Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2023
Immune Complex Glomerulonephritis and Elevated p-ANCA Overlap Syndrome in a 58-Year-Old Patient with Rapidly Progressive Kidney Failure
Portinari G1,*, Migali G2, Vasconcelos LC3
1UCLouvain, Brussels, Belgium
2Nephrology department, CHU UCL-Namur, site Namur, Belgium
3UCLouvain, Brussels, Belgium
*Corresponding author: Giacomo Portinari, UCLouvain, Brussels, Belgium; Email: [email protected].
Received Date: January 07, 2023
Published Date: January 24, 2023
Citation: Portinari G, et al. (2023). Immune Complex Glomerulonephritis and Elevated p-ANCA Overlap Syndrome in a 58-Year-Old Patient with Rapidly Progressive Kidney Failure. Mathews J Case Rep. 8(1):83.
Copyrights: Portinari G, et al. © (2023).
ABSTRACT
A 58-year-old man was referred by his family physician for assessment of macroscopic haematuria, leukocyturia, hypertension, and subacute renal failure. On admission, serum creatinine level was 3.39mg/dL and physical examination did not show anything out of the ordinary. Initial tests that showed massive proteinuria (11.83g/24h), significant haematuria (4081rbc/µL) with presence of dysmorphic red blood cells, leukocyturia (64 wbc/µL) with negative bacterial culture, elevated p-ANCA levels (197.7 UI/mL). Renal biopsy results showed a rapidly progressive immune-complex glomerulonephritis with a majority of IgG2 deposits. Secondary causes of immuno-complex glomerulonephritis were extensively searched and excluded. Initial treatment was administered following the p-ANCA glomerulonephritis treatment guidelines (corticoid pulse therapy and cyclophosphamide). Creatinine levels answered poorly to this treatment and the patient ended up needing haemodialysis. A new therapy following the PEXIVAS trial was started at the Cliniques Universitaires St-Luc in Brussels. The patient is nowadays still undergoing haemodialysis, with poor renal function prognosis. Given the surprising presence of both immune complexes and p-ANCA in renal biopsies and the poor answer to the first line treatments of p-ANCA glomerulonephritis, immune complex and p-ANCA overlap syndrome may be evoked as a likely diagnosis.
Keywords: Glomerulonephritis, ANCA, Vasculitis, Overlap Syndrome, PEXIVAS Trials.
BACKGROUND
p-ANCA vasculitis can manifest as glomerulonephritis which, in renal biopsies, usually show no immune complexes, thus deserving the term “pauci-immune” glomerulonephritis [1]. The presence of both p-ANCA and immune complexes in biopsies has already been described in literature [2]. However, its exact prevalence and prognosis are still unknown. Despite the little literature about this topic, the overlap of immune complexes and p-ANCA seems to be more frequent than expected, and thus deserves to be thought upon.
CASE PRESENTATION
A 58-year-old man was referred by his family physician for assessment of macroscopic haematuria, leukocyturia, hypertension, and sub-acute renal failure. Medical history of the patient enlists hypertension treated by perindopril, high cholesterol levels treated by atorvastatin and ulnar neuropathy. His family’s history recalls two precocious deaths of aneurism rupture amongst his brother and father.
The patient was well up until 4 weeks earlier when he noticed changes in urine coloration. He saw his physician who noted worsening hypertension and adjusted his treatment by adding amlodipine. A blood sample was then drawn and showed severely decreased renal function. No other symptoms were reported such as fever, dyspnoea, cough, oedema, pollakiuria, dysuria, mictalgia or cutaneous lesions.
During the first medical contact in the hospital, parameters were the following: 67 BPM, blood pressure 140/80 mmHg, body temperature 36,5°C and oxygen saturation 94% with no oxygen supplementation. Physical examination did not show anything abnormal.
On admission, serum creatinine level was 3.39mg/dL, and later raised up to 4.65mg/dL. Laboratory tests were otherwise within normal values. His serum creatinine level was normal one year earlier (0,76mg/dl).
