al. (2020) revealed a significantly less incidence of MMC compared to our results. Theses authors examined the CBCT data of 875 Chinese patient and found a 9.03% prevalence of MMC in the first mandibular molar [14.15]. The differences in these percentages may be partially attributed to the sample sizes and the used methodology. A systematic review, which included both in vitro and in vivo studies of the internal anatomy of MFMs, revealed 2 canals in 94.4% and 3 canals in 2.3% of the mesial roots [1].
Thus, it can be concluded that the MMC with a frequency of 14.92 %, if not detected, can affect the quality of endodontic treatment.
In our study, we detected only one independent MMCs with a separate foramen. This result is similar to the findings of most reports assessing MMCs in mandibular first molars. The most common MMC categories in our study was the confluent type (8 joined with mesiobuccal canal and 7 joined with the mesiolingual canal) Versiani et al. (2016) showed similar results in their evaluation of 258 M under micro-CT [16,17].
Various studies reveal that MMCs are located equidistant to the MB and ML canals. Whereas other studies reveal that these additional canals are closer to one of the principal mesial canals. Currently, no significant difference in the distance between the MMC–MB orifices and the MMC–ML ones. A various study revealed similar results [2].
On the other hand, no significant differences in the incidence of MMCs were detected with sex. It is consistent with other studies which have found no significant statistical differences in root canal morphology of MFMs according to gender [7].
In the present report, a case of bilateral MMCs was noted in a female. Also, a case of MMC was found in a female who had three distal canals in the mandibular first molar; giving 6 canals in total.
This study shows that the prevalence of MMCs in the mandibular first molars decrease with age. This result due to the accumulation of various factors such as: secondary dentin formation, root canal calcification, periodontal degeneration, tooth wear, root resorption and thickening of cementum [15]. One theory (Peiris et al., 2008) suggests that the prevalence of MMC is more important in the 30–40-year-old age subpopulation, which coincides with the total root canal differentiation [7]. This theory states that the system canal configuration changes and matures after the completion of root edification and closure of the apex [18]. Also, the continuous formation of secondary dentin, within the root canals, leading to a more complicated root canal morphology [18,19].
The incidence of MMCs decreased with subjects older than 40 years old. This finding was related to secondary dentin formation and calcification of the root canal, which reduced the MMC’s diameter. Gulabivala et al., Navid (Jabali) and Fogel (Peiris et al.) revealed that the prevalence of the root canal’s coronal calcification was increased in subpopulations older than 40 years old versus with those younger than 40 years old [7,10,16].
In this study, type II (3-2) was the most common categories. This result was in agreement with previously studies of Chinese, Brazilian, Korean and Egyptian populations [7,12,15,20].
System canal configuration of mandibular first molar is a critical topic because of the high frequency of endodontic treatment on this tooth in routine dental practice. The operating microscope, endoscopes and cone beam imaging are the keys to locate and negotiate MM canals [18,20].
A limitation of this study is the narrow sample size and the use of heterogeneous CBCT imaging that includes volumes with various voxel sizes. This might complicate the detection and the determination of some
MMCs, as a narrow MMC could be missed in case of using a larger voxel size. So, we suggest performing MMC observations with small field of vision and the use of a higher pixel size.
CONCLUSION
The current CBCT analysis evaluated the root canal anatomy of mandibular first molars in a Tunisian population, revealing the prevalence of MMCs. The incidence of middle mesial canal was significant. It is necessary to be more diligent in detecting and locating additional canals during root canal therapy.
CONFLICT OF INTEREST
No financial interest or any conflict of interest exists.
REFERENCES
- Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, et al. (2010). Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod. 36(11):1786‑1789.
- Weinberg EM, Pereda AE, Khurana S, Lotlikar PP, Falcon C, Hirschberg C. (2020). Incidence of Middle Mesial Canals Based on Distance between Mesial Canal Orifices in Mandibular Molars: A Clinical and Cone-beam Computed Tomographic Analysis. J Endod. 46(1):40‑43.
