Previous Issues Volume 1, Issue 4 - 2016
Endoscopic Hemoclipping of Upper Gastrointestinal Bleeding Secondary to Intramural Gastric Hematoma Following Endoscopic Mucosal Resection. Two Case Reports and Review of the Literature
Lei Shi1, Fu-Jian Liu1
1Department of Gastroenterology, Eighth Affiliated Hospital of Guangxi Medical University, Guigang 537100, Guangxi Zhuang Autonomous Region, China.
Corresponding Author: Lei Shi, Department of Gastroenterology, Eighth Affiliated Hospital of Guangxi Medical University, Guigang 537100, Guangxi Zhuang Autonomous Region, China, Tel: +86 775 4200028; E-Mail: [email protected]
Received Date: 29 Sep 2016 Accepted Date: 19 Oct 2016 Published Date: 21 Oct 2016
Copyright © 2016 Shi L
Citation: Lei Shi and Fu-Jian L. (2016). Endoscopic Hemoclipping of Upper Gastrointestinal Bleeding Secondary to Intramural Gastric Hematoma Following Endoscopic Mucosal Resection. Two Case Reports and Review of the Literature. Mathews J Case Rep 1(4): 017.
ABSTRACT
Intramural hematoma of the gastrointestinal tract after endoscopic intervention is a rare phenomenon in clinical practice, and it is extremely rare in the stomach. Only a few cases have been reported in this location to date. Although the annual incidence of upper gastrointestinal bleedinghas been increasing, bleeding related to a gastric intramural hematoma as a complication of endoscopic therapy is quite rare. We describe two cases of gastric intramural hematoma caused by endoscopic mucosal resection (EMR) and our experiences with successful endoscopic hemoclipping followed by conservative care to avoid surgery for the severe bleeding. The current cases involved two women who presented with abdominal pain. The patients underwent upper gastrointestinal endoscopy, which revealed polyps 6 mm in diameter in the antrum of the stomach. These lesions were removed by EMR. Soon after EMR, the patients experienced upper gastrointestinal bleeding. Panendoscopic examination showed a large intramural hematoma extending from the lower body to the prepyloric antrum with blood oozing from the original lesion. Hemostasis was successfully performed with endoscopic hemoclips, and additional surgery was avoided.
KEYWORDS
Gastrointestinal Bleeding; Gastric Polyp; Gastric Intramural Hematoma; Endoscopic Mucosal Resection; Complication.
INTRODUCTION
Gastric intramural hematomaafter endoscopic therapyis an uncommon and extremely rare disorder, with few reports published in the literature. A MEDLINE search of the Englishlanguage medical literature concerning intramural gastric hematoma following endoscopic therapy revealed only six cases (Table 1). Here, we present two cases of gastric intramural hematoma caused by endoscopic mucosal resection (EMR) and describe our experience of successful endoscopic hemoclipping followed by conservative care for the severe bleeding with gastric intramural hematoma to avoid surgery.
CASE PRESENTATION
Patient 1 was a 48-year-old woman who visited our hospital with a complaint of chronic abdominal pain distention that had lasted for 2 months. No associated symptoms were identified. On examination, there was tenderness on palpation of the upper abdominal region and no palpable mass was present. There were no signs of peritonitis or chronic liver disease. She had no significant medical history and was not receiving anticoagulant therapy. Complete blood count, liver, and renal function tests were normal. We suspect a possible diagnosis of peptic ulcer, based on her symptoms. For diagnostic purposes an endoscopy of the upper gastrointestinal tract was performed, which revealed a flat polyp with a diameter of 6 mm in the greater curvature of the antrum of the stomach (Figure 1A). The differential diagnoses included an gastric neoplasia, likely a gastric leiomyoma or gastric stromal tumor. Endoscopic ultrasonography revealed that the lesion was located in the mucosal layer. On completion of the upper endoscopy and endoscopic ultrasonography examination, the working diagnosis was a polyp in the stomach. Following discussion with the patient, EMR was performed. We injected 3 mL of saline solution into the submucosa using a 21-G injection needle (NET2522-C4, ENDO-FLEX, Voerde, Germany) to raise the lesion (Figure 1B).
