Information Links
Related Conferences
Previous Issues Volume 8, Issue 10 - 2023
Acute Appendicitis due to Retained Intra-Abdominal Foreign Body: Case Report
Abbas Abdollahi, Majid Ansari*
Endoscopic and Minimally Invasive Surgery Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
*Corresponding Author: Majid Ansari, Endoscopic and Minimally Invasive Surgery Research Center, Mashhad University of Medical Sciences, Mashhad, Iran, Tel: +989153230207; Email: [email protected].
Received Date: September 22, 2023
Published Date: October 27, 2023
Citation: Ansari M, et al. (2023). Acute Appendicitis due to Retained Intra-Abdominal Foreign Body: Case Report. Mathews J Case Rep. 8(10):126.
Copyrights: Ansari M, et al. © (2023).
ABSTRACT
BACKGROUND: Retained surgical items are a type of never-occurring event in surgical patients. This study is about an extremely rare case of bilateral abdominal retained surgical sponge that led to acute appendicitis.
Retained surgical items are always complicated and may be dangerous situation that lead to even morbidity or mortality in patients. Legal issues are another consequence of this circumstance for the surgical team and health system. Retained surgical items are asymptomatic in most cases. Invasion and perforation of internal organs such as the bowel, is an extremely rare presentation of retained surgical items. A case of 40 years old female with acute appendicitis due to retained abdominal surgical sponge, which was treated by the authors, is reported in this article. Written informed consent was obtained from the patient for publication of this case report.
Keywords: Acute Appendicitis, Retained Surgical Items, Surgical Sponge, Gossypiboma, Case Report.
INTRODUCTION
BACKGROUND
One of the most important “never events” in surgical patient safety is accidentally retained surgical items (RSIs). The greatest number (62%) of RSIs findings and procedures occurred during the first hospital admission, with two days median time from the index surgery [1]. This is a case report of a woman with bilateral abdominal retained surgical sponge after five years from her last abdominal surgery that led to acute appendicitis.
Most RSIs removal surgeries are performed early, when there are no symptoms, but in the other group, focal pain, collection, and mass were the most common findings. Plain radiography is the most common diagnostic method. Errors that depend on the team or system are important reasons for RSIs rather than isolated personal errors [1]. The incidence of RSIs is traditionally 1 in 8,000 to 18,000 operations of all inpatient; furthermore, intra-abdominal RSIs incidence is approximately 0.3-1 per 1000 abdominal surgeries [2,3]. RSIs risk factors included; body mass index (BMI), unplanned intraoperative events, and procedure duration, which are associated with an increased risk of RSIs. An incorrect count of devices at any time during the procedure is a risk factor for RSIs. In contrast presence of a trainee is associated with a lower risk of RSIs than the absence of a trainee [2]. Other risk factors for RSIs include; trauma surgery [3], emergency surgery [4] and multiple major surgeries at the same time [5]. Retained sponges are the most common type of RSIs. Approximately 80% of diagnosed RSIs cases have a history of correct counting device reports at the end of the index surgery [3]. The retained sponge is called ‘Gossypiboma”, because it may lead to gossip about surgeons [6].
CASE PRESENTATION
A 40 years old woman was admitted to our emergency department (Ghaem Hospital, Mashhad) with abdominal pain for three days ago. She had a medical history of two cesarean sections in 7 and 5 years ago. She reported abdominal pain in the upper abdomen, which then shifted to the right lower quadrant. She experienced one episode of fever, anorexia, nausea, and vomiting. Physical examination revealed a fullness and mass-like lesion in the lower abdomen, with tenderness and rebound tenderness in the right lower quadrant. She had leukocytosis (WBC 17000) and elevated C-reactive protein levels. Acute appendicitis with phlegmon has been reported on abdominal ultra sonography. Computed Tomography (CT) the abdomen and pelvis revealed acute appendicitis with two huge intra- abdominal foreign bodies (Figure 1). The patient underwent midline laparotomy, intra-operative finding included; two huge intra-abdominal masses in lower abdomen with severe inflammation and adhesion of the appendix and also adhesion of the right fallopian tube and ovary to the right mass (Figure 2). The abdominal masses, appendix, right fallopian tube and right ovary were excised (Figure 3). Gross pathologic findings of both abdominal masses were contained surgical gauzes; the right mass was full of pus with invasion and perforation of the appendix tip by gauze (Figure 4). Acute suppurative appendicitis was confirmed by a permanent pathologic report.