- Srivastava S, Alrogaibah NA, Aljarbou G. (2018). Cone-beam computed tomographic analysis of middle mesial canals and isthmus in mesial roots of mandibular first molars-prevalence and related factors. J Conserv Dent. 21(5):526‑530.
- Studebaker B, Hollender L, Mancl L, Johnson JD, Paranjpe A. (2018). The Incidence of Second Mesiobuccal Canals Located in Maxillary Molars with the Aid of Cone-beam Computed Tomography. J Endod. 44(4):565‑570.
- Forner Navarro L, Luzi A, Almenar García A, Hervás García A. (2007). Third canal in the mesial root of permanent mandibular first molars: Review of the literature and presentation of 3 clinical reports and 2 in vitro studies. Med Oral Patol Oral Cir Bucal. 12(8):605‑609.
- Chen G, Yao H, Tong C. (2009). Investigation of the root canal configuration of mandibular first molars in a Taiwan Chinese population. Int Endod J. 42(11):1044‑1049.
- Peiris HRD, Pitakotuwage TN, Takahashi M, Sasaki K, Kanazawa E. (2008). Root canal morphology of mandibular permanent molars at different ages. Int Endod J. 41(10):828‑835.
- Soares de Toubes KMP, Côrtes MI de S, Valadares MA de A, Fonseca LC, Nunes E, Silveira FF. (2012). Comparative Analysis of Accessory Mesial Canal Identification in Mandibular First Molars by Using Four Different Diagnostic Methods. J Endod. 38(4):436‑441.
- Pomeranz HH, Eidelman DL, Goldberg MG. (1981). Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 7(12):565‑568.
- Gulabivala K, Opasanon A, Ng YL, Alavi A. (2002). Root and canal morphology of Thai mandibular molars. Int Endod J. 35(1):56‑62.
- Mirmohammadi H, Mahdi L, Partovi P, Khademi A, Shemesh H, Hassan B. (2015). Accuracy of Cone-beam Computed Tomography in the Detection of a Second Mesiobuccal Root Canal in Endodontically Treated Teeth: An Ex Vivo Study. J Endod. 41(10):1678‑1681.
- Rokaya ME, Kamel WH, Hassan KS. Middle Mesial Canals Prevalence percentage and Its Configuration type Among Some Egyptian Population by CBCT.
- Yang Y, Wu B, Zeng J, Chen M. (2020). Classification and morphology of middle mesial canals of mandibular first molars in a southern Chinese subpopulation: a cone-beam computed tomographic study. BMC Oral Health. 20(1):358.
- Yang F, Yu L, Li J, Cheng J, Zhang Y, Zhao X, et al. (). Evaluation of concentrated growth factor and blood clot as scaffolds in regenerative endodontic procedures: A retrospective study. Aust Endod J. 49(2):332-343.
- de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. (2010). Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 36(12):1919‑1931.
- Akbarzadeh N, Aminoshariae A, Khalighinejad N, Palomo JM, Syed A, Kulild JC, et al. (2017). The Association between the Anatomic Landmarks of the Pulp Chamber Floor and the Prevalence of Middle Mesial Canals in Mandibular First Molars: An In Vivo Analysis. J Endod. 43(11):1797‑1801.
- Versiani MA, Ordinola-Zapata R, Keleş A, Alcin H, Bramante CM, Pécora JD, et al. (2016). Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch Oral Biol. 61:130‑137.
- Kim SY, Kim BS, Woo J, Kim Y. (2013). Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population: variations in the number of roots and canals. J Endod. 39(12):1516‑1521.
- Bhargav K, Sirisha K, Jyothi M, Boddeda MR. (2017). Endodontic management of contralateral mandibular first molars with six root canals. J Conserv Dent. 20(4):282‑285.
- Karapinar-Kazandag M, Basrani BR, Friedman S. (2010). The operating microscope enhances detection and negotiation of accessory mesial canals in mandibular molars. J Endod. 36(8):1289‑1294.