Prevalence and Contributing Factors of Insomnia among Elderly of Pashupati Old Aged Home (Briddhashram)
Sushila Shrestha1, Tara Roka2, Sunil Shrestha 3*, Sujyoti Shakya4
1Registered Nurse, Manmohan Cardiothoracic Vascular and Transplant Centre, TUTH Complex, Maharjgunj, Kathmandu.
2Associate Professor, Nepalese Army Institute of Health Sciences, Kathmandu
3Lecturer, Medical Biochemistry Department, Nobel College, Sinamangal, Kathmandu
4Market Planning Department, Everest Pharmaceuticals Pvt. Ltd, Tinkune, Koteshwor, Nepal.
Corresponding Author: Sunil Shrestha, Lecturer, Medical Biochemistry Department, Nobel College, Sinamangal, Kathmandu, Nepal, Tel +977-11-661399; E-Mail:[email protected]
Received Date: 21 Mar 2017
Accepted Date: 10 Apr 2017
Published Date: 11 Apr 2017
Copyright � 2017 Shrestha S
Citation:Shrestha S, Roka T, Shrestha S and Shakya S. (2017). Prevalence and Contributing Factors of Insomnia among Elderly of Pashupati Old Aged Home (Briddhashram). M J Psyc. 2(2): 014.
ABSTRACT
Insomnia is one of the major and unsolved problems in older people. The prevalence of insomnia increases steadily with age and is often a persistent problem, particularly in older adults and are often mistaken as a normal part of ageing. Studies investigating insomnia among elderly people living in geriatric homes, especially in Nepal, are rare. The objective of this study was to determine the prevalence and contributing factors of insomnia among elderly people of Social Welfare Centre Briddhashram (Old aged home), Pashupati, Kathmandu. A descriptive cross-sectional study design was conducted among 148 elderly people of 60-94 years of age, following simple random sampling technique. The tools used were semi-structured questionnaire, Athens Insomnia Scale (AIS) and Geriatric Depression Scale (GDS). The data was collected by using semistructured interview schedule and was analyzed by using SPSS version 17.0. This study highlights that around three-fifth (61.5%) of the respondents had insomnia associated with different factors such as age, suffering from increased number of physical symptoms, irregular sleep, etc. Three-fourth (75%) of the respondents complained of pain; followed by weakness of extremities (65.5%). Depression, perceived poor health status as compared to one year ago and use of drugs for long term illness were also found to be contributing factors of insomnia. Insomnia is common among elderly population.
KEYWORDS
Insomnia; Elderly; Nepal.
Ageing is a natural phenomenon and an inevitable process. Every living being born, develops, grows old and dies. With the increase in age, people lose their creativity level, problem solving ability and learning skills as well as short-term memory. All the people of the world - be they rich or poor and learned or uneducated - have to pass through this cyclical process in their lives, irrespective of their present state of strength or merit or weakness [1].
Sleep is a vital physiological process with important restorative functions. Sleep disorders and sleeping difficulties are among the most pervasive and poorly addresses problems of aging
Getting enough sleep can have a significant impact on daily function, alertness and overall quality of life [2].
Insomnia or sleeplessness, is a sleep disorder in which there is an inability to fall asleep or to stay asleep as long as desired. This sleep disorder is often practically defined as a positive response to either of two questions: �Do you experience difficulty sleeping?� or �Do you have difficulty falling or staying asleep?� [3].
With age, several changes occur that can place one at risk for sleep disturbances including increased prevalence of medical condition, increased medications use, age related changes in various circadian rhythms, and environmental and life style changes. Insomnia is generally classified as primary or secondary to some underlying cause. Primary insomnia is usually not associated with a medical or psychiatric condition. Secondary insomnia occurs most frequently in the older adult with medical or psychiatric disorders. The causes of insomnia in the elderly are divided into four groups: (1) physical diseases or symptoms, such as long-term pain, bladder or prostate problems, joint diseases such as arthritis or bursitis, and gastroesophageal reflux; (2) environmental/behavioral factors; (3) use of drugs, such as caffeine, alcohol, or prescription medications for chronic diseases; and (4) mental diseases or symptoms, such as anxiety, depression, loss of personal identity, or perceived poor health status [2, 4].