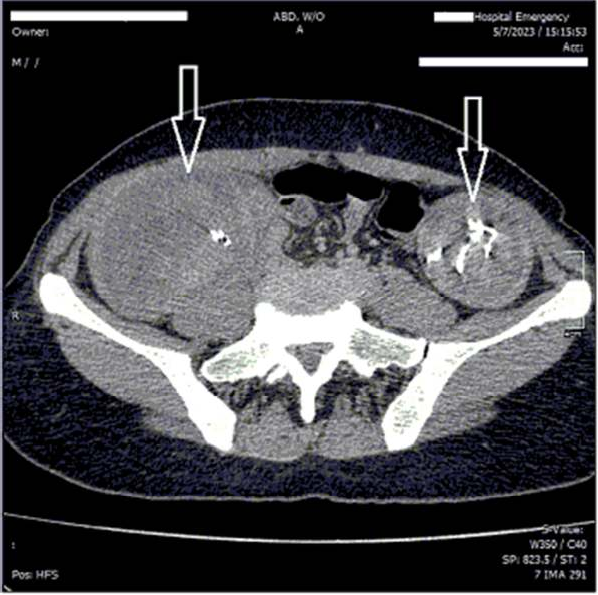 Figure 1A. Two huge abdominal masses with radiopaque strip of gauzes.
Figure 1A. Two huge abdominal masses with radiopaque strip of gauzes.
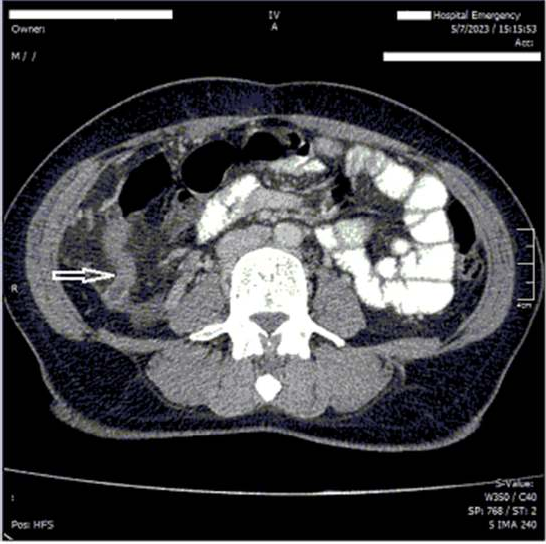
Figure 1B. Appendix with severe inflammation.
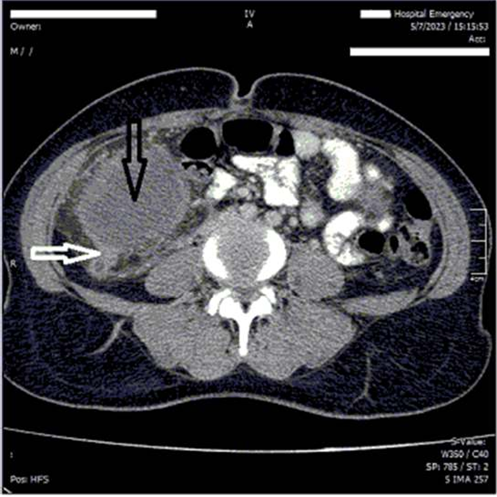
Figure 1C. Appendix with severe inflammation and adhesion to the mass (White arrow) Right huge abdominal mass (Black arrow).
.png)
Figure 2. Appendix with severe inflammation and adhesion to the mass (Black arrow) Right huge abdominal mass (White arrow).
.png)
Figure 3. Appendix with severe inflammation and adhesion to the mass (White arrow) Right huge abdominal mass containing gauzes, and full of pus (Black arrow).
.png)
Figure 4. Left (White arrow) and right (Black arrow) abdominal masses, Appendix with severe inflammation and distal luminal invasion by gauze (Red arrow).
DISCUSSION
Unintentionally retained surgical items are a terrible nightmare for surgeons. This leads to approximately 70% reoperation, 35% mortality rate, and also 80% morbidity [7]. RSIs presentation can be divided in to two groups: aseptic fibrinous manifestations, which lead to granuloma formation, and calcification. Patients with this type of disease are usually asymptomatic. The second group included inflammatory response and abscess formation. RSIs can also cause bowel obstruction, fistulization, and visceral perforations. In addition, most RSIs are found early after surgery, with three weeks mean time, but there are case reports of finding RSIs many years after surgery [8]. In this case report, the last abdominal surgery was done five years ago, and the presentation was acute appendicitis due to luminal perforation of the appendix with gauze.
Some patients` risk factor of RSIs include; surgery in an urgent set up, multiple and not simple surgeries, length of procedure, and obesity. Another type of risk factor is surgical team behavior, such as personnel changes during operation and incorrect surgical item counts [8]. In addition, using large number of surgical instruments or gauzes, and final incisional closure in absence of attending surgeon are the other risk factors [9] In this case, due to patient history; both cesarean sections were in an elective set up. Furthermore, she was not obese during her lifetime. Unfortunately, we could not assess the other risk factors, including surgical team errors, intraoperative number of instruments using and event history.
