Information Links
Related Conferences
Previous Issues Volume 11, Issue 2 - 2026
Exploring the Spectrum of Bilirubin-Induced Brain Injury: A Case of Spastic Cerebral Palsy and Sensorineural Hearing Loss Post-Kernicterus
Aamir Jalal Al-Mosawi*
Advisor Doctor and Expert Trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq
*Corresponding Author: Aamir Jalal Al-Mosawi, Advisor Doctor and Expert Trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq, Email: [email protected]
Received Date: April 02, 2026
Published Date: May 22, 2026
Citation: Al-Mosawi AJ. (2026). Exploring the Spectrum of Bilirubin-Induced Brain Injury: A Case of Spastic Cerebral Palsy and Sensorineural Hearing Loss Post-Kernicterus. Mathews J Case Rep. 11(2):225.
Copyrights: Al-Mosawi AJ. © (2026).
ABSTRACT
Background: Kernicterus is a rare neurological condition caused by bilirubin toxicity, typically leading to dyskinetic or choreoathetoid cerebral palsy and sensorineural hearing loss. This condition usually involves injury to deep brain structures like the globus pallidus and subthalamic nuclei, but emerging reports suggest variability in clinical outcomes. This report describes an unusual case of spastic cerebral palsy and hearing loss following kernicterus, with MRI findings suggestive of both classic kernicterus and features more typical of spastic cerebral palsy. Patients and methods: A 6-year-old boy from South Africa developed severe hyperbilirubinemia (total serum bilirubin exceeding 30 mg/dL) shortly after birth, requiring exchange transfusion. Despite no history of perinatal asphyxia, the child developed acute bilirubin encephalopathy. When seen at the age of six, he had severe spasticity, impaired head control, and poor alertness, with no dystonic or choreoathetoid movements. MRI at 2 years showed basal ganglia involvement, periventricular white matter changes, corpus callosum thinning, and cerebral atrophy. Hearing assessment revealed severe bilateral sensorineural hearing loss. Results: The child received a multimodal neurorestorative therapy regimen, including cerebrolysin, piracetam, citicoline, baclofen, and nutritional support. Over the course of a month, notable improvements were observed: increased alertness, social responsiveness, improved head control, reduced spasticity, and the ability to chew solid food for the first time. Conclusion: This case demonstrates an atypical presentation of kernicterus with spastic cerebral palsy and sensorineural hearing loss, raising questions about the variability in bilirubin-induced brain injury. It also underscores the potential for significant functional recovery with multimodal neurorestorative therapy, even in severe cases.
Keywords: Kernicterus, Spastic Cerebral Palsy, Sensorineural Hearing Loss, Bilirubin Encephalopathy, Neurorestorative Therapy, Neuroplasticity.
INTRODUCTION
Kernicterus is a neurological condition caused by bilirubin neurotoxicity early during life. Excessive hyperbilirubinemia with accumulation of bilirubin in the grey matter of the brain cause irreversible brain damage, and a variety of chronic neurological conditions including cerebral palsy mostly dyskinetic and choreoathetoid types and mental retardation.
The neuropathology of bilirubin-induced brain injury has been described for over a century. In 1847, Jaques Hervieux autopsied 44 jaundiced infants and He described jaundice of the brain in 31 of his 44 autopsied cases, with variable intensity of staining.
In 1875, Johannes Orth reported the autopsy of one jaundiced term infant. The brain was characterized by an intense yellow staining of the basal ganglia, the wall of the third ventricle, the hippocampus, and the central parts of the cerebellum.
In 1903 Christian Schmorl described his findings on 120 autopsies of jaundiced infants. He emphasized the occurrence of intense yellow staining in the basal ganglia and other brain nuclei. All autopsied brains were jaundiced, but only 6 cases showed a staining similar to that described earlier by Orth. Schmorl used the term kernicterus (jaundice of the basal ganglia) to describe the staining pattern [1-7].