Insomnia affects almost half of adults 60 and older. Many factors can cause insomnia. However, the most common reason older adults wake up at night is to go to the bathroom. Prostate enlargement in men and continence problems in women are often the cause. As a person ages, sleep becomes more fragmented [5, 6].
In a previous study from Thailand, nearly 50% of patients over the age of 60 years had insomnia; the factors most strongly associated with insomnia were poor perceived health status and the presence of depression. Somatic comorbidities associated with aging are known to be risk factors for insomnia and depression. Given these facts, insomnia in elderly patients merits clinical attention and research [4].
Like in other developing countries, Nepal�s elderly population is increasing and facing many health problems. The increasing growth and demand of elderly people urges the active involvement of health personnel from different faculty in providing quality services to them.
This study will show the prevalence of insomnia and its associated factors among the elderly people of Pashupati Briddhashram. The findings will help in making the people aware about the possible causes of insomnia; which later on can be used in the management of insomnia at both hospital and community level.
In Nepal, very few studies are reported on insomnia among elderly people. Nepal Health Research Council (NHRC) has enlisted areas of elderly health issues in its short term research priority area. Studies on insomnia and its contributing factors in elderly are necessary to aid health planners and care professional in planning and providing appropriate promotive, preventive, curative and rehabilitative services related to insomnia to the elderly
Research DesignObservational cross-sectional study was applied in the study.
Study SiteThis study site was Pashupati Briddhashram (Old Aged Home).
Study PopulationAll the elderly people who resided in Pashupati Briddhashram (Old Aged Home).
Sample Size The sample size of the study was
n = z2p(1-p) for finite population of size N
d2 + z2p (1-p )/N
Where, p = proportion; d = sampling error that can be tolerated;
z = 1.96; confidence level; N = size of population.
The total elderly population in the Pashupati Bridhashram (Old
Aged Home) was 235.
Taking the value of p=49.3 %, the sample size calculated was;
145.7~148.
Sampling Method
Probability; simple random sampling method was used for sampling.
The lottery method was implied for the sampling process.
Data Collection Techniques and Tools
Data Collection Technique
- Interview by the researcher self Data Collection Tools
- Semi-structured questionnaire
- Athens Insomnia Scale:
Insomnia was diagnosed with the use of Athens Insomnia Scale; which assessed eight different sleep factors (rated on a 0-3 scale) among the respondents. The sleep factors are sleep induction, awakenings during night, final awakening, total sleep duration, sleep quality, well-being during the day, and functioning capacity during the day and sleepiness during the day. Elderly subject who had a total score 6 points or higher was considered as a positive case for insomnia. - Geriatric Depression Scale (Short Form)
This scale was developed by Sheikh and Yesavage as a basic screening measure for depression in older adults. This consists of 15 questions requiring �yes� or �no� answers. Of the 15 items, 10 indicate the presence of depression when answered positively, while the rest indicate depression when answered negatively. A score higher than five suggests depression.
1-5: no depression
6-10: mild depression
11-15: severe depression
Criteria for Selection of Patients
Inclusion Criteria
� All the elderly people living in the Pashupati Briddhashram
were included in the study.
Exclusion Criteria
� Elderly people who were not interested in the study were excluded.
Validity and Reliability
Pre-testing was done for validating the tools. Necessary changes
were done on the basis of results obtained from pre-testing
and final set of questionnaire had been prepared by accommodating
necessary changes under the advice of research guide
and other related expertise. Standard valid tools were also used
for measuring insomnia and depression. The questionnaire was
pre-tested for the reliability as well. Corrective actions were
taken to remove the gaps found in the tools. Pre-testing was
done among the elderly of Nijananda Briddhashram (Old Aged
Home), Taudaha; constituting about 10 percent of the total
sample population of the study.
