Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2024
Duodenal Diverticulation, a Surgical Option for Complex Duodenal-Pancreatic Injuries: Case Presentation
Héctor Alejandro Céspedes Rodríguez*, Daniel Alejandro Tello Duanes
Degree Specialist in General Surgery, Manuel Ascunce Domenech, University Hospital, Camaguey, Cuba
*Corresponding Author: Dr. Héctor Alejandro Céspedes Rodríguez, Instructor Teacher, Degree Specialist in General Surgery, Manuel Ascunce Domenech, University Hospital, Camaguey, Republic 59 between Poor and Perdomo, Postal Code: 70100, Cuba, Telephone. 58360607, ORCID: 0000-0002-3668-9888; E-mail: [email protected].
Received Date: February 22, 2024
Published Date: March 22, 2024
Citation: Rodriguez HAC, et al. (2024). Duodenal Diverticulation, a Surgical Option for Complex Duodenal-Pancreatic Injuries: Case Presentation. Mathews J Cardiol. 8(1):34.
Copyrights: Rodriguez HAC, et al. © (2024).
ABSTRACT
Introduction: Duodenal divertivulization (DD) is a procedure still performed for the treatment of complex duodenal-pancreatic injuries. Objective: To present the case of complex duodenal-pancreatic injury, where a duodenal diverticulation was performed as a way to treat said injury. Case presentation: A 48-year-old patient, who received a stab wound in the epigastrium with epiploic evisceration, was immediately operated on during the abdominal exploration, a complex pancreatic duodenal injury was noted where our surgical team decided to perform DD as a treatment for said injury. Discussion: DD as a necessary surgical option in the management of complex duodenal and pancreatic injuries, but not a technique used systematically or fundamentally for the treatment of these injuries in general. The cases must be chosen methodically, and their indications are the association of lesions of the retroduodenal or intrapancreatic common bile duct and lesions of the gastric antrum where pyloric exclusion and other surgical techniques have minimal resolution in the face of this complex trauma. Conclusions: DD leads to an irreversible alteration of food transit. However, this is a feasible bypass option in cases of high probability of complex duodenal injury of fistula and cicatricial stenosis, particularly in the context of associated gastric injury. The high mortality rate related to duodenal trauma is largely affected by the existence of associated injuries, with penetrating injuries experiencing the greatest intraoperative blood loss and shock.
Keywords: Duodenal Trauma, Pancreatic Trauma, Duodenal Diverticulation.
INTRODUCTION
Traumatic duodenal injuries are infrequent but produce a significant morbidity and mortality rate, which is why their recognition and treatment is essential [1]. Early treatment, being unlikely because its diagnosis is extremely difficult. In the diagnostic approach to duodenal trauma, knowledge of the anatomy of this organ is important, which is of special interest when classifying these injuries, as well as the mechanism that produces the injury, especially in cases of blunt abdominal trauma [2-4]. The high frequency of associated injuries should be kept in mind, since the duodenum is in close relationship with other intra and retroperitoneal organs, as well as with larger vascular structures that can imminently endanger the patient's life [3,5]. The objective of our presentation is to describe the duodenal diverticulation procedure as a useful technique in the management of complex duodenal-pancreatic trauma.
CASE PRESENTATION
A 48-year-old male, black patient, who arrives at the emergency department of our center due to receiving a penetrating stab wound to the epigastrium with epiploic evisceration, is operated on immediately during the abdominal examination, revealing a complex pancreatic duodenal injury (transfixing injury). of the first and second portion of the duodenum, with choledochal injury and of the head of the pancreas without injury to the main pancreatic duct and injury to the gastric antrum, transfixing-type injury), where our surgical team decided to perform DD as treatment for said injury due to the complexity of this and the significant number of associated injuries.
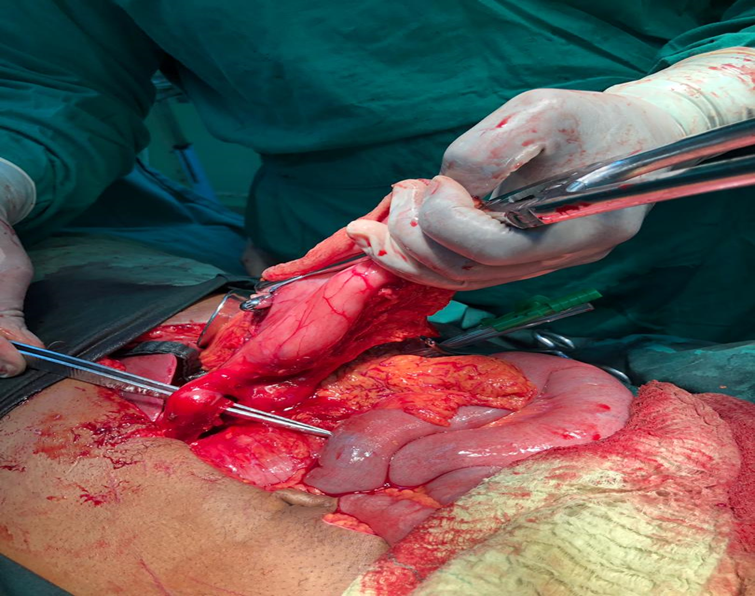
Figure 1. Note one of the transfixing-type lesions in the duodenal bulb, which corresponds to a choledochal lesion, the antrectomy almost completed
DISCUSSION
Penetrating injuries occur more frequently in urban areas, while blunt injuries predominate in rural settings. In a review of 17 series published in the literature over a period of 22 years, a total of 1,513 duodenal injuries were found, of which 1,175 (77.7%) were the result of penetrating trauma [1,3,4].