The association of kernicterus with hearing loss has been reported as early as 1950 [8].
Kernicterus is classically associated with dyskinetic and choreoathetoid cerebral palsy, resulting from selective injury to deep brain structures including the globus pallidus and subthalamic nuclei. Sensorineural hearing loss is also a hallmark. However, spastic cerebral palsy, especially in a quadriplegic distribution, is typically linked to white matter or cortical injury, often due to periventricular leukomalacia or hypoxic-ischemic encephalopathy [1-9].
This report describes a child with severe spastic cerebral palsy and hearing loss following kernicterus with no history of birth asphyxia. Magnetic resonance imaging (MRI) revealed features suggesting both kernicterus and spastic cerebral palsy, raising the possibility of an atypical or mixed presentation.
PATIENTS AND METHODS
A 6-year-old boy from South Africa was born at term following an uncomplicated pregnancy and delivery. Early-onset jaundice developed in the neonatal period, with total serum bilirubin levels exceeding 30 mg/dL. Exchange transfusion was performed. The infant subsequently developed signs of acute bilirubin encephalopathy, including irritability, poor feeding, and seizures, which were controlled with levetiracetam (Keppra) which was given for few months.
There was no history of perinatal asphyxia, and the mother was Rh-positive, excluding Rh isoimmunization.
When the child was seen on October 4, 2025, he exhibited significant spasticity, despite being on a daily dose of 20 mg of baclofen, divided into two doses. His movements were severely restricted, with an equinus/plantar flexion deformity that could only be corrected (dorsiflexed) with difficulty. Additionally, there were marked flexions at both the elbow and wrist, and he had poor head control.
His level of alertness to his environment was low, and he was not recognizing his parents or sister. During the clinic visit, he did not produce any sounds; however, his parents reported that he occasionally vocalized at home.
No clear dystonic, choreiform, or athetoid movements were observed.
Magnetic Resonance Imaging and MR Spectroscopy was performed at the age of 2 years (16th February, 2019).
Technique: Sagittal T1 3-D with axial and coronal reformats. Axial T2, FLAIR, DWI and SWI. Coronal T2 fat sat. MRS left basal ganglia and left parietal white matter.
IV Contrast: None given.
Findings included:
- Age-appropriate myelination with generalized supratentorial volume reduction with prominent ventricles and extra-axial cerebral convexity CSF spaces.
- Bilateral symmetrical abnormal T2/FLAIR hyperintensity involving the globus pallidum (primarily dorsomedial aspect), the thalami (primarily pulvinar region with some volume loss) and subthalamic nuclei. No corresponding abnormal T1 signal changes.
- There is involvement of periventricular confluent white matter without evidence of hemorrhage or mineralization on SWI.
- Mild diffuse thinning of the corpus callosum. Small pituitary gland with absent ostia pituitary T1 hyperintensity.
- Unremarkable posterior fossa structures.
- The mastoid air cells and paranasal sinuses are grossly clear.
MRS study shows normal choline/creatine ratios and NAA peak with no evidence of significant lactate.
Hearing Assessment performed on the 16th February, 2019 showed bilateral severe sensorineural hearing loss (Thresholds ~75–90 dB HL).
Tympanometry: Normal middle ear function.
Oto Acoustic Emissions Test (DPOAE) [Figure-1A]: No responses in either ear indicating cochlear outer hair cell dysfunction.
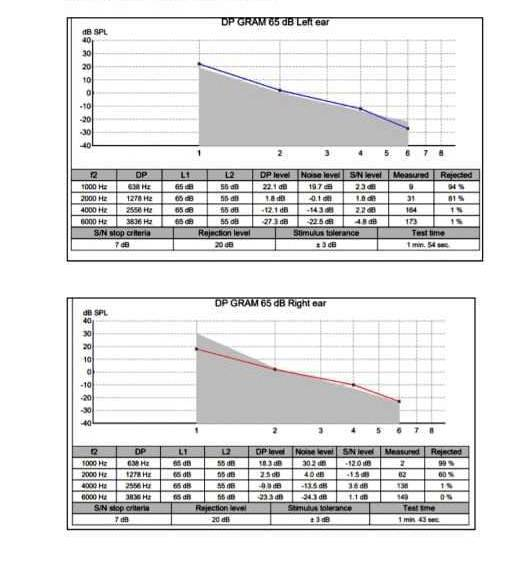
Figure-1A. Oto Acoustic Emissions Test (DPOAE): No responses in either ear indicating cochlear outer hair cell dysfunction.