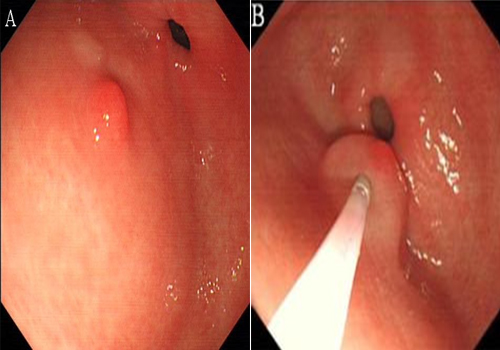
Figure 1: A: An upper gastrointestinal endoscopic finding reveal a flat polyp with a diameter of 6 mm in the greater curvature of the antrum of the stomach. B: After injection of 3 mL of saline, the whole nidus of the polyp was lifted satisfactorily.
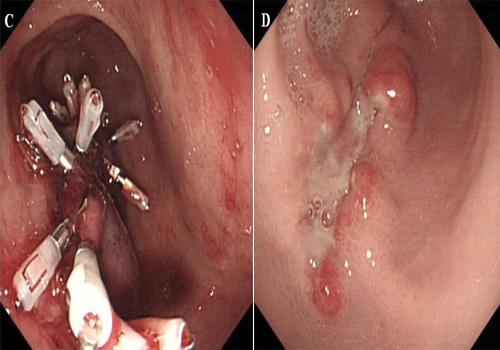
Thepolyp was completely removed by high-frequency electrocoagulation, and a white wound was observed. Four hours after EMR, the patient experienced severe bleeding and abdominal pain. The patient's hemoglobin level decreased considerably, from 12.8 g/dL to 6.7 g/dL. She underwent transfusion with 6 units of packed red blood cells to correct the anemia. Urgent endoscopy was performed, which revealed a large intramural hematoma extending from the lower body to the prepyloric antrum with blood oozing from the area of the injection site, causing almost complete obstruction of the gastric out-let (Figure 1C). Endoscopic hemoclipping was successfully performed when streaming of gastric intramural hematoma was found on endoscopic examination (Figure 1D).
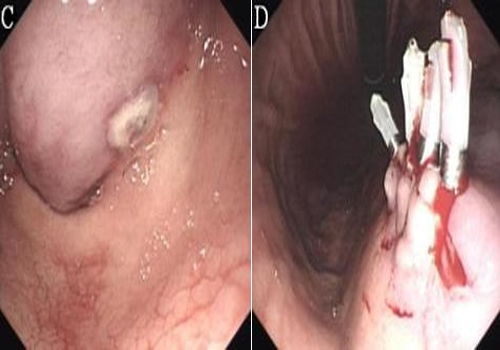
C: Endoscopic appearance 4 h later showing a large intramural hematoma extending from the lower body to the prepyloric antrum with a blood oozing from the original lesion that was causing almost complete obstruction. D:Endoscopic hemoclipping was successfully performed when streaming of gastric intramural hematoma was found on endoscopic examination.
The bleeding was completely controlled. The patient was managed conservatively with nutritional support, a proton pump inhibitor, and intravenous antibiotics. A follow-up endoscopy after 7 days revealed that the previously large hematoma was found to be smaller and had become ulcerated (Figure 1E). The gastroscope was able to pass through the stricture. The polyp obtained measured 6 mmx6 mm based on pathology. Histological examination of the polyp showed that it was an adenoma. Another endoscopic examination2 months later showed complete resolution of the hematomas (Figure 1F).
E: Follow-up endoscopy 7 days later revealed that the previously large hematoma was found to be smaller and had become ulcerated. F: Followup endoscopy 2 months later showed complete resolution of the hematoma.
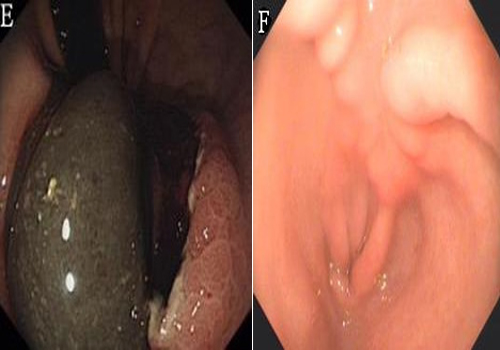
Patient 2 was a 44-year-old woman who was referred to an outside hospital because of abdominal pain of 5 days' duration. She denied a history of local trauma or coagulopathy. Like the first patient,endoscopy was also performed. The upper endoscopy showed a 6 mmx6 mm polypoid protrusive lesion in the stomach antrum (Figure 2A), and EMR of the polyp was performed. Histological examination of the gastric lesion showed it was a hyperplastic polyp. Three hours after EMR, the patient experienced bleeding and sudden epigastric pain. The patient was transferred to our hospital for further evaluation and treatment. Following discussion with the patient, endoscopy of the upper gastrointestinal tract was performed, revealing a large intramural hematoma in the anterior wall of the antrum of the stomach (Figure 2B).
