Previous Issues Volume 2, Issue 2 - 2017
Art of Salvaging: Bicuspidization and Bone Grafting with Platelet Rich Fibrin in Mandibular Left First Molar – A Case Report
Ankita Dalvi1, Shivani Sachdeva*2, Harish Saluja3, Abhijeet Haridas 4
1P.G. Student at Pravara Rural Dental College and Hospital, Loni, Maharashtra
2Associate Professor at Pravara Rural Dental College and Hospital, Loni, Maharashtra.
3Reader at Rural Dental College and Hospital, Loni, Maharashtra.
4P.G. Student at Pravara Rural Dental College and Hospital, Loni, Maharashtra.
Corresponding Author: Shivani Sachdeva, Department of Periodontics Pravara Rural Dental College and Hospital, Tel: 09730548805 E-Mail: [email protected]
Received Date: 10 Apr 2017 Accepted Date: 31 Jul 2017 Published Date: 02 Aug 2017
Copyright © 2017 Sachdeva S
Citation: Sachdeva S, Dalvi A, Saluja H and Haridas A. (2017). Art of Salvaging: Bicuspidization and Bone Grafting with Platelet Rich Fibrin in Mandibular Left First Molar – A Case Report. Mathews J Case Rep 2(2): 032.
ABSTRACT
The increased desire of patients to salvage and maintain their dentition has forced conservative and regenerative dentistry to conserve the teeth in the mouth which are planned to be removed. Thus periodontally compromised teeth with severe vertical bone loss and furcation invasion may well be retained of their roots. In this case report bicuspidization of the left first mandibular molar with bone graft and Platelet Rich Fibrin (PRF) membrane and subsequent prosthetic treatments are presented.
KEYWORDS
Furcation; Intrabony Defects; Bicuspidization; PRF Membrane.
INTRODUCTION
The treatment and management of mandibular molar teeth exhibiting furcation invasions (FI) may involve restorative dentistry, endodontics and periodontics, so that the teeth are retained in whole or in part. Such teeth can be useful as independent units of mastication or as abutments in simple fixed bridges. Thus tooth separation and resection procedures are used to preserve as much tooth structure as possible rather than sacrificing the whole tooth [1].
The furcation defects vary from a subtle loss of attachment in the buccal furcation area, forming a shallow pocket, to advanced pathology with deep pockets > 10 mm, advanced bone loss and clinical exposure of the furcation [2-4]. In the mandibular molars, grade III defects are managed by tunnelling procedures, hemisection and bicuspidisation along with open flap debridement [2, 5 ,6].
The ultimate goal of periodontal therapy is to regenerate the lost periodontal tissues caused by periodontitis [7]. Various controlled clinical trials have demonstrated that some of the available grafting procedures may result in periodontal regeneration in intrabony defects, but complete and predictable reconstruction of periodontal tissues is still difficult to obtain [8]. The reason is that periodontium, once damaged has a limited capacity for regeneration [9]. The most positive outcome of periodontal regeneration procedures in intrabony defect has been achieved with a combination of bone graft and guided tissue regeneration [10, 11]
REVIEW OF LITERATURE Bisection or bicuspidization is the separation of mesial and distal roots of mandibular molars along with their coronal portion, where both segments are then retained individually [12, 13].
The following table summarize the indications and contraindications for bicuspidization:
| Indications | Contraindications |
|---|---|
|
1. Periodontal indications
|
1. General contraindications to periodontal surgery
|
|
2. Endodontic or conservativeindications
|
2. Factors associated with local anatomy
|
|
3. Prosthetic indications
|
3.Endodontic factors
|
|
4. Restorative factors
|
|
|
5. Strategic considerations
|
Endodontic therapy is performed initially, and during the open flap debridement procedure, the bicuspidization is done and the tooth is restored with a post-endodontic restoration, keeping in mind that the restoration allows for optimal plaque control in the space between the separated roots [2, 14-17].
CASE REPORT
A 31-year-old male presented with the complaint of pain of left mandibular first molar with slight mobility. On examination, the tooth was sensitive to percussion. On probing the area, there was a 9-mm-deep periodontal pocket around the mesial aspect of the furcation area (Figure 1).

