Previous Issues Volume 1, Issue 3 - 2016
Cross Fused Renal Ectopia with Uretero-Pelvic Junction Obstruction in Upper Moiety and Renal Pelvis Stones in the Lower Moiety
Jamshid Sadiqi1, Najibullah Rasouly1
1Radiology department, French Medical Institute for Children (FMIC), Kabul, Afghanistan.
Corresponding Author: Jamshid Sadiqi, Radiology department, French Medical Institute for Children (FMIC), Kabul, Afghanistan, Tel: +93 20 250 0522; E-Mail: [email protected]
Received Date: 30 Jul 2016 Accepted Date: 16 Aug 2016 Published Date: 19 Aug 2016
Copyright © 2016 Sadiqi J
Citation: Sadiqi J and Rasouly N. (2016). Cross Fused Renal Ectopia with Uretero-Pelvic Junction Obstruction in Upper Moiety and Renal Pelvis Stones in the Lower Moiety. Mathews J Case Rep 1(3): 014.
INTRODUCTION
Cross fused renal ectopia (CFRE) is a rare congenital anomaly which is characterized by crossing one of the kidneys to the opposite side of its ureter insertion and fusing with the contralateral kidney. CFRE is the second common fusion anomaly after horse shoe kidney with the incidence rate of 1/1000 to 1/2000 of births. The male to female ratio is about 2-3 per 1 [1-2]. The fusion anomalies of the kidney for the first time was classified by Wilmer on 1938 but later on 1957 McDonald and McClellan modified the existed classification into crossed ectopia with fusion and without fusion and Solitary as well as bilateral crossed ectopia [3]. The mentioned abnormalities are clinically significant as about half of the patients may represent with complications such as; hydronephrosis, infections, uretero-pelvic junction obstruction and nephrolithiasis [4].
CASE REPORT
A 14 years old boy with history of left flank pain was referred to radiology department of French Medical Institute for Children (FMIC) for Intravenous urography (IVU) examination. The KUB plain image showed multiple radio-opaque stones at the region of left flank [Figure. 1] while after IV injection of non-ionic contrast agent the nephrogram image demonstrated a large kidney in the left side with no evidence of nephrogram in the right side [Figure. 2]. 30 minutes post contrast image displayed significant hydronephrosis of an upper moiety with evidence of abrupt cutoff at the region of renal pelvis and moderate hydronephrosis of the a lower moiety kidney due to stones in the renal pelvis [Figure. 3]. Only single ureter which showed passage of contrast into the urinary bladder was detected in 90 minutes post contrast image [Figure. 4]. After the mentioned imaging findings the diagnosis of a right side crossed fused renal ectopia with uretero-pelvic junction obstruction of upper kidney (normal position left kidney) and renal pelvis stones of lower kidney(right fused ectopic kidney) was performed. Then patient was introduced for surgery department for nephrolithotomy as well as treatment of upper moiety uretero-pelvic junction obstruction. The lithotomy with junction-junction (JJ) stent procedure was done. Post operation plain image demonstrated no evidence of renal stones with a normal JJ stent location into the upper moiety kidney and urinary bladder [Figure. 5]. Also post operated ultrasound images showed no evidence of stones and hydronephrosis with a normal JJ stent position [Figure. 6, 7].

Figure 1: Multiple radio-opaque Stones in the left flank region.

Figures 2: Nephrogram shows a large kidney in the left side of abdomen.
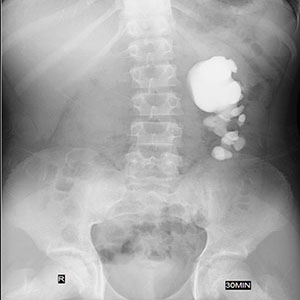
Figures 3: Significant hydronephrosis in the upper moiety with abrupt cut off at the uretero-pelvic junction and moderate hydronephrosis in the lower moiety due to renal pelvis stones.

