Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
Covid-19 in a Patient with Congenital Analbuminemia and Coronary Artery Disease: A Case Report
Sana Aboulkacem1, Yessine Amri2,3,*, Aymen Tezeghdenti4, Manel Ayoub1, Refka Kaddour5, Oussama Lamine1, Chakib Mazigh1
1Biochemistry Department, Military Hospital of Tunis, Monfleury, 1008, Tunis, Tunisia
2Biochemistry Laboratory, Bechir Hamza Children’s Hospital, Bab Saadoun Square, 1007, Tunis, Tunisia
3Department of Educational Sciences, Higher Institute of Applied Studies in Humanity Le Kef, University of Jendouba, Le Kef, Tunisia.
4Immunology Department, Military Hospital of Tunis, Monfleury, 1008, Tunis, Tunisia
5Anesthesiology Department, Bechir Hamza Children’s Hospital, Bab Saadoun Square, 1007, Tunis, Tunisia
*Corresponding author: Dr. Yessine Amri, Biochemistry Laboratory, Bechir Hamza Children’s Hospital, Bab Saadoun Square, Tunis 1007, Tunisia; Tel : 00216 22888506; E-mail: [email protected]
Received Date: February 6, 2023
Publication Date: February 13, 2023
Citation: Aboulkacem S, et al. (2023). Covid-19 in a Patient with Congenital Analbuminemia and Coronary Artery Disease: A Case Report. Mathews J Case Rep. 8(2):90.
Copyright: Aboulkacem S, et al. © (2023)
ABSTRACT
Congenital analbuminemia (CAA) is a very rare autosomal recessive disorder that can be rarely associated with coronary artery disease. Our data describe the clinical features and laboratory results of a COVID patient with congenital analbuminemia (CAA) and coronary artery disease. To the best of our knowledge, it is the first case of recurrent acute coronary syndrome in a young adult with CAA. Moreover, COVID-19 has never been described among the 90 cases of CAA reported in the literature. Mild clinical manifestations observed in such CAA patients can be explained by the elevated biosynthesis of other plasma proteins, including serum globulins. Indeed, the high serum complements C3 and C4 resulted from CAA disease protect patient from the risk of intravascular coagulation and cell death during COVID-19 infection. On the other hand, the statin therapy of hypercholesterolemia which is mostly observed in CAA patient reduce the incidence of severe clinical manifestations and improve prognosis in COVID-19 patients by modulating the immune response to inflammation, improving endothelial function, inhibiting oxidative stress, and exerting direct antiviral effects.
Keywords: Albumin; Congenital Analbuminemia; Coronary artery disease; COVID-19
INTRODUCTION
Coronavirus Diseases-2019 (COVID-19), declared by WHO as a global pandemic in March 2020, was called by the multi-faceted pathology. With one year’s hindsight, clinicians are still unable to fully understand both its pathophysiological mechanisms and its clinical manifestations. Risk factors for worse clinical outcome have not been well-defined yet.
Patients with multiple disorders appeared to be more predisposed to develop severe forms of this infection. Emerging data suggest a relatively high incidence of cardiovascular disease (CVD) in patients with severe COVID-19 and CVD may be associated with a high risk of fatal outcomes due to COVID-19 [1].
Congenital analbuminemia (CAA) is a very rare autosomal recessive disorder (incidence < 1 in 1 million births) that can be rarely associated with coronary artery disease (CAD) [2,3].
In the present study, we report the first case of asymptomatic COVID-19 in a patient with CAA and coronary artery disease. To the best of our knowledge, COVID-19 infection has never been evoked among the 90 cases of CAA reported in the literature [4,5].
CASE REPORT
A 34-year-old man, born out of a non-consanguineous marriage in northern Tunisia, with congenital analbuminemia was admitted to our hospital for SARS-CoV-2 RT-PCR test because of his contact history with his mother who developed a severe form of the disease. He had been hospitalized the last year for hypercholesterolemia and coronary artery disease. The patient has not been vaccinated and did not show or develop any signs or symptoms.
