Information Links
Related Conferences
Previous Issues Volume 8, Issue 11 - 2023
Characterization of COVID-19 through Clinical Manifestation, Diagnostic Evaluation and Management: A Study from CNMCH and Basirhat
Biplab Ghosh*, Joy Mondal, Rituparna Haldar, Ayesha Abid, Debashis Santra, Dipankar Bag, Bodhan Roy, Arijit Modak, Ananda Chaulya, Rafiqul Islam Khan
Department of microbiology, Calcutta National Medical College and Hospital 32, West Bengal 700014, India
*Corresponding Author: Biplab Ghosh, Department of microbiology, Calcutta National Medical College and Hospital 32, West Bengal 700014, India; Email: [email protected]
Received Date: November 29, 2023
Publication Date: December 09, 2023
Citation: Ghosh B, et al. (2023). Characterization of COVID-19 through Clinical Manifestation, Diagnostic Evaluation and Management: A Study from CNMCH and Basirhat. Mathews J Case Rep. 8(11):136.
Copyright: Ghosh B, et al. © (2023)
ABSTRACT
Background: The outbreak of a new corona virus (SARS CoV-2) that causes severe acute respiratory syndrome is clinically named as COVID-19. The virus is major cause of concern owing to its intensity of virulence and rapid spread across the world that causes more than two million of people infected and thousands of deaths. Aim: The aim of this research was to do surveillance among comorbid patients from two distinct hospitals of West Bengal, an eastern region of India. Methods: Nasopharyngeal and oropharyngeal sample was collected from the suspected patient for the isolation of the viral RNA followed by its diagnosis by RT-QPCR method. Results: We identified that, among 500 tested samples 50 (10%) were found to be covid positive. 60% (30/50) of the positive population were Asymptomatic and rest 40% (20/50) were Symptomatic. 6.66% (2/30) of the asymptomatic population were observed to be suffering from chronic renal disease and chronic lung disease each. Variation in comorbidity was observed among the Symptomatic patient where 10% (2/20) of the population were observed to be suffering from hypertension and diabetes and 35% (7/40) had severe respiratory problem. 44% (22/50) COVID patient were immunocompromised. Of these, 36.36% (8/22) of the immunocompromised Covid positive patient were Symptomatic and rest 63.63% (14/22) were asymptomatic. Conclusion: A variation of comorbid characteristics was observed and therefore a thorough clinical surveillance should be done to restrict the spread of infection.
Keywords: SARS CoV-2, COVID-19, Viral RNA, RT-QPCR, Co-morbidity
INTRODUCTION
After the first case reports of an acute respiratory syndrome of unknown etiology in the city of Wuhan, Hubei province (December 31, 2019), Chinese authorities identified a new coronavirus (SARSCoV-2) that causes the clinical disease COVID-19. The virus outbreak spread quickly, significantly affecting all continents with more than 2 million people infected and thousands of deaths [1,2]. SARS CoV-2 by the International Committee on Taxonomy of Viruses, belongs to the genus beta-CoV [3]. Beta-CoV also comprises of the Severe Acute Respiratory Syndrome CoV (SARS-CoV), and Middle Eastern Respiratory Syndrome CoV (MERS-CoV). On February 11th, 2020, the World Health Organization (WHO) announced a new name for disease caused by SARS-CoV-2: CoV disease (COVID-19), and exactly a month later, on March 11th, 2020, it was declared as a pandemic [3,4]. Rapid characterization of SARS-CoV-2 by electron microscopy and NGS confirmed that it shared the structural features and genomic organization of other beta coronaviruses [6,7]. The virus has the ability to alter its physiological structure in response to environmental conditions. It is an enveloped virus having a size range of 60-140nm with distinctive surface spikes. Sars Cov 2 is a 29 -30 kb size positive sense single stranded RNA genome and is organised as methylcapped - 5ʹ UTR-ORF1a/b-S-ORF-3-E-M-ORF6-ORF7a/b-ORF8-N/ORF9b-ORF10-3ʹ UTR-PolyA tail [8]. The literature review study reveals that the ribosome profiling techniques in one of the earliest published genome, hCov-19/wuhan/IVDC-HB-01/2019(GISAID accession number EPI_ISL_402119) having a genome size of 29,891 bp has the presence of additional upstream and internal open reading frames(ORFs) [9]. The lack of hemagglutinin esterase gene in Sars Cov 2 genome differs it from other betacoronaviruses. Two third of the entire genome is composed of ORF1ab which encodes a large polyprotein pp1ab. The polyprotein pp1ab is cleaved into 16 non-structural proteins (Nsps) which is responsible for viral replication [8]. The structural protein found in the mature virion is encoded by S, E, M and N genes found toward the 3ʹ end of the genome [10]. The spike(S) glycoprotein binds to human angiotensin-converting enzyme (ACE2) receptor for cell entry [11]. The two subunits of spike (S) protein S1 and S2 contains a polybasic cite PRRA which enables cleavage by furin and other proteases [5]. The virus replication is enhanced by the virulence factor present in the multibasic cleavage site similar to that of multiple tissue tropism found in avian influenza A(H5N1) virus [12,13].