Figure 1:
On radiographic examination, severe vertical bone loss was evident at the mesial aspect of the furcation area. The bony support of distal root was completely intact but at mesial roots level was compromised due to presence of deep infrabony pocket (Figure 2).
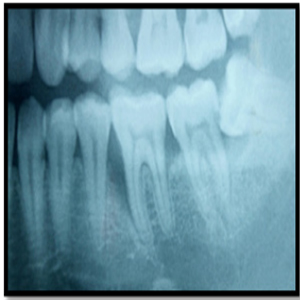
Figure 2:
The working canal length was determined and the canals were biomechanically prepared using step back technique. A long shank tapered fissure carbide bur was used to make vertical cut toward the bifurcation area. Surgical procedure was planned with bicuspidization technique and alveolar bone regeneration using Decalcified freeze dried bone allograft (DM-Bone) (Figure 3) and Platelet Rich Fibrin (PRF) membrane (Figure 4).
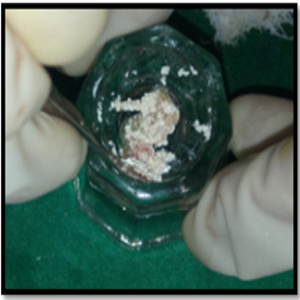
Figure 3:
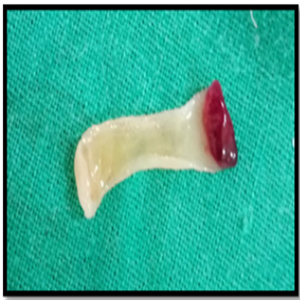
Figure 4:
A full thickness flap was reflected with the crevicular incision extending from the distal surface of the mandibular 2nd premolar to the midfacial surface of the mandibular 2nd molar (Figure 5). After the flap elevation, the tooth was dissected and the gutta-percha cones and other restorative surplus were removed from the furcation (Figure 6).

Figure 5:

Figure 6:
All faces of the mesial and distal roots were instrumented and the spurs were smoothened with aerotor. After thorough curettage of the mesial vertical osseous defect and irrigation with saline solution, the bone graft (DM-Bone) was placed in the defect and condensed followed by coverage with patient's PRF membrane. The flap was repositioned and sutured and a periodontal dressing was given. (Figure 7-8).

Figure 7:

Figure 8:
Six weeks after surgery, the dissected portions were prepared for a splinted stainless steel restorations and each dissected parts of the tooth was crowned as a premolar tooth (Figure 9). The patient was followed at 3, 6, 12 and 24 months after surgery, and clinical measurements and radiographies were recorded.