Socio-demographic characteristics.
| n = 148 | ||||
|---|---|---|---|---|
| S.N. | Socio-demographic variables | Frequency | Percentage | |
| 1 | Age | |||
| 60-69 years | 45 | 30.4 | Mean: 73.64 | |
| 70-79 years | 60 | 40.5 | S.D.: �8.16 | |
| 80 years and above | 43 | 29.1 | ||
| 2 | Sex | |||
| Male | 70 | 47.3 | ||
| Female | 78 | 52.7 | ||
| 3 | Marital status | |||
| Married | 27 | 18.2 | ||
| Unmarried | 29 | 19.6 | ||
| Divorced | 7 | 4.7 | ||
| Widowed | 85 | 57.4 | ||
| 4 | Duration of widowhood | |||
| 1-10 years | 49 | 57.6 | Median: 10.00 | |
| 11-20 years | 19 | 22.8 | IQR: 5.00- 19.00 | |
| 21 years and above | 17 | 20 | ||
| 5 | Number of children | |||
| No children | 43 | 29.1 | Median: 2.00 | |
| 01-May | 86 | 58.1 | IQR: 0.00- 5.00 | |
| More than 5 | 19 | 12.8 | ||
| 6 | Ethnicity | |||
| Brahmin | 60 | 40.5 | ||
| Chhetri | 43 | 29.1 | ||
| Janajat | 44 | 29.7 | ||
| Dalit | 1 | 0.7 | ||
| 7 | Religion | |||
| Hindu | 141 | 95.3 | ||
| Buddhist | 7 | 4.7 | ||
| 8 | Educational status | |||
| Illiterate | 7 | 4.7 | ||
| Informal education | 32 | 21.6 | ||
| Primary level | 5 | 3.4 | ||
| Secondary level | 2 | 1.4 | ||
Ethical Consideration
The objectives of the study were clearly explained to the respondents
as well as the concerned authority of the Briddhashram,
before data collection. A letter from college was submitted
to the concerned authority and permission for data collection
was taken from the Briddhashram (Old Aged Home). Letter of
approval was obtained from the review committee of the campus.
Informed consent was taken from respondents. No one
was forced to give their consent or participate in the study. Respondents
were free to withdraw participation at any point during
the interview. Privacy, confidentiality and anonymity were
maintained.
Table 2: shows that majority of the respondents (60.1%) stated lack of
care taker as being the reason for leaving home, followed by personal
wish (25.7%). About two fifth (43.9%) of the respondents were living in
the Briddhashram (Old Aged Home) since more than 5 years. Around three
fourth of the respondents (71.6%) said that their family members didn�t
visit them. All of the respondents didn�t have any kind of financial support
from the family.
Socio-demographic characteristics
| n = 148 | ||||
| S.N. | Socio-demographic variables | Frequency | Percentage | |
| 1 | Reasons for leaving home* | |||
| Low economy | 15 | 10.1 | ||
| Family conflict | 22 | 14.9 | ||
| Lack of care taker | 89 | 60.9 | ||
| Loss of spouse | 9 | 6.1 | ||
| Personal wish | 38 | 25.7 | ||
| 2 | Duration of stay in ashram* | |||
| Upto 5 years | 83 | 56.1 | Median: 5.00 | |
| More than 5 years | 65 | 43.9 | IQR: 2.00- 10.00 | |
| 3 | Frequency of family visit in past 6 months* | |||
| No | ||||
| 1-5 times | 106 | 71.6 | Median: 3.00 | |
| More than 5 | 32 | 21.6 | IQR: 2.00- 5.25 | |
| 10 | 6.8 | |||
*Multiple Response
Data Analysis Procedure
After the collection of data, it was overviewed, checked and
verified checked for completeness, consistency and accuracy.
The raw data collected was processed, analyzed and interpreted
using the SPSS 17.0 version software. The data were analyzed
by using different statistical technique. The findings were
interpreted through frequency table.
Table 3: shows that among the respondents, three fifth (61.5%) of them had insomnia. Insomnia was diagnosed with the use of Athens Insomnia Scale which assessed eight different factors (rated on a 0-3 scale) among the respondents.
Assessment of insomnia.
| n = 148 | ||||
| Insomnia | Frequency | Percentage | ||
| Yes | 91 | 61.5 | ||
| No | 57 | 38.5 | ||
Data was obtained from 148 elderly people, yielding a 100% response rate. The elderly people included in the study were 60-94 years of age. The mean age was 73.64 years and the Standard Deviation (S.D.) was 8.167.
