Previous Issues Volume 2, Issue 2 - 2017
Specific Phobia Following Road Traffic Collision: Medico-Legal Issues of Causation, Diagnosis, and Prognosis in Single Case Study
Hugh Koch1, Paul Elson2, Richard Cosway3, Sophie Mayhew4
1Hugh Koch, Chartered Psychologist, Hugh Koch Associates, Cheltenham, U.K., visiting Professor to Stockholm University, Sweden.
2Paul Elson, Chartered Psychologist, Cheltenham & Cardiff.
3Richard Cosway, Chartered Psychologist, Cheltenham & Edinburgh.
4Sophie Mayhew, Chartered Psychologist, Cheltenham & Truro.
Corresponding Author: Hugh Koch, Chartered Psychologist, Hugh Koch Associates, Cheltenham, U.K., visiting Professor to Stockholm University, Sweden. Tel: 01242 263 715; E-Mail: [email protected]
Received Date: 14 Mar 2016 Accepted Date: 15 Jun 2017 Published Date: 19 Jun 2017
Copyright © 2017 Koch H
Citation: Koch H, Elson P, Cosway R and Mayhew S. (2017). Specific Phobia Following Road Traffic Collision: MedicoLegal Issues of Causation, Diagnosis, and Prognosis in Single Case Study. Mathews J Case Rep 2(2): 029.
ABSTRACT
The multi-faceted assessment process involved in providing evidence of psychological injuries to the courts is illustrated with particular reference to a case study of a road traffic collision claimant diagnosed with a specific travel phobia. The need for reliable medico-legal processes is emphasized.
KEYWORDS
Road Traffic Collision (RTC); Medico-legal postulates; Diagnosis.
INTRODUCTION
Assessing trauma in personal injury compensation cases in the civil courts is complex. It involves consideration of many overlapping clinical and medico-legal issues [1]. Experts providing evidence need experience in assessing reliability and truthfulness [2, 3]. This publication addresses these issues in the context of a road traffic collision (RTC) and a common cluster of psychological symptoms, diagnosed as a specific phobia (travel), classified as DSM-V 300.29 [4]. The case study individual presented here who was seen by the first author is anonymised, and an aggregation of salient features seen across several cases are discussed here.
BACKGROUND OF RTC CASE
Mr. Smith (21 years of age) was a rear seat passenger in a 4x4 vehicle travelling on a dual carriageway outside London. The vehicle was hit by an oncoming vehicle - both vehicles were travelling at approximately 60 mph. The claimant's vehicle was knocked into a ditch and rolled over partially. The claimant attended a nearby hospital with physical injuries to his neck, shoulders and back, however he was not admitted to hospital. He sought help and advice from his general practitioner (GP). He had previously been learning to drive prior to the index accident.
FIRST ASSESSMENT
The claimant was interviewed approximately 9 months postaccident. He described a mixture of post-traumatic stress symptoms, mood disturbance, social withdrawal, and, predominantly, travel anxiety as both a passenger and a 'learner' driver. This was supported by history of GP attendance. Although the stress and mood disturbance had largely subsided, his main difficulty with travelling remained. The interviewer considered a range of diagnoses as illustrated in the amended road map/decision tree, for anxiety, [5] in (Figure. 1) below.
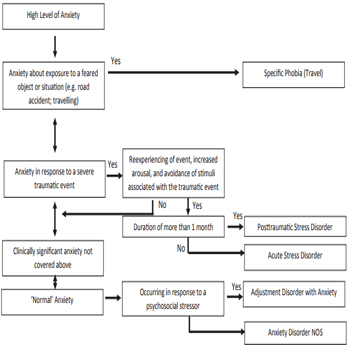
Figure 1: Amended Decision Tree for Anxiety.
To obtain a differential diagnosis for a specific phobia, this cluster of symptoms must be differentiated from other anxietybased disorders as illustrated in (Figure 2) below [5].
