Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2023
Effusive Non-Tuberculosis Mycobacterial and Fungal Acute Pericarditis in Post COVID Patient: A Case Report
Omid Reza Amini1, Azade Sezavar Seiedi2, Abbasi Mohamad3, Somaye Farokhnejad4,*
1Cardiologist, Atherosclerosis Prevention Research Center AND School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
2Department of Cardiology, Ghaem Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
3Heart surgeon, Mashad University of Medical Sciences, Tehran, Iran
4Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*Corresponding Author: Somaye Farokhnejad, MD, Cardiovascular Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Phone: +989122124921; E-mail: [email protected].
Received Date: April 13, 2023
Published Date: April 24, 2023
Citation: Farokhnejad S, et al. (2023). Effusive Non-Tuberculosis Mycobacterial and Fungal Acute Pericarditis in Post COVID Patient: A Case Report. Mathews J Cardiol. 7(1):27.
Copyrights: Farokhnejad S, et al. © (2023).
ABSTRACT
Purulent pericarditis is identified by pus in pericardial space. Pericarditis due to Candida species is very rare and is associated with severe sepsis, cardiac tamponade, and a high grade of mortality. Pericardial involvement with Mycobacterium avium complex (MAC) is unusual. We present a case of post COVID purulent mycobacterial and fungal pericarditis, which was managed both medically and surgically.
Keywords: COVID-19, Mycobacterium, Candida Albicans.
INTRODUCTION
Purulent pericarditis is identified by pus in pericardial space, rising from the spread of a neighboring bacterial infection site or by blood dissemination [1]. Pericarditis due to Candida species is very rare and is associated with severe sepsis, cardiac tamponade, and a high grade of mortality; so it should be diagnosed and treated promptly. Patients with a history of immunosuppression are impressed with this infection [2-4].
Pericardial involvement with Mycobacterium Avium complex (MAC) is unusual [5,6]. Infections caused by either of the mycobacterium avium (M. avium) and mycobacterium intracellulare (M. intracellulare) are referred as MAC [7]. MAC infections usually introduce in middle to older aged patients. Alcoholics or smoker patients and patients with underlying obstructive pulmonary disorders are more susceptible [8].
We describe a male patient with an unusual case of large purulent pericardial effusıon secondary to Candida albicans in combination with MAC infection. He had a history of COVID infection 2 weeks prior to his admission into our hospital.
CASE REPORT
A 54-year-old gentleman was admitted to our hospital with two-week shortness of breath, productive cough, positional and pleuritic chest pain and lethargy. He has been suffering from bilateral lower limbs edema during last two weeks and had no evaluation for it.
The patient was in semi sitting position and he was obtaining oxygen by nasal canola. Following careful physical examination, blood pressure was 80/50 mmHg, the pulse rate was 140 pulses per minute and oxygen saturation was 96%. Internal jugular vein bulged. No heart murmurs were heard and the normal heart sounds were muffled. Both lower limbs had pitting edema beneath knees.
His only past medical history was admission due to COVID-19 infection 2 weeks before the index date. An obtained electrocardiogram at Emergency Department showed sinus tachycardia and mild diffuse ST elevation.
The chest X-ray (CXR) taken on the day of admission showed cardiomegaly (Figure 1).
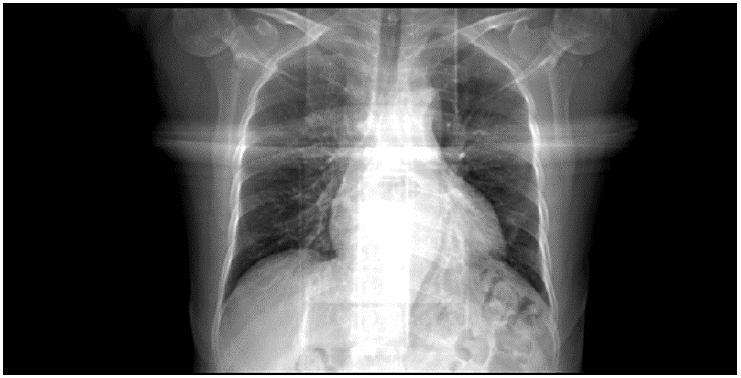
Figure 1. Chest radiography showed cardiomegaly.