This study was conducted in order to find out the prevalence of insomnia and identify its contributing factors among elderly people of Pashupati Briddhashram (Old Aged Home).
Table 4: shows that majority of the respondents had the physical symptom of pain i.e. 75.0%. Around two third (65.5%) of them had weakness of extremities, followed by problem of blurred vision (54.1%). Each 8.8% of them had diarrhea and skin itching, and 4.7% had constipation.
| n = 148 | ||||
| S.No | Name of symptoms | Yes | No | |
|---|---|---|---|---|
| 1 | Pain | 111 (75.0) | 37 (25.0) | |
| 2 | Shortness of breath | 53 (35.8) | 95 (64.2) | |
| 3 | Weakness of extremities | 97 (65.5) | 51 (34.5) | |
| 4 | Fatigue and malaise | 54 (36.5) | 94 (63.5) | |
| 5 | Poor appetite | 28 (18.9) | 120 (81.1) | |
| 6 | Skin itching | 13 (8.8) | 135 (91.2) | |
| 7 | Dizziness | 25 (16.9) | 123 (83.1) | |
| 8 | Diarrhea | 13 (8.8) | 135 (91.2) | |
| 9 | Constipation | 7 (4.7) | 141 (95.3) | |
| 10 | Urinary frequency | 36 (24.3) | 112 (75.7) | |
| 11 | Urinary incontinence | 18 (12.2) | 130 (87.8) | |
| 12 | Urinary difficulty | 16 (10.8) | 132 (89.2) | |
| 13 | Blurred vision | 80 (54.1) | 68 (45.9) | |
| 14 | Difficulty hearing | 29 (19.6) | 119 (80.4) | |
| 15 | Dry mouth | 28 (18.9) | 120 (81.1) | |
Prevalence of Insomnia
This study has revealed that the prevalence of insomnia among
elderly of Pashupati Briddhashram (Old Aged Home) is three
fifth (61.5%). This finding is similar to a study conducted in three
French cities [7], where more than 70% of the elderly reported
at least one insomnia symptom. The finding is also similar to
the study conducted in Panchthar district of Nepal [6]; which
reported that difficulty maintaining sleep was the most common
form of insomnia among the elderly i.e. 61.3% and 49.3%
had difficulty initiating sleep. Moreover, the finding is similar to
the study conducted in Northern Taiwan [4], where insomnia
criteria were met for 41.4% individuals. The finding is in contrast
with the finding of the study done in Hong Kong [8], where
the prevalence of insomnia was reported to be 11.9% respectively.
The finding is also in contrast with the study conducted
in long-term care residents of Canada [9], where the prevalence
of insomnia was 6.2%
Table 5: shows that most of the respondents had the physical symptoms
for more than 6 months. Majority of them had difficulty hearing (96.6%)
and blurred vision (93.8%) for more than 6 months. Similarly, 92.6% of
them had fatigue; 91.8% had weakness of extremities; 90.6% had shortness
of breath; 89.3% had dry mouth; 88.9% had urinary incontinence;
88.3% had pain; for more than 6 months.
Duration of physical symptoms.