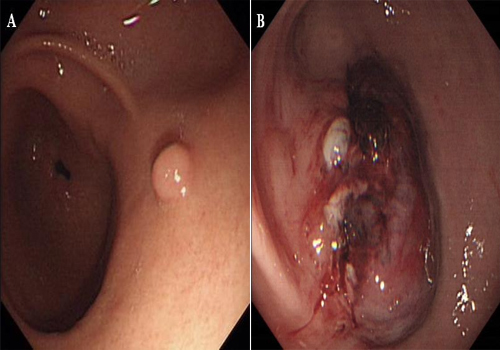
Figure 2: A: Endoscopic examination revealed a 5-mm polyp in the posterior wall of the stomach. B: Endoscopy showed a large gastric intramural hematoma in the area of the injection site.
Endoscopic hemoclipping was performed when streaming of gastric intramural hematoma was found on endoscopic examination (Figure 2C). The bleeding was completely controlled. Another endoscopy 7 days later showed complete resolution of the hematomas (Figure 2D).
C: Endoscopic hemoclipping was performed when streaming of gastric intramural hematoma was found on. D:Endoscopic view of the gastric ulcer at the original lesion 7?lK MJNBVCC days after endoscopic intervention.
DISCUSSION
Intramural hematoma of the gastrointestinal tract is a rare phenomenon in clinical practice. Most affected patients are white men who are about 60 years of age. Such hematomas been reported to occur in the duodenum, followed by the small and large intestines. The identifiable predisposing causes of intramural hematoma include: coagulopathy, trauma, peptic ulcer disease, endoscopic therapy, or spontaneous hematoma [1-4]. Gastric intramural hematoma after endoscopic therapy is an extremely rare disorder, with few reports published in the literature. A review of the English literature revealed only six published cases (Table 1). To the best of our knowledge, this report describes the first case of a life-threatening gastric intramural hemorrhage with gastric outlet obstruction caused by EMR that was managed successfully with endoscopic hemoclipping. The specific cause and development of gastric intramural hematoma are not known, but the pathogenesis in these cases was supposed to have been due to trauma to the blood vessels during the submucosal injection, especially to gastrointestinal thickpedunculatedpolyps, which always have thick nutrient blood.
Table 1: Clinical presentation and management of gastric intramural hematoma after endoscopic therapy in previously published case reports.
| No | First author | Age (yr) | Sex | Underlying disease | Endoscopic intervention | Treatment |
|---|---|---|---|---|---|---|
| 1 | Yang [5] | 72 | Female | Gastric subepithelial tumor | ESD | Conservative |
| 2 | Sadio [6] | 76 | Male | Oval ulcer | Endoscopic injection therapy | Conservative |
| 3 | Sun [7] | 33 | Male | Gastric subepithelial tumor | EMR | Surgery |
| 4 | Keum [8] | 71 | Female | Gastric flat adenoma | ESD and APC | Endoscopic incision and drainage |
| 5 | Itaba [9] | 75 | Male | Pancreatic disease | EUS-FNAB | Conservative |
| 6 | Shi [10] | 66 | Male | Bleeding anastomotic ulcer | Endoscopic injection therapy | Conservative |
ESD: Endoscopic submucosal dissection; EMR: Endoscopic mucosal resection; APC: Argon plasma coagulation; EUS-FNAB: Endoscopic ultrasoundguided fine-needle biopsy.