Figure 4: Single ureter with normal caliber is seen in the left side showing passage of contrast into the urinary bladder.

Figures 5: No evidence of renal stones after operation with a normal JJ stent position into the upper moiety kidney and urinary bladder.

Figures 6: Post operation ultrasound image shows fused kidneys with evidence of a notch between them and JJ stent in the upper kidney with no evidence of stone in lower kidney.

Figures 7: Post operation ultrasound shows tip of JJ stent inside the urinary bladder.
DISCUSSION
It is commonly believed that, CFRE results from abnormal migration and crossing of ureteric bud and metanephric blastoma during the 4th to 8th weeks of embryonic life [5]. Some other etiologies like abnormal location of umbilical artery that prevents normal cephalic migration, malrotated caudal end of the fetus, teratogenic and genetic factors have been also proposed [6]. The inferior CFRE is more common comparing to superior type as in inferior type the upper pole of crossed ectopic kidney is fused with the lower pole of superior normal positioned kidney [5]. The incidence of Left to right crossed ectopia is 3 times higher in comparison to right to left crossed ectopia and here we presented a right to left crossed fused ectopia [2]. Cross renal ectopia have four main categories; fused or non-fused renal ectopia, unilateral crossed ectopia with renal agenesis of the contralateral side and crossed renal ectopia bilaterally without fusion which in more than 85% of cases complete or incomplete fusion of the kidneys exist [1]. The cross fused kidneys demonstrate six different anatomical types; inferior (which is the most common type), superior (the least common one), L shaped, sigmoid, disc and lump kidneys [1]. The diagnosis of this congenital malformation can be done by various imaging modalities; intravenous urography can reveal absent kidney in one side with information about origin, course and insertion of ureters but no specific findings of fused kidneys. Ultrasonography shows an empty renal fossa in one side and fused kidneys in contralateral side with an anterior or posterior notch between both kidneys. Computed tomography can give detail information about the fused Kidneys. Regarding function of kidneys renal scintigraphy would be the best modality [7]. Although no specific treatment is required for asymptomatic cases, previous understanding of the anomaly seems necessary before any needed surgical intervention. Sometimes renal complications like nephrolithiasis; hydronephrosis, uretero-pelvic junction obstruction and infection may occur which require appropriate treatment [5]. In the present study the cross fused kidneys demonstrated evidence of uretero-pelvic junction obstruction with significant hydronephrosis in the normal positioned left kidney and multiple stones in the cross fused right kidney which resulted in moderate hydronephrosis.
REFERENCES
- Akdogan L, Oguz AK, Ergun T and Ergun I. (2015). The rarest of the rare: crossed fused renal ectopia of the superior ectopia type. Case reports in nephrology. 2015, 4.
- Bauer SB. (2002). Anomalies of the upper urinary tract. Campbells urology. 1885-1924.
- Solanki S, Bhatnagar V, Gupta AK, and Kumar R. (2013). Crossed fused renal ectopia: Challenges in diagnosis and management. Journal of Indian Association of Pediatric Surgeons. 18(1), 7.
- Abeshouse BS and Bhisitkul I. (1959). Crossed renal ectopia with and without fusion. Urologia internationalis, 9(2), 63-91.
- Solanki S, Bhatnagar V, Gupta AK and Kumar R. (2013). Crossed fused renal ectopia: Challenges in diagnosis and management. Journal of Indian Association of Pediatric Surgeons. 18(1), 7-10.
- Chang PL, Mrazek-Pugh B and Blumenfeld YJ. (2011). Prenatal diagnosis of cross-fused renal ectopia: does color Doppler and 3-dimensional sonography help?. Journal of Ultrasound in Medicine. 30(4), 578-580.
- Kaur N, Saha S, Mriglani R, Saini P, et al. (2013). Crossed fused renal ectopia with a single ureter: a rare anomaly. Saudi Journal of Kidney Diseases and Transplantation. 24(4), 773- 776.