| S.No | Name of symptoms | Yes | No |
| 1 | Pain | 111 (75.0) | 37 (25.0) |
| 2 | Shortness of breath | 53 (35.8) | 95 (64.2) |
| 3 | Weakness of extremities | 97 (65.5) | 51 (34.5) |
| 4 | Fatigue and malaise | 54 (36.5) | 94 (63.5) |
| 5 | Poor appetite | 28 (18.9) | 120 (81.1) |
| 6 | Skin itching | 13 (8.8) | 135 (91.2) |
| 7 | Dizziness | 25 (16.9) | 123 (83.1) |
| 8 | Diarrhea | 13 (8.8) | 135 (91.2) |
| 9 | Constipation | 7 (4.7) | 141 (95.3) |
| 10 | Urinary frequency | 36 (24.3) | 112 (75.7) |
| 11 | Urinary incontinence | 18 (12.2) | 130 (87.8) |
| 12 | Urinary difficulty | 16 (10.8) | 132 (89.2) |
| 13 | Blurred vision | 80 (54.1) | 68 (45.9) |
| 14 | Difficulty hearing | 29 (19.6) | 119 (80.4) |
| 15 | Dry mouth | 28 (18.9) | 120 (81.1) |
Age
In this study, about three fourth (76.7%) of the elderly who were
76 years and above had insomnia, whereas around half (51.1%)
of the elderly who were 60-75 years had insomnia. There
was strong statistical significance between age and insomnia
(p=0.002). The finding is similar to the finding of the study in
Zagazig city [2], where it was reported that the prevalence of
insomnia was higher among the elderly who were above 65
years (63.9%). The finding is consistent with the study in Alexandria,
Egypt [10], where it was concluded that advanced age
was significantly associated with the insomnia symptoms. The
finding is also similar to the study conducted in Hong Kong [8] in
which the prevalence of insomnia was shown to increase with
age (p<0.001). The finding is also consistent to one of the study
done among Greek population [11], where it was found out
that insomnia increased with age (p<0.001).
Table 6: shows the total number of physical symptoms present among the respondents. More than half of the respondents (52.7%) had more than 3 physical symptoms. The median of number of physical symptoms is 4.00.
| n = 148 | ||||
| Number of physical symptoms | Frequency | Percentage | ||
| Up to 3 symptoms | 62 | 41.9 | Median: 4.00 | |
| More than 3 symptoms | 78 | 52.7 | IQR: 2-6 | |
Sex
In this study, more than two third (67.9%) of the females and
just more than half (54.3%) of the males had insomnia; but
there was no statistical significance between sex and insomnia
(p>0.005). The finding is similar to the study by [12] in which it
was concluded that men were less likely than female to develop
insomnia symptoms. The result is consistent with the result of
the study in Zagazig city [2] where females developed insomnia
more commonly than males (61.1% vs. 38.9%). Similarly, the
study in Hong Kong [8] reported that the insomnia symptoms
were more common in females than males (14% vs. 9.3%). Similarly,
a study in china [13] showed that women reported more
insomnia symptoms than men (36.4% vs. 28.7%, p=0.001).
Similarly, according to the study by [7]; women reported more
insomnia symptoms than men (75% vs. 70%, p=0.0001). The
result is similar to the study by [4] in Northern Taiwan, which
concluded that insomnia was more common in women than in
men (63.3% vs. 36.7%). The finding is in contrast to the study
conducted in Cairo, Egypt [13]; where a significantly higher percentage of males suffered insomnia more than females (45%
vs. 22.6%).
Table 7: shows that two fifth of the respondents experienced cough during
night (41.2%). About 28.4% of them had the problem of nocturia. Only
1.4% of them had the problem of snoring during sleep.
Presence of problems during night sleep
| n = 148 | ||||
| S.N. | Problems | Yes | No | |
|---|---|---|---|---|
| 1 | Cough | 62(41.2) | 87 (58.8) | |
| 2 | Nocturia | 42 (28.4) | 106 (71.6) | |
| 3 | Snoring | 2 (1.4) | 146 (98.6) | |
| 4 | Bad dreams | 15 (10.1) | 133 (89.9) | |
| 5 | Apnea | 11 (7.4) | ||
Marital status
In this study, more than two third (72.4%) of the unmarried
group of elderly, followed by less than two third (62.0%) of divorced
and widowed, and less than half (48.1%) of the married
had insomnia. The result is similar to the study done in Zagazig
city [2]; where insomnia was found to be highest among
divorced, widowed and single group of elderly i.e. 66.7%. The
result is in contrast with the study conducted in Cairo, Egypt
[13]; where it was reported that married individuals suffered
insomnia at a significantly higher percentage than unmarried,
divorced, separated and widows. The finding also contrasts
with the study done by [7] which concluded that widowed or
divorced condition was significantly associated with insomnia
symptoms (p<0.0001).