Clinical examination revealed normal vital signs (temperature: 37.2°C; blood pressure 110/70 mmHg; heart rate: 84bpm), normal body mass index: (height: 184 cm; weight: 81 kg), and no fever. The patient respiratory frequency was 19, and his oxygen saturation was 97%.
A nasopharyngeal swab by real-time PCR (RT-PCR) confirmed a SARS-Cov-2 infection.
Serum protein gel agarose electrophoresis (Hydrasys 2 Scan, Sebia, France) revealed a lower area and intensity in the albumin band (10 % of the total protein levels; reference range, 53-65 %) with the increase of other serum protein fractions (Figure1).
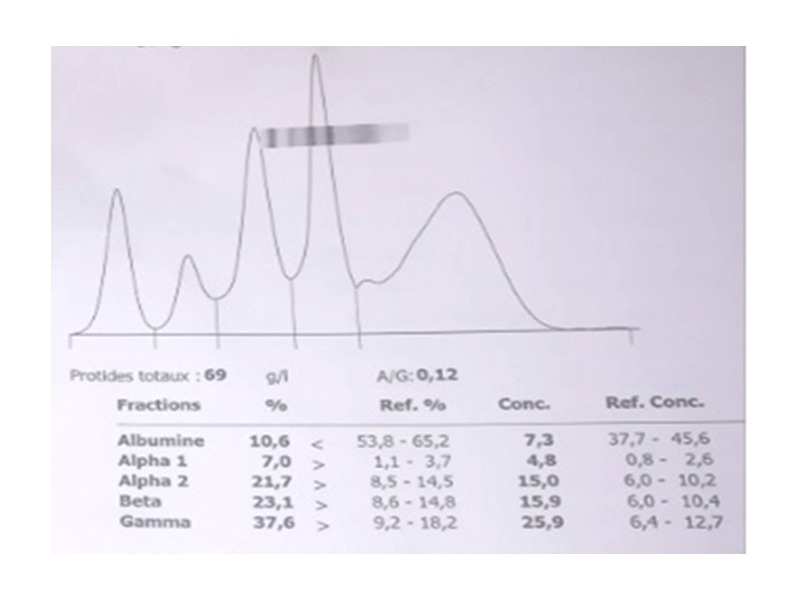
Figure 1: Serum protein electrophoresis profile of a patient with congenital analbuminemia.
Laboratory routine tests revealed high total cholesterol and LDL cholesterol level: 10 and 7.4 mmol/L, HDL cholesterol: 1.59 mmol/L, triglycerides: 2.2 mmol/L, Lipoprotein (a): 240 nmol/ L (normal range, <50 nmol/L) , Apoprotein B:2.11g/L (normal range, 0,16-1,17 g/L), blood count without abnormality, C-reactive Protein: 26.2 mg/L, fasting glucose: 5.2 mmol/L, urea: 3.1 mmol/L (normal range, 3.3-7 mmol/l), creatinine: 76 µmol/L (normal range, 53-120 μmol/L), liver enzymes: TGO: 19 IU/L and TGP : 20 IU/L (normal ranges respectively, 10-42 and 10-60 UI), Complement factor C3:2.3 g/L (reference range, 0.97-1.57 g/L), Complement factor C4: 0,96 g/L (reference range, 0.16-0,44g/L), interleukin six : 7 pg/L, Immunoglobulin G: 18.5g/L(reference range, 6.5-15g/L), Immunoglobulin A: 2.86 g/L(reference range, 0.8-3.1g/L), and Immunoglobulin M: 0.81 g/L (reference range, 0.55-3g/L).
The thrombophilia assessment showed platelet count:250000/mm3 (reference range, 150000/mm3 -400000/mm3), normal prothrombin time, normal D-dimeres level, absence of antiphospholipid antibodies, normal ranges for protein C and S, no factor V Leiden or prothrombin mutations, and normal homocysteine level.
DISCUSSION
Congenital albuminemia is a pathology that can be noisy at birth but is very often diagnosed in adulthood. Patients may show clinical signs: edema, fatigue, hypotension, and lipodystrophy.
The poverty of clinical manifestations in patients with CAA can be explained by the elevated biosynthesis of other plasma proteins by the liver, including serum globulins [6].