The initial tests that were run gathered a 24 hours urinalysis that showed massive proteinuria (11.83g/24h), significant haematuria (4081rbc/µL) with presence of dysmorphic red blood cells and leukocyturia (64 wbc/µL) with negative bacterial culture; a blood sample who showed significantly elevated p-ANCA levels (197.7 UI/mL) and no c-ANCA, no antinuclear factor, no anti-GBM antibodies, no anti-phospholipase PLA2R receptor antibodies, no gammaglobulin peak and normal C3-C4 levels; an abdominal CT scan who showed a small non obstructive kidney stone; a renal Doppler ultrasound who found no vascular cause of arterial hypertension.
Macroscopic haematuria was investigated by cystoscopy, which highlighted a bladder polyp. Later biopsy results showed an in situ urothelial carcinoma that was responsible for the blood loss. The polyp was resected, and local chemotherapy was administered once.
Given the clinical picture of subacute renal failure with elevated p-ANCA, dysmorphic red blood cells in urine and massive proteinuria, type II glomerulonephritis was suspected, and a renal biopsy was immediately programmed.
Biopsy results proved to be surprising, as the images were of a rapidly progressive immune-complex glomerulonephritis with a majority of IgG2 deposits. Details of these immune complexes are shown in Table 1. Presence of interstitial nephritis and acute tubular necrosis was also noted.
Table 1. Immunofixation details of renal biopsy.
.png)
Anatomopathologist’s main hypothesis was of a post-infectious glomerulonephritis (auto-immune causes and dysproteinemia were excluded as no significant C1q and heavy or light chains were found in the glomerules).
Latent infections were initially excluded considering many factors in addition to the patient’s small medical history: very little inflammation (measured by C-reactive protein) was found in blood samples, B and C hepatitis serologies were negative and transthoracic echocardiography and intradermic tuberculin tests were found to be normal.
Assessment of extension was initially orientated towards the diagnosis of p-ANCA vasculitis, to exclude pulmonary and ENT lesions. Laryngologist’s consult and head CT-scan showed no significative sinusopathy and pulmonary CT-scan showed no lesions.
p-ANCA vasculitis usually is associated with renal biopsies showing no immune complexes, thus deserving the term “pauci-immune” glomerulonephritis [1]. In this case, given the histological presence of immune complexes, another cause of illness was searched. Immune complex and p-ANCA overlap syndrome was then considered as a potential diagnosis. This condition is already known in literature and has been the topic of a few studies and case reports [2].
While the exact diagnosis was discussed, kidney function started to slowly deteriorate towards high creatinine levels, with the highest number recorded at 4.65mg/dL 10 days after hospitalization. The decision was then made to treat following p-ANCA glomerulonephritis therapy guidelines. Solumedrol pulse-therapy associated with 6 cyclophosphamide cycles was started, to which the renal function answered poorly.
Further examinations were accomplished secondarily to look for latent infections. Two PET-CT were realized, both came up negative for infectious sites such as endocarditis. One showed a few mediastinal lymph nodes but was realised during a SARS-CoV-2 infection, which invalidates the finding.
Five months after the first medical contact, the patient was hospitalised in the Cliniques Universitaires Saint Luc in Brussels for an acutisation of renal insufficiency which required haemodialysis.
A new kidney biopsy was made, which showed the presence of immune complexes as well. The tubules and the interstitium also showed inflammatory damage (acute interstitial necrosis and focal segmental glomerulosclerosis).
Infection assessment was furthered. All haemocultures came back negative. Slow growth bacteria haemocultures were collected and came back also negative. More infectious serologies were tested (Coxiella, Bartonella, Mycoplasma pneumoniae, Chlamydia trachomatis, EBV, CMV, Toxoplasma gondii, parvovirus, HIV, Brucella and Legionella) and all came back negative. Syphilis tests were negative. Trans-oesophageal echography was normal, thus excluding endocarditis. Another PET-CT was realised which showed some hypermetabolism around the thoracic aorta; MRI exploration of this anomaly was reassuring. EBUS was also realised to assess mediastinal lymph nodes; the results were reassuring.