MATERIAL & METHODS
Sample collection and Isolation of viral RNA
A total of 500 Nasopharyngeal and oropharyngeal samples were collected in VTM Vial under cold chain from both hospitals admitted and community acquired symptomatic and asymptomatic patient. RNA for isolation procedures typically involves three general steps: cell lysis, separation of RNA from other macromolecules such as DNA, Proteins, and lipids, followed by RNA concentration [14].
RT-QPCR is used as a diagnostic tool for detecting SARS-CoV-2
PCR-based methods are considered the gold standard for viral detection. SARS-CoV-2 requires RT-PCR based approaches, by virtue of being an RNA virus. In order to enhance the sensitivity and fidelity of RT PCR assays, the strategy is to evaluate the potential of various viral genes as probe targets and compare the relative performance of each gene [15]. The various diagnostics kits used in our laboratory assay probe against the ORF1b and N region of the viral genome. Subsequently it also aimed at two novel assays nucleocapsid (N), and RNA-dependant RNA polymerase (RdRp).
RESULT
Identification and characterization of COVID positive samples
50 (10%) out of total 500 tested samples were found to be covid positive. The positive samples are further categorised on two major parameters which are Asymptomatic and Symptomatic.
Asymptomatic positive samples
60% (30/50) of the positive population were found to be Asymptomatic. Of these, 6.66% (2/30) of the asymptomatic population were observed to be suffering from chronic renal disease and chronic lung disease each. (Fig 1) was observed to be statistically significant with P value < (0.001), ***
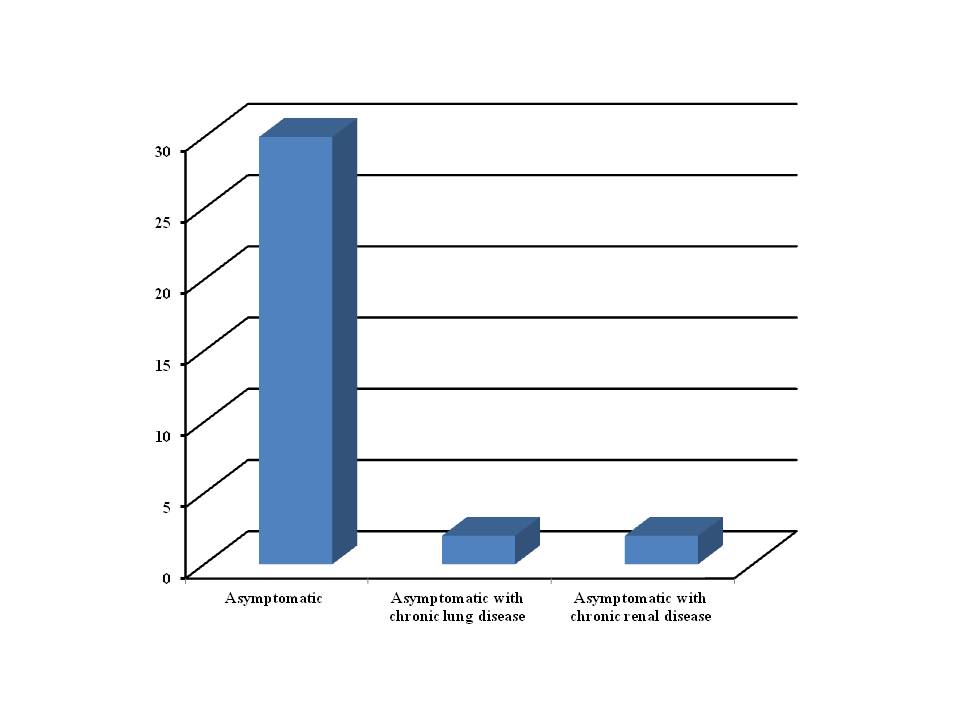
Figure 1: Characterization of asymptomatic positive samples.
