Previous Issues Volume 2, Issue 1 - 2017
Caudate Lobe Cystic Echinococcosis
Mohammad Tahir Aien1, Fazel Rahman Faizi2*
1Department of Radiology, French Medical Institute for Children Afghanistan.
Corresponding Author: Fazel Rahman Faizi, Department of Radiology, French Medical Institute for Children, Afghanistan, Tel: 93 20 250 0522; E-Mail: [email protected]
Received Date: 03 Dec 2016 Accepted Date: 27 Dec 2016 Published Date: 02 Jan 2017
Copyright © 2017 Faizi FR
Citation: Faizi FR and Aien MT. (2017). Caudate Lobe Cystic Echinococcosis. Mathews J Case Rep 2(1): 022.
ABSTRACT
Cystic echinococcosis is a zoonotic disease produced by larva of echinococcosis granulosis. The parasite has two hosts, a definitive and an intermediate host. The definitive host is usually dogs but maybe other carnivores. The intermediate host is usually sheep but maybe other herbivores. Humans become infected accidentally through contact with dogs or contaminated water and vegetables. Liver is the most common site of involvement however caudate lobe is rarely involved. A 24 year-old female with sole complaint of jaundice was referred to our department to undergo abdominal CT-scan. A well-defined multiseptated cystic structure was noted in caudate lobe. Keeping in view patient's history of contact with animals and imaging characteristics, the diagnosis of cystic echinococcosis was made.
KEYWORDS
Cystic Echinococcosis; Caudate Lobe; Jaundice; Splenomegaly.
INTRODUCTION
Case presentation
A 24-year-old female with history of jaundice was referred to Radiology department of FMIC hospital to undergo contrast enhanced abdominal CT-scan. Her laboratory studies revealed elevated level of direct and indirect bilirubin. Pre-contrast abdominal CT demonstrated a low attenuation cystic structure with multiple internal septae occupying segment I (caudate lobe) and segment V of the liver; focal wall calcification was also apparent. (Figure 1) The lesion revealed subtle wall enhancement in post-contrast images. (Figure 2) Portal vein and intra-hepatic biliary channels were dilated. (Figure 3)Portal hypertension was evident by splenomegaly and splenic vein engorgement, dilatation and tortuosity. (Figure 3 and 4) we believe that portal vein hypertension and obstructive jaundice was due to mass effect of the lesion over CBD and portal vein at porta hepatis. (Figures 2, 4)
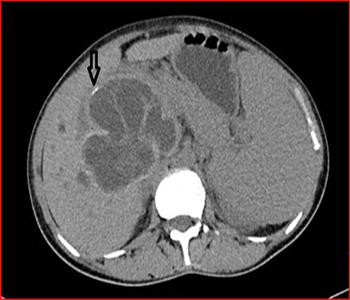
Figure 1: Pre-contrast axial slice of the abdomen demonstrates a well-defined cystic structure with multiple septae in segment I (caudate lobe) and segment V of the liver. Note the focal wall calcification of the cyst. (arrow)
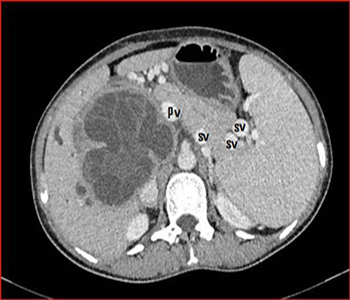
Figure 2: Post-contrast axial slice of the abdomen demonstrates subtle wall enhancement of the cyst. Note the portal vein (PV) close approximation to the cyst and splenic vein (SV) engorgement.
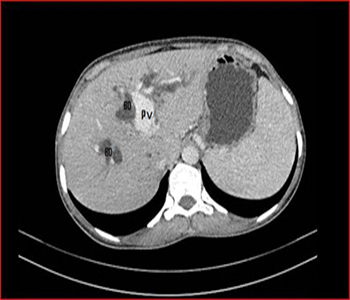
Figure 3: Post-contrast axial slice of the abdomen. Note the dilated portal vein (PV) and intra-hepatic biliary ducts (BD).

Figure 4: Post-contrast coronal slice of the abdomen. Note the cyst is producing mass effect on portal vein (large arrow) and portal hypertension is evident by splenomegaly and splenic vein engorgement and tortuosity (small arrow).