Endoscopy is the key for diagnosis, and intramural hematomas appear as bulging, dark-reddish submucosal masses. The spectrum of clinical symptoms at presentation is wide, including abdominal pain, emesis, and gastrointestinal tract hemorrhage. The standard techniques for endoscopic control of bleedingafter therapeutic endoscopy are not established. The management of gastric intramural hematomas depends on the clinical situation, but conservative management, including fasting, nutritional support, and treatment with a proton pump inhibitor, is typically recommended as the initial management strategy; surgical intervention is required if medical treatment fails or in cases of severebleeding [11]. There has been only one reported case of gastric intramural hematoma that required surgical treatment [5]. In that case, a 33-yearold man underwent EMR to remove a subepithelial tumor in the antrum, and he was treated surgically to evacuate the hematoma. One case required endoscopic treatment with adrenaline injection [8]. In that case, endoscopy showed an oval ulcer on the posterior wall of the gastric antrum, with oozing bleeding. Hemostasis was achieved by endoscopic injection therapy. The patient was also treated conservatively and recovered. The remaining four cases were managed conservatively, and they recovered [7-10]. Similar to previous reports, in our cases, the diagnosis was confirmed by endoscopy, and the patients were treated with endoscopic hemoclipping followed by conservative care for the bleeding to avoid additional surgery. Early diagnosis is crucial because most patients can be treated non-surgically with good outcomes. Our patients did not undergo surgical intervention because they responded well to endoscopic treatment. These patients recovered fully with no recurrence during 2 months of follow-up. With the recent widespread availability of EMR, it has become common clinical practice to resect gastrointestinal polyps. Even in expert hands, there can be serious complications when performing EMR. The most frequent complications are perforation, bleeding, stenosis, and air embolism[12]. Gastric intramural hematoma is an extremely rare complication of EMR. We present these findings to help physicians recognize this complication because better understanding of these risk factors may help to avoid more invasive procedures in the future. Although the effectiveness of endoscopic hemoclipping for gastric intramural hematoma has not been proved because gastric intramural hematoma is rare, we believe that it is technically feasible and may be considered as the procedure of choice for severe bleeding with gastric intramural hematomain order to avoid surgery. We also recommend endoscopic hemoclip application at the initial resection to prevent an acute bleed.
REFERENCES
- Chu YY, Sung KF, Ng SC, Cheng HT, et al. (2010). Achalasia combined with esophageal intramural hematoma: case report and literature review. World J Gastroenterol. 16(42), 5391- 5394.
- Hameed S, McHugh K, Shah N and Arthurs OJ. (2014). Duodenal haematoma following endoscopy as a marker of coagulopathy. Pediatr Radiol. 44(4), 392-397.
- Tong M, Hung WK, Law S, Wong KH, et al. (2006). Esophageal hematoma. Dis Esophagus. 19(3), 200-202.
- Eichele DD, Ross M, Tang P, Hutchins GF, et al. (2013). Spontaneous intramural duodenal hematoma in type 2B von Willebrand disease.World J Gastroenterol. 19(41), 7205-7208.
- Shi L, Liu FJ, Jia QH, Guang H, et al. (2014). Intramural hematoma with gastric outlet obstruction: a rare complication of endoscopic injection therapy for bleeding anastomotic ulcer. Endoscopy. 46(Suppl 1). E254-255.
- Dhawan V, Mohamed A and Fedorak RN. (2009). Gastric intramural hematoma: a case report and literature review. Can J Gastroenterol. 23(1), 19-22.
- Yang CW and Yen HH. (2011). Large gastric intramural hematoma: unusual complication of endoscopic submucosal dissection. Endoscopy. 43(Suppl 2), E240.
- Sadio A, Peixoto P, Cancela E, Castanheira A, et al. (2011). Intramural hematoma:rare complication of endoscopic.Endoscopy. 43(Suppl 2), E141-142.
- Sun P, Tan SY and Liao GH. (2012). Gastric intramural hematoma accompanied by severe pigastric pain and hematemesis after endoscopic mucosal resection. World J Gastroenterol. 18(47), 7127-7130.
- Keum B, Chun HJ, Seo YS, Kim YS, et al, (2012). RyuHS.Gastric intramural hematoma caused by argon plasma coagulation: treated with endoscopic incision and drainage (with videos). GastrointestEndosc. 75(4), 918-919.
- Itaba S, Kaku T, Minoda Y, Murao H, et al. (2014). Gastric intramural hematoma caused by endoscopic ultrasound-guided fine-needle biopsy. Endoscopy. 46(Suppl 1), E666.
- Ahn JY, Jung HY, Choi KD, Choi JY, et al. (2011). Endoscopic and oncologic outcomes after endoscopic resection for early gastric cancer: 1370 cases of absolute and extended indications. Gastrointest Endosc. 74(3), 485-493.