Symptomatic positive samples
40% (20/50) of the positive population harboured symptomatic characteristics. Of these, 55% (11/20) of the symptomatic patient were suffering from fever at evaluation. 10% (2/20) of the population were observed fever at evaluation with hypertension, diabetes and fever at evaluation with breathlessness each. 35% (7/40) of the symptomatic patient were observed to be suffering from fever with cough and breathlessness. (Fig 2) was observed to be statistically significant with P value < (0.001), ***
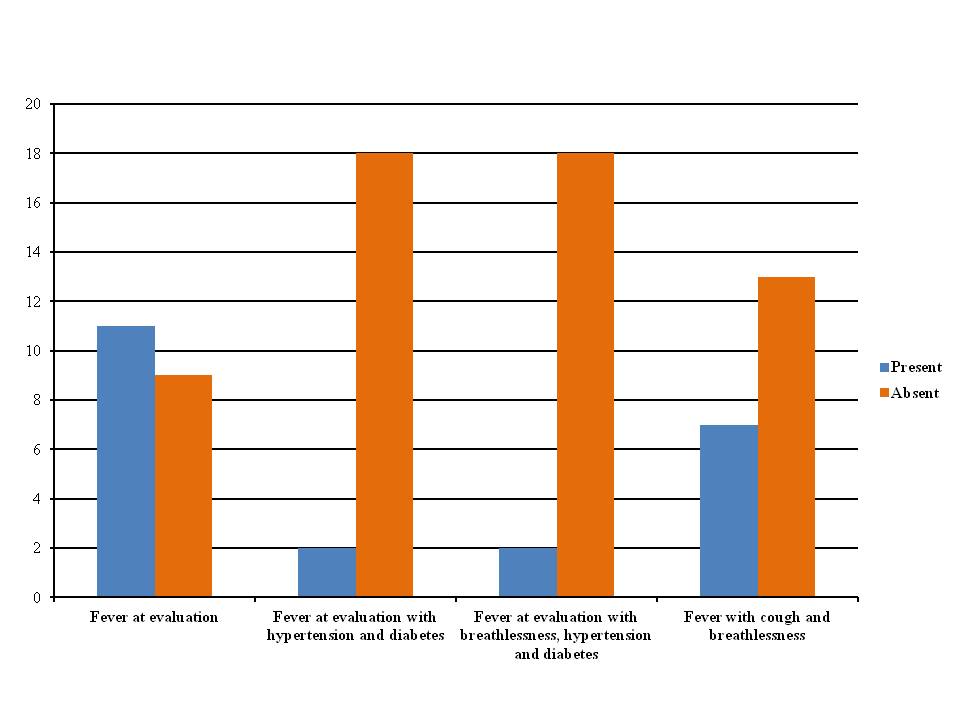
Figure 2: Characterization of Symptomatic positive samples.