Figure 9:
DISCUSSION
Management of deep infrabony pocket, encroaching root apex of posterior teeth along with furcation involvement, always presents a challenge to the periodontist. Non-surgical management alone leads to failure due to inaccessibility of the base of the pocket and the furcation region, leading to an incomplete removal of the plaque and plaque retentive factors [2, 18, 19]. The clinician splits the mandibular molar vertically through the furcation, without removing either half, leaving two separate roots that then are treated as bicuspids (a procedure termed “bicuspidization”).
Farshchian and Kaiser [20] have reported the success of a molar bisection with subsequent bicuspidization. They stated that the success of bicuspidization depends on three factors: 1. Stability of, and adequate bone support for, the individual tooth sections; 2. Absence of severe root fluting of the distal aspect of the mesial root or mesial aspect of the distal root; 3. Adequate separation of the mesial and distal roots, to enable the creation of an acceptable embrasure for effective oral hygiene.
According to Newell [21], the advantage of bisection is the retention of some or all the tooth structure and the disadvantage is that the tooth has to undergo endodontic therapy. Not many studies have been cited in the literature regarding the use of bicuspidised molar teeth as a viable abutment for a fixed partial bridge. The role of endodontic care prior to bicuspidization procedure has a long history and it has remained today as a necessity in treating furcally involved mandibular molars. However, failure to perform endodontic treatment first is not a contraindication for root resectioning if it can be determined that a successful root canal filling is practical and possible.
The treatment for deep infrabony pocket (vertical bone loss) requires the use of various regenerative procedures but PRF belongs to a new generation of platelet concentrates geared to simplify preparation without biochemical blood handling. PRF is considered as a fibrin biomaterial. Its molecular structure with low thrombin concentration is an optimal matrix for migration of endothelial cells and fibroblasts. It permits a rapid angiogenesis and an easier remodeling of fibrin in a more resistant connective tissue. Therefore, these PRF membranes can be used for all types of superficial cutaneous and mucous healing. Not only is it a simple fibrin membrane but also a matrix containing all the molecular and cellular elements permitting optimal healing. The matrix carries all the favorable constituents present in a blood sample. That is why this biomaterial can be considered a physiological concentrate. It is obtained without any addition or manipulation. A case was provided successful treatment of dehiscences with PRF and autogenous bone graft at the implant dehiscence site which could be compared to the regeneration required in our case [22].
CONCLUSION
Bicuspidization may be an apt alternative to extraction and implant therapy and should be discussed with patients during consideration of treatment options. With recent refinements in endodontics, periodontics and restorative dentistry root separation and resection have received acceptance as a conservative and dependable dental treatment and the functional needs have been adequately met with by such treated teeth.
REFERENCES
- Vandersall DC and Detamore RJ. (2002). The mandibular molar Class III furcation invasion. A review of treatment options. JADA. 133(1): 55-60.
- Andreasen FM, Andreasen JO and Cvek M. (2007). Root fractures. In: Textbook and Color Atlas of Traumatic Injuries to Teeth. Andreasen FM, Andreasen JO, eds. Copenhagen: Blackwell Publishing Ltd. 337-371.
- Grossmann Y, Araúz-Dutari J, Chogle SM, Blatz MB, et al. (2006). A conservative approach for the management of a crownroot fracture. Quintessence Int. 37(10): 753-759.
- Arhun N, Arman A, Ungor M and Erkut S. (2006). A conservative multidisciplinary approach for improved aesthetic results with traumatized anterior teeth. Br Dent J 201(8): 501-512.
- Luebke RC. (1984). Vertical crown-root fractures in posterior teeth. Dent Clin North Am. 28(4): 883-895.
- Schetritt A and Steffensen B. (1995). Diagnosis and management of vertical root fractures. J Can Dent Assoc. 61(7): 607-613.
- Froum SJ, Gomez C and Breault MR. (2002). Current concepts of periodontal regeneration. A review of the literature. N Y State Dent J. 68(9): 14-22.
- Trombelli L. (2005). Which reconstructive procedures are effective for treating the periodontal intraosseous defect? Periodontol 2000. 37: 88-105.
- Bartold PM, Shi S and Gronthos S. (2006). Stem cells and periodontal regeneration. Periodontol 2000. 40: 164- 172.
- . McClain PK and Schallhorn RG. (1993). Long-term assessment of combined osseous composite grafting, root conditioning, and guided tissue regeneration. Int J Periodontics Restorative Dent. 13(1): 09-27.
- Guillemin MR, Mellonig JT and Brunsvold MA. (1993). Healing in periodontal defects treated by decalcified freeze-dried bone allografts in combination with ePTFE membranes (I). Clinical and scanning electron microscope analysis. J Clin Periodontol. 20(7): 528-536.
- Tarnow D and Fletcher P. (1984). Classification of the vertical component of furcation involvement. J Periodontol. 55(5): 283-284
- Waerhaug J. (1980). The furcation problem: etiology, pathogenesis, diagnosis, therapy and prognosis. J Clin Periodontol. 7(2): 73-95.
- Trope M, Blanco L, Chivian N and Sigurdsson A. (2006). Pathways of pulp. In: Role of Endodontics after Dental Traumatic Injuries. Cohen S, Hargreaves KM, eds. Missouri: Mosby. 610-649.
- Sugaya T, Kawanami M, Noguchi H, Kato H, et al. (2001). Periodontal healing after bonding treatment of vertical root fracture. Dent Traumatol. 17(4): 174-179.
- Mullally BH and Ahmed M. (2000). Periodontal signs and symptoms associated with vertical root fracture. Dent Update. 27(7): 356-360.
- Tamse A, Kaffe I, Lustig J, Ganor Y, et al. (2006). Radiographic features of vertically fractured endodontically treated mesial roots of mandibular molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101(6): 797-802
- Flores MT, Andersson L, Andreasen JO, et al. (2007). Guidelines for fractured and luxated permanent teeth. Dent Traumatol. 23(2): 66-71.
- Rosen H and Partida-Rivera M. (1986). Iatrogenic fracture of roots reinforced with a cervical collar. Oper Dent. 11: 46-50.
- Farshchian F and Kaiser DA. (1988). Restoration of the split molar: bicuspidization. Am J Dent. 1(1): 21-22.
- Newell DH. (1991). The role of the prosthodontist in restoring root resected molars: A study of 70 molar root resections. J Prosthet Dent. 65(1): 7-15.
- Shivani S, Mangesh P, Harish S and Platelet-rich F. (2015). A physiological concentrate in the management of buccal dehiscence of implant - A case report; Journal of Pierre Fauchard Academy (India section). 29: 103-106.