No haematological anomaly was found such as urine monoclonal protein peak or cellular clones. Cryoglobulin testing came back negative.
Giving the refractory nature of the illness, a new corticoid pulse therapy followed by degressive corticoid maintenance was started; 7 plasmatic exchanges were realized; cyclophosphamide was again administered as well as rituximab, following guidelines from PEXIVAS trials [3].
Diuresis returned timidly (500 to 700mL of urine/24h), CRP levels came back to normal, p-ANCA was slightly reduced but haematuria and proteinuria persisted.
The patient was discharged with the objective of undergoing ambulatory dialysis and ambulatory cyclophosphamide – rituximab cycles. He remains until now dependent on haemodialysis, and his renal prognosis has been estimated as poor.
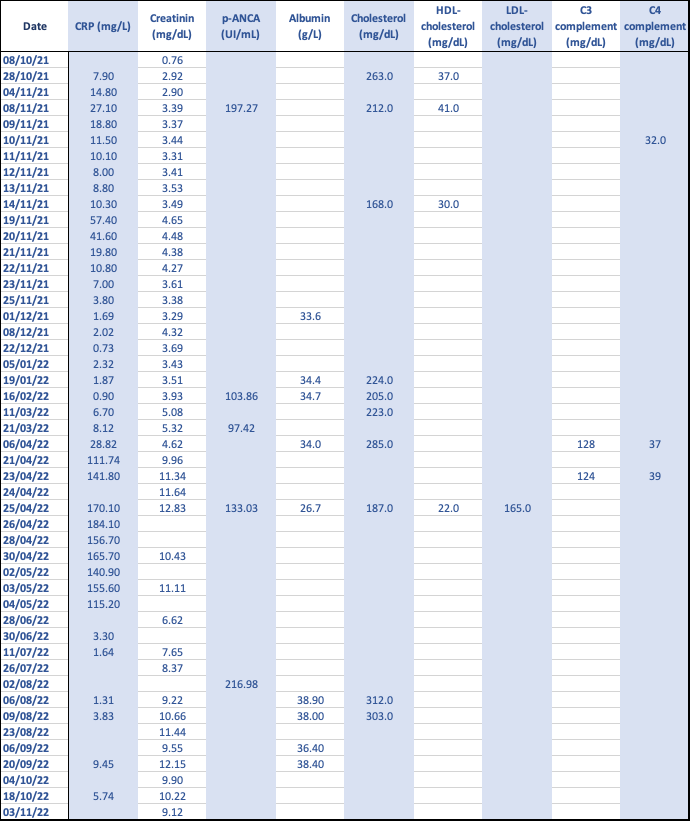
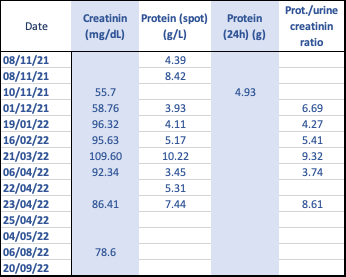
Biological values from diagnosis until the latest tests are reported on Annex 1 & 2.
ANNEX 1: Blood Biological Values.
ANNEX 2: Urine Biological Values.
p-ANCA and immune complex overlap syndrome in literature
Prevalence
The prevalence of overlap syndrome highly variates among studies reporting this condition. IgG associated ANCA glomerulonephritis was recorded going up to 11% of ANCA glomerulonephritis (with half having weak staining only) in a study [4] and C3 complexes were found amongst 40% of analysed cases in another retrospective study [5]. Combined prevalence of IgM and IgG deposits in p-ANCA glomerulonephritis was assessed at 60.6% in another article [6].
The main cause behind these differences could be the immunofluorescence definition of presence of immune complexes, some authors deciding to interpret weak staining as significant, other only going for strong staining. When analysing biopsies with an electronic microscope, this prevalence goes up to 56% [7].