Immunocompromised patient within COVID positive population
44% (22/50) of the Covid positive population were observed to be immunocompromised. Of these, 36.36% (8/22) of the immunocompromised Covid positive patient were Symptomatic and rest 63.63% (14/22) of the immunocompromised sample were harboured by asymptomatic positive population. (Fig 3) was observed to be statistically significant with P value < (0.001), ***
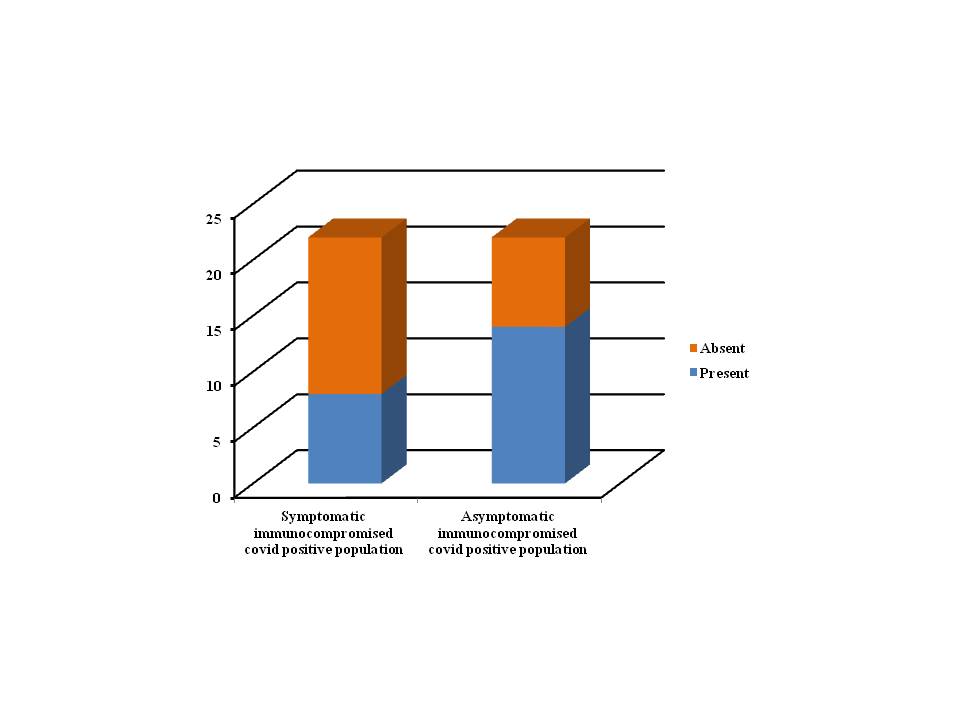
Figure 3: Characterization of Symptomatic and Asymptomatic immunocompromised sample.
DISCUSSION
This study demonstrates the prevalence of SARS CoV2 among the hospitalised and community acquired patient having symptomatic and asymptomatic features with comorbid characteristics. Prevalence of comorbidity with SARS CoV2 infection have been observed worldwide with uncontrolled spread of the virus. Comorbidity was observed within both symptomatic and asymptomatic population of our study with 6.66% and 45% respectively whereas report from other parts of India states the high rate of comorbidity where 72% of the reported cases were comorbid and 37% of the cases were without comorbid [16].
Variation in the report of comorbidity is observed throughout across the globe. In contrast to our report of 6.66% of the asymptomatic infected population suffering from chronic lung disease and chronic renal disease(3.33% each), report from Iran states that of all the comorbid cases reported ,2.02% had respiratory diseases and 0.60% had chronic kidney diseases [17].Whereas data collected from Indonesia confirms that of all the comorbid cases reported, a high percentage of infected people that is 23.08% had chronic kidney disease and a larger section of the infected population, 6.45% had chronic respiratory disease [18]. Report collected from Spain states that 3.8% of the comorbid patient had chronic renal failure [19].
Our study shows 10% of the infected symptomatic population suffering from fever with hypertension and diabetes whereas 35% of the infected symptomatic patient suffering from fevers with cough and breathlessness. Thus, in our study we found majoritarian of our infected patient were suffering from severe acute respiratory disease in contrast to other comorbid infection. Report across the globe shows distinct comorbid characteristics, study from Iran states high percentage of the comorbid patient were diabetic which constitute 3.81% followed by 1.99% hypertension and 1.25% suffering from cardiovascular diseases [17].Whereas report from Indonesia shows even higher percentage of comorbid infection with majoritarian of comorbid infected patient had hypertension 42.31% and cardiovascular disease 30.77% respectively with relatively low percentage 28.21% of comorbid diabetic patient [18]. Data collected from Spain also states high rate of comorbid infection with 28.5% of its covid infected patient suffering from hypertension and 7.7% had cardiovascular diseases followed by 13.5% comorbid infected patient were diabetic [19].