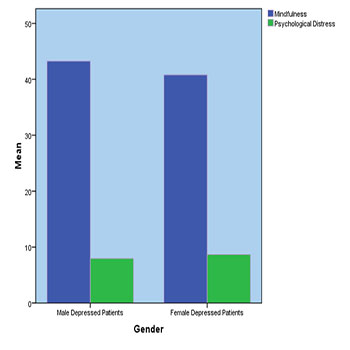
The present study was aimed to explore the relational aspect of mindfulness and psychological distress. Finding of the study confirmed that mindfulness has negative relationship with psychological distress. As mindfulness will increase psychological distress will decrease in depressed patients. Finding showed that mindfulness has negative impact on psychological distress. Gender played a significant role in the identification of mindfulness level in depressed patients. High level of mindfulness showed in male patients than female patients. But no significance difference of psychological distress was found in term of gender.
Limitations also exist when it comes to measures of critical independent variables along with the theoretical frameworks we were looking at intended to stand for. Sample composition is relative small. Current study based on cross-sectional method and longitudinal method is best way to get depth knowledge about depressed patients.
In future researchers must notice these suggestions: Sample size of the research must be increase and across the nation exploration is required. This examination has established the relationship between mindfulness and positive thinking but in future exploration causal relationship highly recommended. More demographic variables like forgiveness, personality and happiness ought to be explored in the role of mental health.
- Kabat-Zinn J. (2003). Mindfulness-based interventions in context: Past, present and future. Clinical Psychology: Science and Practice. 10(2): 144-156.
- Brown K W and Ryan R M. (2003). The benefits of being present: Mindfulness and its role in psychological wellbeing. Journal of Personality and Social Psychology. 84(4): 822-848.
- Germer C K, Siegel R D and Olendzki A. (2005). Mindfulness: what is it? What does it matter? In R. D. S. C. K. Germer, & P. R. Fulton (Ed.), Mindfulness and Psychotherapy. New York: The Guildford Press.
- Kabat-Zinn J. (1994). Wherever you go, there you are: mindfulness Meditation in everyday life. New York: Hyperion.
- Linehan MM. (1994). Acceptance and change: The central dialectic in psychotherapy. In S. C. Hayes, N. S. Jacobson, V. M. Follette & M. J. Dougher (Eds.), Acceptance and Change: Content and Context in Psychotherapy (pp. 73- 86). Reno, NV: Context Press.
- Kingston T, Dooley B, Bates A, Lawlor E et al. (2007). Mindfulness based cognitive therapy for residual depressive symptoms. Psychology and Psychotherapy. 80(2): 193-203.
- Evans S, Ferrando S, Findler M, Stowell C, et al. (2008). Mindfulness-based cognitive therapy for generalized anxiety disorder. Journal of Anxiety Disorders. 22(4): 716- 721.
- Barlow D and Durand V. (2005). Abnormal psychology: An integrative approach. Belmont,CA: Thomson Wadsworth.
- Horwitz A V, Scheid T L and Brown T N. (1999). Approaches to mental health and illness: conflicting definitions and emphases. In Howitz AV (ed.) Handbook for the study of mental health.New York: Cambridge University Press. 1-11.
- Leigh J, Bowen S and Marlatt G A. (2005). Spirituality, mindfulness & substance abuse. Addictve Behavior. 30(7): 1335-1341.
- Follette V, Palm K M and Pearson A N. (2006). Mindfulness and trauma: Implications for treatment. Journal of Rational-Emotive & Cognitive-Behavior Therapy. 24(1): 45-61.
- McCullough M E, Emmons R A and Tsang J. (2002). The grateful disposition: A conceptual and empirical topography. Journal of Personality and Social Psychology. 82(1): 112-127.
- Nakamura Y M and Orth U. (2005). Acceptance as a coping reaction: Adaptive or not? Swiss Journal of Psychology. 64(4): 281-192.
- Kessler R C, Barker P R, Colpe L J, Epstein J F, et al. (2003). Screening for serious mental illness in the general population. Arch Gen Psychiatry. 60(2): 184-189.
- Walach H, Buchheld N, Buttenmuller V, Kleinknecht N, et al. (2006). Measuring Mindfulness--The Freiburg Mindfulness Inventory (FMI). Personality and Individual Differences. 40(8): 1543-1555.