Treatment
In all studies analysed within the redaction of this case report, treatment followed the ANCA-associated vasculitis therapy guidelines. The first line of glucocorticoids with immunosuppressants such as cyclophosphamide or rituximab was the main choice of molecules [8].
Prognosis
A study showed that renal IgG associated p-ANCA vasculitis had no difference in clinical symptoms and renal outcome compared to classic pauci-immune ANCA vasculitis [4]. These authors are however contradicted by another study that associates IgG complex with higher creatinine levels and poorer kidney survival [9]. Other authors seem to notice that these immune complexes seem to be associated with worse proteinuria [10] and with poor long-term renal survival when C3 complexes are found [5].
CONCLUSION
p-ANCA and immune complex overlap syndrome remains a poorly understood diagnosis in its primary form. Its existence in literature is limited to some case reports and a few observational studies. However, some of these papers show that its frequency may be higher than expected. This perhaps calls for a future standardization of diagnosis tools and measurements by experts, so that the importance and impact of this syndrome can be studied more. In the future, new treatment guidelines could be drawn or the same definition of “pauci-immune glomerulonephritis” might be questioned.
Hopefully, this short case report will bring one more piece to the puzzle of knowledge which is being continuously built in the field of glomerulonephritis.
ACKNOWLEDGEMENTS
Authorization to be published anonymously was obtained directly from the patient.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
REFERENCES
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. (2013). 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 65(1):1-11.
- Morizane R, Konishi K, Hashiguchi A, Tokuyama H, Wakino S, Kawabe H, et al. (2012). MPO-ANCA associated crescentic glomerulonephritis with numerous immune complexes: case report. BMC Nephrol. 13:32.
- Walsh M, Merkel PA, Peh C-A, Szpirt WM, Puéchal X, Fujimoto S, et al. (2020). Plasma Exchange and Glucocorticoids in Severe ANCA-Associated Vasculitis. N Engl J Med. 382(7):622-631.
- Dudreuilh C, Fakhouri F, Vigneau C, Augusto JF, Machet MC, Rabot N, et al. (2020). The Presence of RenalIgGDepositsinNecrotizingCrescenticGlomerulonephritisAssociatedwithANCAIsNotRelated to Worse Renal Clinical Outcomes. Kidney Dis (Basel). 6(2):98-108.
- Oba R, Kanzaki G, Sasaki T, Okabayashi Y, Haruhara K, Okabe M, et al. (2021). Long-Term Renal SurvivalinAntineutrophilCytoplasmicAntibody-AssociatedGlomerulonephritisWithComplementC3 Deposition. Kidney Int Rep. 6(10):2661-2670.
- Hirose O, Itabashi M, Takei T, Honda K, Nitta K. (2017). Antineutrophil cytoplasmic antibody-associatedglomerulonephritiswithimmunoglobulindeposition.ClinExpNephrol. 21(4):643-650.
- Haas M, Eustace JA. (2004). Immune complex deposits in ANCA-associated crescentic glomerulonephritis: a study of 126 cases. Kidney Int. 65(6):2145-2152.
- Yates M, Watts RA, Bajema IM, Cid MC, Crestani B, Hauser T, et al. (2016). EULAR/ERA-EDTA recommendationsforthemanagementofANCA-associatedvasculitis.AnnalsoftheRheumatic Diseases. 75(9):1583-1594.
- Lin W, Shen C, Zhong Y, Ooi JD, Eggenhuizen P, Zhou YO, et al. (2021). Glomerular Immune DepositioninMPO-ANCAAssociatedGlomerulonephritisIsAssociatedWithPoorRenalSurvival. Front Immunol. 12:625672.
- Neumann I, Regele H, Kain R, Birck R, Meisl FT. (2003). Glomerular immune deposits are associated with increased proteinuria in patients with ANCA-associated crescentic nephritis. Nephrol Dial Transplant. 18(3):524-531.