Computed tomography scan (Figure 2) showed severe pericardial effusion up to 30-mm maximal thickness and basilar ground glass opacities in both lungs, with a small left plural effusion.
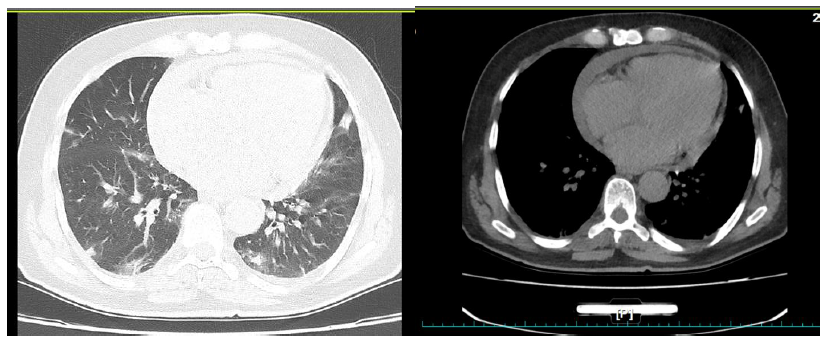
Figure 2. plural effusion with ground glass opacities (left) and pericardial effusion (right).
2-Dimentional transthoracic echocardiographic evaluation revealed normal leftventricle function and size. As predicted based on physical exam and previousimaging, a large circumferential pericardial effusion was detected with all of theechocardiographic tamponade signs. It had right atrium and right ventricle diastoliccollapse and the respiratory variation on Mitral valve was more than 10%. Therewasno evidence ofvalvulardisease.
In lab data we found a leukocytosis (white blood cell: 12000/ml) and elevated erythrocyte sedimentation rate (ESR: 52).
An ultrasound scan of the abdomen did not show hepatomegaly, splenomegaly or intra-abdominal lymphadenopathy.
Considering clinical and Echocardiographic diagnosis of tamponade, pericardial aspiration was performed under echo guidance and 1500 mL purulent fluid was aspirated in two sessions and a pigtail catheter left in place (Figure 3).

Figure 3. purulent pericardial fluid.
Pericardial fluid cytology showed 2100mg/dl amorphous protein with some lymphocytes, scattered neutrophils, few RBCs and no malignant cells.
First culture of pericardial fluid specimen showed Candida Albicans so antifungal treatment with Caspofungin, voriconazole and fluconazole was started and the patient referred for surgery.
The patient was taken to the operating room, 70 mL purulent fluid was removed and pericardial biopsy was done and sent to the pathology department.
Pericardial specimen was evaluated for mycobacterium tuberculosis (MT) by real time polymerase chain reaction (PCR). The result was negative for MT, but it was positive for Non tuberculosis mycobacterium species.
Post-surgical echocardiography revealed resolved pericardial effusion and normal ejection fraction.
Therapy was started with Isoniazid, rifampicin, clarithromycin, and ethambutol, and antifungal treatment was continued. The patient continued being asymptomatic and accordingly discharged home after a few days. The two-week follow-up showed a normal echocardiography and normal sinus rhythm in Electrocardiogram.
DISCUSSION
This was a rare and fascinating case. First, it was a co infection with MAC and candida albicans pericarditis. In addition, the MAC was found in the pericardium biopsy when the patient referred for surgery; if not, the infection may have been untreated.
Candida (most common as Candida albicans) is an unusual cause of purulent pericarditis [9,10]. Risk factors for such infection include recent thoracic or abdominal surgery, immunosuppression or malignancy [10]. In our case, given the history of covid infection, we were concerned that it could be the cause for immunosuppression.
Diagnosis of MAC disease is based on detection of MAC from blood cultures, tissue biopsies or body fluids [7]. Species recognition is performed with using of specific DNA probes [11,12], high-performance liquid chromatography or biochemical tests [7].
Therapy for Candida albicans pericarditis is based on surgical drainage and antifungal treatment. Surgical drainage is an essential part of treatment.