High serum complement C3 and C4 suggest that there was a compensatory biosynthesis by the liver and low complement system activation resulting in the moderate release of pro-inflammatory cytokines and, consequently, less risk of intravascular coagulation and cell death.
This hypothesis is consistent with a systematic review and meta-analysis, showing that the serum concentrations of complement C3 and C4 were significantly lower in COVID-19 patients with more severe disease or who died during follow-up when compared to those with milder disease or survivor status [7].
Typical biological findings are mainly hypoalbuminemia, the elevation of some plasma proteins, and hypercholesterolemia with a high concentration of LDL cholesterol as observed in our patient who was under statins before infection [6].
Due to their cholesterol–lowering activity and their pleiotropic effects, statins can reduce the incidence of severe clinical manifestations and improve prognosis in COVID-19 patients by modulating the immune response to inflammation, avoiding cytokine storm, inhibiting oxidative stress, exerting direct antiviral effects, improving endothelial function, and regulating homeostasis [8,9].
A multicenter US observational study of over 10,000 patients hospitalized for COVID-19 found that use of statins before admission was associated with a greater than 40% reduction in mortality and a greater than 25% reduction in risk of developing a severe outcome, after controlling for other medication use, comorbid conditions, hospital site and month of admission, and patient demographic characteristics [10].
ACKNOWLEDGEMENTS
We thank all the clinicians for their fruitful involvement in this work. We also thank the patients and their parents for their contribution.
RESEARCH FUNDING
None declared.
AUTHOR CONTRIBUTIONS
All Authors have contributed to the drafting and the critical revision of the article. The final version was approved by all authors.
DECLARATION OF COMPETING INTEREST
The authors declare that they have no competing financial interests or personal relationships that could affect this paper.
INFORMED CONSENT
The patient signed informed consent before blood withdrawal, after receiving all the necessary information about the research.
ETHICAL APPROVAL
This study was carried out under the principles of the Declaration of Helsinki developed by the World Medical Association and approved by the Human Ethics committee of the Military Hospital of Tunis.
REFERENCES
- Bae S, Kim SR, Kim M, Shim WJ, Park SM. (2021). Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: a systematic review and meta-analysis. Heart. 107(5):373-380.
- Demirsoy E, Sirin G, Ozker E. (2011). Coronary artery bypass surgery in a patient with analbuminemia. Tex Heart Inst J. 38(1):85-87.
- Aboulkacem S, Arem K, Ayoub M, Ba A, Raddaoui H, Hajlaoui N, et al. (2021). Congenital analbuminemia complicated by relapsing acute coronary syndrome: A case report and literature review. Ann Cardiol Angeiol (Paris). 70(4):256-258.
- Minchiotti L, Caridi G, Campagnoli M, Lugani F, Galliano M, Kragh-Hansen U. (2019). Diagnosis, Phenotype, and Molecular Genetics of Congenital Analbuminemia. Front Genet. 10:336.
- Register of analbuminemia cases. (2021). The albumin website.
- Minchiotti L, Galliano M, Caridi G, Kragh-Hansen U, Peters T Jr. (2013). Congenital analbuminaemia: molecular defects and biochemical and clinical aspects. Biochim Biophys Acta. 1830(12):5494-5502.
- Zinellu A, Mangoni AA. (2021). Serum Complement C3 and C4 and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis with Meta-Regression. Front Immunol 12:696085.
- Ganjali S, Bianconi V, Penson PE, Pirro M, Banach M, Watts GF, et al. (2020). Commentary: Statins, COVID-19, and coronary artery disease: killing two birds with one stone. Metabolism. 113:154375.
- Vuorio A, Kovanen PT. (2021). Statins as Adjuvant Therapy for COVID-19 to Calm the Stormy Immunothrombosis and Beyond. Front Pharmacol. 11:579548.
- Daniels LB, Ren J, Kumar K, Bui QM, Zhang J, Zhang X, et al. (2021). Relation of prior statin and anti-hypertensive use to severity of disease among patients hospitalized with COVID-19: Findings from the American Heart Association's COVID-19 Cardiovascular Disease Registry. PLoS One. 16(7):e0254635.