Another unique feature of our study depicts that 44% of the covid infected patient were Immunocompromised and that too the majority of which were Asymptomatic, in contrast to the report from Indonesia which states that only 3.85% of their infected population was immunocompromised [18].
CONCLUSION
A large section of COVID infected patients observed in India and across the globe, showed a wide variation of comorbid characteristics. Hence more thorough clinical studies through routine surveillance and diagnostic evaluation should be undertaken to combat the spread of infection. The administration of drugs vide accurate therapeutic index should be considered for comorbid patients to reduce mortality.
REFERENCES
- WHO. (2020). Coronavirus Disease (COVID-2019) Situation Reports.
- https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
- Ahn DG, Shin HJ, Kim MH, Lee S, Kim HS, Myoung J, et al. (2020). Current status of epidemiology, diagnosis, therapeutics vaccines for novel coronavirus disease 2019 (COVID-19). J Microbiol Biotechnol. 30:313–324.
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. (2020). Severe acute respiratory syndrome coronavirus 2 (SARSCoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 55 (3):105924.
- World Health Organization. (2020). COVID-19 Situation report - 51. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311- sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10
- Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF. (2020). The proximal origin of SARS-CoV-2. Nat Med. 26:450–452.
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. (2019). China Novel Coronavirus I, Research T. 2020. A Novel Coronavirus from patients with pneumonia in China. N Engl J Med. 382:727–733.
- Chan JF, Yuan S, Kok KH, To KK, Chu H, Yang J, et al. (2020). A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 395:514–523.
- Chan JF, Kok KH, Zhu Z, Chu H, To KK, Yuan S, et al. (2020). Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect. 9:221–236.
- Finkel Y, Mizrahi O, Nachshon A, Weingarten-Gabbay S, Morgenstern D, Yahalom-Ronen Y, et al. (2021). The coding capacity of SARS-CoV-2. Nature. 589:125–130.
- Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, et al. (2020). A new coronavirus associated with human respiratory disease in China. Nature. 579:265–269.
- Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q. (2020). Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science. 367:1444–1448.
- Boonnak K, Matsuoka Y, Wang W, Suguitan AL Jr, Chen Z, Paskel M, et al. (2012). The multibasic cleavage site of the hemagglutinin of highly pathogenic A/Vietnam/1203/2004 (H5N1) avian influenza virus acts as a virulence factor in a host-specific manner in mammals. J Virol. 86:2706–2714.
- Lau SY, Wang P, Mok BW, Zhang AJ, Chu H, Lee AC, et al. (2020 ). Attenuated SARSCoV-2 variants with deletions at the S1/S2 junction. Emerg Microbes Infect. 9:837–842.
- Wozniak A, Cerda A, Ibarra-Henríquez C, Sebastian V, Armijo G, Lamig L, et al. (2020). A simple RNA preparation method for SARS-CoV-2 detection by RT-QPCR. Sci Rep. 10:16608.
- Sreepadmanabh M, Sahu AK, Chande A. (2020). COVID-19: Advances in diagnostic tools, treatment strategies, and vaccine development. J Biosci. 45:148.
- Singh AK, Gupta R, Ghosh A, Misra A. (2020). Diabetes in COVID-19: Prevalence, pathophysiology, prognosis, and practical consideration. Diabetic and Metabolic Syndrome: Clin Res Rev. 14:303-310.
- Nikpouraghdam M, Jalali Farahani A, Alishiri G, Heydari S, Ebrahimnia M, Samadinia H,et al. (2020). Epidemiological characteristics of corona virus disease 2019(COVID-19) patients in Iran: A single Centre study. J Clin Virol. 127:104378.
- Djaharuddin I, Munawwarah S, Nurulita A, Ilyas M, Tabri NA, Lihawa N. (2021). Comorbidities and mortality in COVID-19 patients. Gac Sanit. 35(s2):s530-s532.
- Blanco JR, Cobos-Ceballos MJ, Navarro F, Sanjoaquin I, Arnaiz de Las Revillas F, Bernal E, et al. (2021). Pulmonary long term consequences of COVID-19 infections after hospital discharge. Clin Microbiol infect. 27:892-896.