Amphotericin B and fluconazole were often used in reported cases [13]. Our case was treated successfully with Caspofungin, Voriconazole and Fluconazole. Antimycobacterial treatment of MAC infection needs combination therapy that should include a macrolide and ethambutol, with or without rifabutin [7]. In our patient we used the Isoniazid, rifampicin, clarithromycin, and ethambutol combination.
CONCLUSION
This is a rare case report of MAC and candida acute pericarditis in a post COVID infected host. Our patient had no evidence of recurrence of symptoms during follow up period.
ACKNOWLEDGMENTS
We thank Dr. Saieede Shafiy MD, Microbiology Manager, for her expert microbiology review.
CONFLICTS OF INTEREST
All authors have nothing to declare.
AUTHORS CONTRIBUTION
ORA: management of the patient and doing the pericardiocentesis, ASS: management of the patient, SF: writing the manuscript AM: surgical management of the patient.
ETHICS STATEMENT
Consent for publication anonymized has been obtained from the patient. As it is a case report, no approval from our ethics committee was required.
DATA AVAILABILITY STATEMENT
All data are available at the electronic file of the patient and the PACS system of our hospital.
REFERENCES
- Rabinovici R, Szewczyk D, Ovadia P, Greenspan JR, Sivalingam JJ. (1997). Candida pericarditis:clinicalprofileand treatment.Ann ThoracSurg. 63(4):1200-1204.
- Khoueiry Z, Delseny D, Leclercq F, Piot C, Roubille F. (2013). Cardiac tamponade likely due tocandida infection, in an immunocompetent patient. Ann Cardiol Angeiol (Paris). 62(2):122-123.
- Tang CP, Wang YW, Shiau YT, Lee RC, Lan KH, Chao Y. (2009). Gastropericardial fistula andCandidaalbicanspericarditis:ararecomplicationofgastricadenocarcinomatreatedwithradiationand chemotherapy.J Chin Med Assoc. 72(7):374-378.
- Dahl C, Fuursted K, Schroder H. (2007). A paediatric case of Candida pericarditis andeosophagus stricture during treatment for acute lymphatic leukaemia. ActaOncologica. 46(6):859-861.
- Choo PS, McCormack JG. (1995). Mycobacterium avium: a potentially treatable cause of pericardial effusion. J Infect. 30(1):55-58.
- Woods GL, Goldsmith JC. (1989). Fatal pericarditis due to Mycobacterium avium-Zntracellulare in acquired immunodeficiency syndrome. Chest. 95(6):1355-1357.
- Mohamed Buhary T, Gayed SL, Hafeez I. (2016). Pericardial effusion with Mycobacterium avium complex in HIV-infected patients. BMJ Case Rep. 2016:bcr2016215686.
- Marvisi M, Bassi E, Zanlari L, Civardi G. (2008). A case of mycobacterium avium complex infection in an immunocompetent man presenting with pericarditis and an HRCT pattern of lymphangitis. Eur J Intern Med. 19(4):300-302.
- Sung J, Perez IE, Feinstein A, Stein DK. (2018). A case report of purulent pericarditis caused byCandida albicans Delayed complication forty-years after esophageal surgery. Medicine. 97(28):e11286.
- Puius YA, Scully B. (2007). Treatment of Candida albicans pericarditis in a hearttransplant patient.Transpl Infect Dis. 9(3):229-232.
- Murray R, Mallal S, Heath C, French M. (2001). Cerebral mycobacterium avium infection in an HIV-infected patient following immune reconstitution and cessation of therapy for disseminated mycobacterium avium complex infection. Eur J Clin Microbiol Infect Dis. 20(3):199-201.
- Kiehn TE, Edwards FF. (1987). Rapid identification using a specific DNA probe of Mycobacteriumavium complex from patients with acquired immunodeficiency syndrome. J Clin Microbiol. 25(8):1551-1552.
- Neughebauer B, Alvarez V, Harb T, Keefer M. (2002). Constrictive pericarditis causedby candida glabrata in an immunocompetent patient: case report andreview of literature.Scand J Infect Dis. 34(8):615-619.