Brainstem Auditory Evoked Response Test [Figure-1B]: Normal waveform morphology, moderate to severe sensorineural hearing loss.
Auditory Steady State Response Test [Figure-1C]: Thresholds across the frequency spectrum 500Hz to 4KHz reflected severe sensorineural hearing loss.

Figure-1B. Brainstem Auditory Evoked Response Test: Normal waveform morphology, moderate to severe sensorineural hearing loss.

Figure-1C. Auditory Steady State Response Test: Thresholds across the frequency spectrum 500Hz to 4 KHz reflected severe sensorineural hearing loss.
RESULTS
The therapeutic intervention was based on our extensive published experiences with the treatment of cerebral palsy and kernicterus [1-7,9-13], which included multimodal neurorestorative therapies:
First week (Started on October 4, 2025)
Intramuscular cerebrolysin 2.5 ml every other day, in the morning.
Intramuscular piracetam 500 mg. every other day in the morning.
Oral baclofen 10 mg 3 times daily.
Oral diazepam 2 mg at 9 pm.
Oral citicoline 100 mg daily.
Royal jelly capsule (Nutritional support) twice daily.
Collagen oral solution (Nutritional support) 3 ml daily.
Second week
First week therapies were continued.
Oral piracetam was added, 400 mg every other day in the morning, on the days not receiving Intramuscular piracetam.
Third week
Intramuscular cerebrolysin 2.5 ml daily in the morning.
Oral baclofen 10 mg 3 times daily.
Oral piracetam 400 mg daily.
Oral melatonin 5 mg at 9 pm.
Royal jelly capsule (Nutritional support) twice daily.
Collagen oral solution (Nutritional support) 3 ml in the morning and 2 ml at 5 pm.
Fourth week
Intramuscular cerebrolysin 2.5 ml every other day in the morning.
Oral baclofen 10 mg 3 times daily.
Oral piracetam 400 mg daily.
Oral melatonin 5 mg at 9 pm.
Oral magnesium glycinate 100 mg daily.
Royal jelly capsule (Nutritional support) twice daily.
Collagen oral solution (Nutritional support) 3 ml in the morning and 2 ml at 5 pm.
Hearing aid [High-Power pediatric Behind-the-Ear (BTE)] was recommended.
Outcomes
Improvement was obvious as early as October 18, 2025, continued through the first month of treatment. The child demonstrated:
- Improved alertness and environmental responsiveness.
- Recognized family members and smiled socially.
- Improved head control
- Reduced spasticity in all limbs
- For the first time, he was able to chew solid food
DISCUSSION
Kernicterus is generally considered a preventable condition that has become increasingly rare in many geographic areas in the world. It is associated with chronic metal and neurological dysfunction resulting from bilirubin-induced brain damage early during life, mostly in the basal ganglia [5].
Kernicterus is most commonly associated with dyskinetic/choreoathetoid cerebral palsy or ataxic cerebral palsy, and sensorineural hearing loss. The pathognomonic MRI finding is injury to the globus pallidus and subthalamic nucleus [1-5,9].
In this case, although globus pallidus abnormalities on MRI and hearing loss were consistent with kernicterus, the clinical phenotype was dominantly spastic, not dyskinetic. Moreover, MRI showed corpus callosum thinning and cerebral atrophy findings not typical of kernicterus but more commonly associated with spastic cerebral palsy, particularly in a quadriplegic distribution [1-5,11-13,14].