The most common RSIs are sponges [9,10], and the thorax and abdomen are the most common locations of it [10]. The highest numbers of RSIs are found during the first hospital admission [1] while aseptic foreign bodies may be asymptomatic for years [11]. Nevertheless, in this case, RSIs were found in the abdomen and were asymptomatic for years until they were infected when the appendix lumen was invaded by gauze.
Ultrasound can be helpful for retained gauze and shows a mass with a hyperechoic line or strong echo with an acoustic shadow [11-13]. CT scans are useful and can show bounded cystic lesions in retained gauze cases [11], air trapping in sponge may lead to spongiform or whirl like appearance with high density area [12]. Finding retained gauzes without marker are more difficult than with strip band [14]. In contrast, in this case, US was not helpful, and complicated appendicitis with phlegmon was reported; however, CT scan could detect acute appendicitis and two huge abdominal masses with metallic content.
It is important to know when the surgical devices count is incorrect, the closure of the surgical incision is completely wrong, unless in unstable patients [15]. However the correct surgical device count is not 100% roll out retained surgical items.
CONCLUSION
Surgical teams must always be aware of the possibility of RSIs, and if there is any uncertainty about the device count, serious effort is needed to manage the situation. Excellent team work behavior, avoidance of unnecessary personnel changes during operation, performing elective operation during day time, and not at unusual night time are some important factors to prevent RSIs.
ETHICAL APPROVAL
Due to hospital ethical board approval investigation, this case report did not meet the criteria for human subject research.
CONSENT
Written informed consent was obtained from the patients for publication of this case report and accompanying images.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
FUNDING
This case reports did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
- Stawicki SP, Cook CH, Anderson HL 3rd, Chowayou L, Cipolla J; OPUS 12 Foundation Multicenter Trials Group, et al. (2014). Natural history of retained surgical items supports the need for team training, early recognition, and prompt retrieval. Am J Surg. 208(1):65-72.
- Stawicki SP, Moffatt-Bruce SD, Ahmed HM, Anderson HL 3rd, Balija TM, Bernescu I, et al. (2013). Retained surgical items: a problem yet to be solved. J Am Coll Surg. 216(1):15-22.
- Zejnullahu VA, Bicaj BX, Zejnullahu VA, Hamza AR. (2017). Retained Surgical Foreign Bodies after Surgery. Open Access Maced J Med Sci. 5(1):97-100.
- Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. (2003). Risk factors for retained instruments and sponges after surgery. N Engl J Med. 348(3):229-235.
- Lincourt AE, Harrell A, Cristiano J, Sechrist C, Kercher K, Heniford BT. (2007). Retained foreign bodies after surgery. J Surg Res. 138(2):170-174.
- Bani-Hani KE, Gharaibeh KA, Yaghan RJ. (2005). Retained surgical sponges (gossypiboma). Asian J Surg. 28(2):109-115.
- Birolini DV, Rasslan S, Utiyama EM. (2016). Unintentionally retained foreign bodies after surgical procedures. Analysis of 4547 cases. Rev Col Bras Cir. 43(1):12-17.
- Whang G, Mogel GT, Tsai J, Palmer SL. (2009). Left behind: unintentionally retained surgically placed foreign bodies and how to reduce their incidence--pictorial review. AJR Am J Roentgenol. 193(6 Suppl):S79-S89.
- Eghbali F, Bhahdoust M, Madankan A, Mosavari H, Vaseghi H, Khanafshar E. (2022). Hidden retained surgical sponge with intestinal migration: A rare case report. Int J Surg Case Rep. 2022:107274.
- Cima RR, Kollengode A, Garnatz J, Storsveen A, Weisbrod C, Deschamps C. (2008). Incidence and characteristics of potential and actual retained foreign object events in surgical patients. J Am Coll Surg. 207(1):80-87.
- Chaya R, Okamura T, Nagai T, Kobayashi D, Kobayashi T, Akita H, et al. (2018). Case of a giant gauzeoma diagnosed 21 years after an inguinal hernia surgery. J Rural Med. 13(2):177-180.
- Bairwa BL. (2021). Gossypiboma-an unusual cause of surgical abdomen and surgeon's nightmare: A rare case report. Int J Surg Case Rep. 80:105521.
- Biswas RS, Ganguly S, Saha ML, Saha S, Mukherjee S, Ayaz A. (2012). Gossypiboma and surgeon-current medicolegal aspect-a review. Indian J Surg. 74(4):318-322.
- Kokubo T, Itai Y, Ohtomo K, Yoshikawa K, Iio M, Atomi Y. (1987). Retained surgical sponges: CT and US appearance. Radiology. 165(2):415-418.
- Kaiser CW, Friedman S, Spurling KP, Slowick T, Kaiser HA. (1996). The retained surgical sponge. Ann Surg. 224(1):79-84.