The second portion of the duodenum is the most frequently affected region after trauma. In a review where a significant number of duodenal injuries were analyzed, observing that after abdominal trauma, the second duodenal portion is the most frequently involved anatomical location with 331 injuries (33%), followed by the third and fourth portions with a total of 194 (19.4%) and 190 (19%). The least affected duodenal portion was the first with 144 (14.4%). Likewise, in 142 (14.2%) patients multiple duodenal lesions were found. In our case, there were multiple transfixing injuries of the first and second portions of the duodenum associated with injuries to the retroduodenal portion of the common bile duct, prepyloric region, and head of the pancreas, without showing disruption of the main pancreatic duct, or uncontrollable bleeding from the head of the pancreas for this reason. The duodenum is rarely injured in isolation and is very often associated with other types of injury to surrounding organs. In a review of eleven series from 1968 to 1990, a total of 1153 duodenal injuries were identified; Of these, 1,045 patients (90%) presented a total of 3,047 associated lesions. The liver was the most frequently affected organ, with a total of 517 injuries (16.9%), followed by the pancreas with 355 (11.6%), the small intestine with 351 (11.5%) and the colon with 343 (11.3%). Likewise, 299 lesions (9.8%) were detected in the large abdominal venous vessels, with the inferior vena cava lesion being the most frequent. On the other hand, arterial injuries occurred in 202 patients [2-4].
Our case was classified as type III, deciding to perform a duodenal diverticulation as a surgical option since it managed to resolve all the injuries safely. The original duodenal diverticulation was described by Berne et al. [1] in 1968. The procedure includes antrectomy and gastrojejunostomy, truncal vagotomy, debridement and duodenorrhaphy, duodenostomy, biliary Kehr tube and feeding jejunostomy. The main drawback of this technique is its great complexity, making it difficult to perform in unstable patients, but this was not the case in our case. It is a complex and time-consuming procedure, which is why it currently has practically no application for simple duodenal-pancreatic trauma [1-4]. The most serious form of duodenal injuries is when they are associated with combined pancreatic injuries, as they are associated with significant morbidity and mortality. These injuries can be addressed individually in some patients with relatively simple procedures; but in more complex cases, the risk of postoperative fistulas in both organs is very high. It is in these cases where the auxiliary procedures mentioned above have the greatest application. We consider duodenal diverticulation as a necessary surgical option in the management of complex duodenal and pancreatic injuries, but not a systematic or fundamental technique for the treatment of these injuries in general [2,3]. The cases must be chosen methodically, and their indications are the association of lesions of the retroduodenal or intrapancreatic common bile duct and lesions of the gastric antrum where pyloric exclusion and other surgical techniques have minimal resolution in the face of this complex trauma. The technique used in the surgical treatment of duodenal trauma is debatable due to the great variety of therapeutic options derived from a series of variables that must be considered in such circumstances [2,3]. The majority (70-85%) of duodenal injuries are candidates for simple procedures such as: debridement of devitalized tissue and primary repair, or resection and anastomosis plus drainage. Patients with extensive duodenal injuries may be candidates for more complex procedures, such as duodenal diverticulization, pylorus exclusion, or pancreaticoduodenectomy [1,2,4].
Between hemodynamically and metabolically stable patients or those who have achieved stability after resuscitation and those who are unstable is crucial. For those who do not recover physiological integrity, the surgical procedure of choice is the one that limits contamination of the cavity, even if it is not the definitive procedure. Resections and reconstructions that take longer times are prohibited in patients who are hypovolemic, acidotic, hypothermic, or have coagulopathy. The surgeon's instinct is to treat each injury with the best surgical technique, however, in critically ill patients, brevity is essential and physiology takes precedence over anatomy. For the rest of the patients, it is advisable to opt for a therapeutic option with definitive resolution [4-6].