The absence of birth asphyxia suggests that the cortical and white matter injury could either be part of an unrecognized multifactorial insult, or that bilirubin toxicity extended beyond traditional deep gray matter structures in this patient.
This presentation may represent an atypical or mixed phenotype:
- Basal ganglia injury and hearing loss = classic kernicterus
- Cerebral atrophy and spasticity = white matter involvement or cortical injury
While kernicterus has a well-described neuroanatomical predilection, emerging reports suggest variability in susceptibility and clinical outcomes. This case supports that the spectrum of bilirubin encephalopathy may be broader than previously thought.
The child’s marked functional improvement after neurorestorative therapy (including Cerebrolysin, Piracetam, and Citicoline) suggests potential neuroplasticity even in severe cases.
CONCLUSION
This case illustrates a rare presentation of predominantly spastic cerebral palsy with sensorineural hearing loss following kernicterus. MRI findings of brain atrophy and corpus callosum thinning suggest cortical and white matter involvement, not typically associated with classic bilirubin encephalopathy.
In the absence of perinatal asphyxia, this case raises important questions about the extent and variability of bilirubin-induced brain injury and the potential for atypical cerebral palsy phenotypes. Multimodal neurorestorative therapy may offer meaningful improvements even years after the initial insult.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST
None.
REFERENCES
- AL-Mosawi AJ. (2018). A novel therapeutic approach for kernicterus. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-98425-1.
- Al-Mosawi AJ. (2019). The novel use of cerebrolysin and citicoline in the treatment of kernicterus. On J Neur & Br Disord. 3(1):208-212.
- Al-Mosawi AJ. (2020). New Therapies for the treatment of ataxic cerebral palsy caused by kernicterus. EC Clinical and Medical Case Reports. 3(4):26-31.
- Al-Mosawi AJ. (2021). The early treatment of a boy from Virginia with ataxic cerebral palsy. J Pediatrics and Child Health Issues. 2(4):1-5.
- Al-Mosawi AJ. (2021). Kernicterus: The continuing occurrence of a preventable chronic disabling neurologic condition. J Clin Images Med Case Rep. 2(1):1-4.
- Al-Mosawi AJ. (2019). The pattern of mental retardation in Iraqi children.1st ed., Saarbrücken; LAP Lambert Academic Publishing. ISBN: 978-613-9-47350-2.
- Al-Mosawi AJ. (2019). The etiology of mental retardation in Iraqi children. SunKrist Journal of Neonatology and Pediatrics. 1(1):1-9.
- Barnett RN, Ryder CF. (1950). Deafness and kernicterus. AMA Arch Otolaryngol. 52(5):771-772.
- Al-Mosawi AJ. (2019). The pattern of cerebral palsy in Iraqi children. MedLife Clinics. 1(1):1-9.
- Al-Mosawi AJ. (2019). New therapies for the treatment of spastic cerebral palsy. Medical Journal of Clinical Trials & Case Studies. 3(2):1-9.
- Al-Mosawi AJ. (2020). Cerebral Palsy: A Unique Illustrated Experience. SunKrist Neurology, Neurosurgery and Stroke Journal. 2(1):1-13.
- Al-Mosawi AJ. (2022). A Girl from Qatar with Post-Infantile Acquired Cerebral Palsy Caused By Submersion Injury: A Rare Etiology and a Therapeutic Challenge. Clinical Research and Clinical Trials. 5(1):1-4.
- Al-Mosawi AJ. (2020). The Treatment of a Child with Birth Asphyxia Induced Brain Atrophy, Adrenal Hemorrhage, and Bi-lateral Hyperoxaluric Nephrocalcinosis: A Challenging Case and a Unique Experience. Open Access Journal of Biogeneric Science and Research. 2(2):1-6.
- Al-Mosawi AJ. (2021). Brain Imaging Abnormalities in Cerebral Palsy. Journal of Clinical Research in Radiology. 4(1):11-15.