DISCUSSIONS
Cystic echinococcosis is a zoonotic disease produced by larva of Echinococcosis granulosis [1, 2]. The parasite has two hosts, a definitive and an intermediate host. The definitive host is usually a dog but maybe other carnivores. The intermediate host is commonly a sheep but maybe other herbivores. Humans become infected accidentally through contact with dog or consuming contaminated water and vegetables [1-3]. The parasite passes through intestinal wall and enters portal vein or lymphatic system. Liver is the primary site of defense, hence, the most frequently involved organ (75%). Meanwhile, right lobe of the liver is the most commonly involved lobe whereas caudate lobe is rarely involved [1, 4]. Sometimes the parasite enters systemic circulation through capillaries and may be lodged somewhere else [1]. The cyst is slowly growing and maybe clinically silent for years. Dull right upper quadrant pain is the most common clinical symptom in uncomplicated cyst [3, 4]. Complicated cyst demonstrates varying clinical manifestations like intrabiliary rupture, intra-peritoneal rupture, jaundice and portal hypertension [4]. Jaundice may occur due to rupture of the cyst in biliary channels or by cyst's mass effect over extrahepatic biliary ducts. Portal hypertension is a rare complication and it occurs in caudate lobe cystic echinococcosis [4]. The cyst may demonstrate variable imaging features based on cyst's growth stage; it may be a thick walled cystic structure; a multiseptated cystic structure; a cystic structure with detached membrane; a complex mass or totally calcified structure [2]. Ultrasound is the primary investigation of choice for detection of liver cystic echinococcosis. CT is indicated in cases where ultrasound is inconclusive due to patient's related difficulties (obesity, bowel gas, abdominal wall defect, and previous surgery) or for evaluation of complications of the cyst. MRI is superior over CT for evaluation of cyst's intra-biliary communication when typical features are absent [5]. Some serological tests are available for diagnosis of cystic echinococcosis but a gold standard test for definitive diagnosis is lacking [6]. Percutaneous aspiration-injection-reaspiration drainage (PAIR) plus albendazole/ mebendazole is superior over open surgical excision due to increased clinical efficacy and lower complication, mortality, recurrence and hospitalization [6, 7].
CONCLUSION
Cystic echinococcosis is a zoonotic disease caused by echinococcosis granulosis and is common in sheep farming countries. Humans get infected incidentally through contact with dogs or contaminated foods and vegetables. Liver is the most common site of involvement. Uncomplicated cysts are usually asymptomatic for years. Complicated cysts may present with varying clinical symptoms. Portal vein hypertension and obstructive jaundice are rare complications and are due to lesions mass effect over portal vein and common bile duct at porta hepatis. Differential diagnosis • Liver abscess • Liver malignancy
FINAL DIAGNOSIS
Caudate lobe cystic echinococcosis.
REFERENCES
- Pedrosa I, Saiz A, Arrazola J, Ferreiros J, et al. (2000). Hydatid Disease: Radiologic and Pathologic Features and Complications. 1: (CME available in print version and on RSNA Link). Radiographics. 20(3): 795-817.
- Dahniya MH, Hanna RM, Ashebu S, Muhtaseb SA, et al. (2001). The imaging appearances of hydatid disease at some unusual sites. The British journal of radiology. 74(879): 283- 289.
- Lee SK, Yen PS, Ling CM and Chou ASB. (2005). Hydatid Cyst of Liver: a case report and literature review. Chinese Journal of Radiological Medicine. 30(5): 295-299.
- Yuan, Wei-Hsin, Rheun-Chuan Lee, Yi-Hong Chou, et al. (2005). Hydatid cyst of the liver: A case report and literature review. The Kaohsiung journal of medical sciences. 21(9): 418-423.
- Kumar R, Reddy SN and Thulkar S. (2002). Intrabiliary rupture of hydatid cyst: diagnosis with MRI and hepatobiliary isotope study. The British journal of radiology. 75(891): 271-274.
- Barnes TS, Deplazes P, Gottstein B, Jenkins DJ, et al. (2012). Challenges for diagnosis and control of cystic hydatid disease. Acta tropica. 123(1): 1-7.
- Smego RA, and Sebanego P. (2005). Treatment options for hepatic cystic echinococcosis. International journal of infectious diseases. 9(2): 69-76.