Information Links
Related Conferences
Previous Issues Volume 8, Issue 4 - 2023
About an Exceptional Complications of Intravesical BCG Therapy
Nizar Cherni1, Abdallah Chaachou1, Wael Ferjaoui2,*, Samir Ghozzi1, Mohamed Dridi1
ABSTRACT
Infectious spondylodiscitis of tuberculous origin (PDT) and renal pyonephrosis are exceptional complications of intravesical BCG therapy.
We report in this study, a case of exceptional complications of intravesical BCG therapy.
Keywords: Tuberculous, BCG Therapy, Bladder tumour
CASE REPORT
A 67-year-old patient had an endoscopic resection of a bladder tumour 3 years previously with histology of a superficial tumour requiring additional BCG intravesical therapy. Eight months later he consulted for low back pain disturbing his walking. An MRI was requested (Figure 1) showing an aspect of L4-L5 spondylodiscitis with a large peri-vertebral and anterior epidural abscessed collection. A scan-guided puncture was performed and the anatomopathological examination concluded to a granulomatous inflammation with foci of necrosis; the aspect is in favour of tuberculosis. The patient was put on quadruple therapy for 45 days and dual therapy for 2 months and 2 days. A follow-up MRI (Figure 2), after a month and a half, showed the persistence of a nodular lesion of 1.5 cm in the right frontoparietal cortico subcortical level in favour of a micro abscess of tuberculosis origin. A second biopsy was carried out and the anatomical examination was in favour of the diagnosis. The patient was put back on quadritherapy for 2 months and dual therapy for 12 months.
A follow-up MRI showed an improvement in this micro-collection under antitubercular treatment.



Figure 1: Appearance of L4-L5 spondylodiscitis with a large perivertebral and anterior epidural collection.
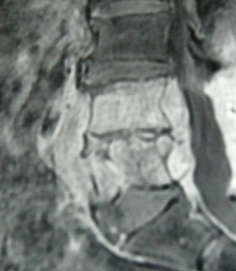
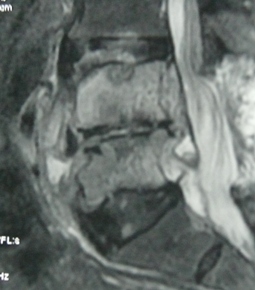
Figure 2: A nodular lesion of 1.5 cm long axis at the frontoparietal cortico subcortical level.
The patient was consulted, two months later, for right lumbago in a febrile context. On biology, he had a hyperleukocytosis and an elevated CRP. Ultrasound showed a thinned right renal parenchyma with an echogenic content. IVUS showed a non-functioning right kidney.
Measurement of creatinine clearance through the nephrostomy tube showed a non-functioning right kidney. (Creatinine clearance is 2ml/min). The patient had a right nephrectomy. Pathological examination of the specimen showed granulomatous inflammation without necrotic foci.
One year later, the patient returned to the hospital with a recurrence of metastatic tumour complicated by obstructive renal failure, partially resolved by left percutaneous drainage.
The osteoarticular complications of intravesical BCG therapy are rare, their frequency varies from 0.5 to 1%. They are arthralgia, mono or polyarthritis reactive or infectious, spinal pain (19%), and radiological sacroiliitis in 14% [1].
According to the studies, osteoarticular complications occur after at least five intravesical instillations of BCG with a delay between the last instillation and the beginning of the articular manifestation of less than two weeks [2]. In the majority of cases, it is a reactive disease.
To reduce the risk of haematogenous dissemination, and therefore any bone localization, it is recommended that intravesical instillations of BCG therapy are performed after 2 to 3 weeks of endoscopic resection or bladder biopsy. Ofloxacin can reduce the adverse effects of BCG therapy in general. However, in the case of spondylodiscitis and osteoarticular complications, this remains undetermined.
REFERENCES
- Prakash G, Pal M, Odaiyappan K, Shinde R, Mishra J, Jalde D, et al. (2019) Bladder cancer demographics and outcome data from 2013 at a tertiary cancer hospital in India. Indian J Cancer 56:54–58
- Bassi P. (2002) BCG (Bacillus of Calmette–Guerin) therapy of high-risk superficial bladder cancer. Surg Oncol 11:77–83