Pyloric exclusion consists of suturing the duodenal lesion, closing the pylorus with absorbable thread, through gastrostomy, followed by gastrojejunostomy at the gastrostomy site, without truncal vagotomy, without gastrectomy, and without biliary bypass. This diverts gastric flow away from the duodenum for several weeks while the duodeno-pancreatic injuries heal. The pylorus is eventually opened (about 1 to 2 months later) and the gastrojejunostomy is functionally closed. In pancreaticoduodenectomy – Whipple surgery – the distal stomach, the head of the pancreas and the entire duodenum, initial portion of the jejunum, gallbladder, common bile duct and head of the pancreas are resected. In very extensive lesions of the proximal duodenum and the head of the pancreas, the destruction of the ampulla, the pancreatic duct or the bile duct can prevent reconstruction, requiring this approach. However, due to the magnitude of the surgery, this is an exceptional procedure in trauma [7,8].
Proposed by Benne in 1968, after performing it in 16 patients, duodenal diverticulation consisted of primary closure of duodenal lesions, antrectomy, termino-lateral gastrojejunostomy, and lateral tube duodenostomy. In the case of duodenopancreatic injuries near the ampulla of Vater or the extrapancreatic portion of the common bile duct, the orientation was to drain the bile duct. Vagotomy was recommended since it decreases the enzymes rich in pancreatic juice, and can reduce the possibility of erosive gastritis in the immediate postoperative period, and can prevent the appearance of gastric ulcer [2,3,5,7]. Subsequently, in 1974, Benne et al. [1] published 34 additional cases of duodenal diverticulation with a 16% total mortality. For all of the above, we consider and despite the fact that new modifications of this surgical procedure are described, which is a technique to be taken into account in the management of complex duodenopancreatic trauma, where the association with other organs such as the bile duct, stomach and jejunum suggest that it is, quickly, always taking into account the hemodynamic aspect of the patient in question, in order to overcome its complexity and mortality associated with it, reduce the figures in each patient and achieve what every surgeon wants total success of his surgical procedure [9].
CONCLUSIONS
Duodenal diverticulation leads to an irreversible alteration of alimentary transit. However, this is a feasible bypass option in cases of high probability of complex duodenal injury of fistula and cicatricial stenosis, particularly in the context of associated gastric injury. The high mortality rate related to duodenal trauma is largely affected by the existence of associated injuries, with penetrating injuries experiencing the greatest intraoperative blood loss and shock.
AUTHORS' CONTRIBUTIONS
Héctor Alejandro Céspedes Rodríguez: Search of the information and conformation of the document.
Daniel Alejandro Tello Duanes: Conformation of the document.
ACKNOWLEDGEMENTS
None.
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- Berne CJ, Donovan AJ, White EJ, Yellin AE. (1974). Duodenal "diverticulization" for duodenal and pancreatic injury. Am J Surg. 127(5):503-537.
- da Costa Ferreira CP, Lima NS, Mortati MCG, Ribeiro MA, Taha MIA, Perlingeiro JAG, et al. (2020). Duodenal diverticulization as treatment of complex duodeno-pancreatic lesions: Case report. Int J Surg Case Rep. 66:298-303.
- Cruz RJ Jr, Vincenzi R. (2010). Modified duodenal diverticulization technique for the management of duodenal fistulas. Am J Surg. 199(2):e29-e33.
- Mungazi SG, Mbanje C, Chihaka O, Madziva N. (2017). Combined pancreatic and duodenal transection injury: A case report. Int J Surg Case Rep. 39:285-287.
- Coccolini F, Kobayashi L, Kluger Y, Moore EE, Ansaloni L, Biffl W, et al. (2019). Duodeno-pancreatic and extrahepatic biliary tree trauma: WSES-AAST guidelines. World J Emerg Surg. 14:56.
- Rodríguez-García JA, Ponce-Escobedo AN, Pérez-Salazar DA, Sepúlveda-Benavides CA, Uvalle-Villagómez RA, Muñoz-Maldonado GE. (2019). Duodenal injury in blunt abdominal trauma. Case report and literature review. Cir Cir. 87(S1):53-57.
- Ordoñez CA, Parra MW, Millán M, Caicedo Y, Padilla N, García A, et al. (2021). Damage control in penetrating duodenal trauma: less is better - the sequel. Colomb Med (Cali). 52(2):e4104509.
- Schroeppel TJ, Saleem K, Sharpe JP, Magnotti LJ, Weinberg JA, Fischer PE, et al. (2016). Penetrating duodenal trauma: A 19-year experience. J Trauma Acute Care Surg. 80(3):461-465.
- Pesce A, Fabbri N, Tilli M, Bertasi M, Feo CV. (2022). The Berne-Donovan technique for diverticulization of a severe lateral non-traumatic duodenal fistula. Ann Ital Chir. 92:344-348.