Figure 2: Differential Diagnosis for Specific Phobia.
| Specific Phobia must be Differentiated from... | In contrast to the specific phobia, the other condition... |
|---|---|
| Panic Disorder with Agoraphobia | Is characterized by recurrent unexpected Panic Attacks and avoidance of typically many different situations |
| Social Phobia | Is characterized by fear and avoidence of social situations. |
| Avoidance in Posttraumatic Stress Disorder | Is related to stimuli that remind the individual of a previously experienced life-threatening event. |
| Avoidance in Obsessive-Compulsive Disorder | Is associated with the content of the obsessions (e.g. dirt, contamination) |
| Avoidance in Separation Anxiety Disorder | Is associated with fear of separation from parents or caretakers. |
| Avoidance in Psychotic Disorders | Is in response to a delusion (without the recognition that the fear is excessive or unreasonable) |
| Non-pathological avoidance of circumscribed objects or situations | Lacks clinically significant impairment or distress (e.g. person who fears snakes but lives in Manhattan. |
Having decided the 'best fit' diagnosis for Mr. Smith was a Specific Phobia (Travel), the expert assessed that the claimant's ongoing phobia of travelling was unlikely to resolve spontaneously and he therefore recommended 8 - 10 sessions of cognitive-behavioural therapy (CBT), focusing on a gradual re-exposure model in line with prevailing research [6]. Psychometric test data using the GAD-7 & PHQ-9 indicated a high level of low mood and anxiety which acted as a base line measure of his general psychological state/difficulties. [7, 8].
SECOND ASSESSMENT
12 months later, the expert was re-instructed to review Mr. Smith's psychological status, following receipt of 10 sessions of CBT which had focused on gradual re-exposure to travel situations of increasing complexity. He reported significant improvement in his travel anxiety and avoidance with no current disruption. Repeated psychometric testing was consistent with a lowered level of mood disturbance and generalised anxiety, as shown in (Figure 3).
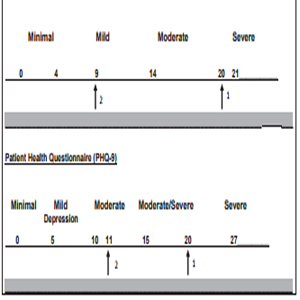
Figure 3: Psychometric Scores On Two Occasions.
Raw scores and ranges are shown above.
MEDICO-LEGAL ISSUES IN MR. SMITH'S CASE
The two assessments of Mr. Smith's psychological status and the opinions given to the Court were consistent with commonly held medico-legal postulates (9) shown in (Figure 4) below.
Figure 4: Koch's Medico-legal Postulates.
- A robust opinion should address diagnosis, causation, and attribution, duration and prognosis.
- A robust opinion will include more than one type of evidence. An opinion based on claimant self-report only may still be valid but is a 'weak' opinion in medico-legal terms.
- The classification/diagnostic categories given in DSM V and ICD 10 are a part of an expert's opinion/formulation - this systematic check of relevant criteria must be balanced by wider clinical judgement. (Figure 4 continued)
- The expert's Mental State Examination should be consistent with the claimant's description of currently active symptoms - a clear discrepancy reduces the robustness/strength of an opinion
- A robust opinion should include a history of factors which could, on the balance of probabilities, affect a specific index event reaction.
- A robust opinion should give particular emphasis to the 12 month period prior to and post the index event, but not to the exclusion of earlier or later history.
- . An expert opinion should incrementally increase in robustness over time with access to more data and discussion with other relevant professionals both legal and clinical.
- An expert's opinion should be the 'best fit' professional view of all available data at that time, and should be modified, if appropriate, as and when new data becomes available.
- It is incumbent on the expert to be impartial, independent of instructing party, and maintain as a high level of logicality as possible when appraising evidence.
In particular, Mr. Smith's history included the following
Causation One previous road accident Although in some publications the general recommendation is not to manage bone voids larger than 5 cm with autogenous grafts [4, 26]. The use of non vascularized autogenous bone grafting for larger segmental bone defects (up to 16 cm) has been described to provide satisfactory results in several case series [14, 25, 27-29] (Figure 1). Pre-existing vulnerability to anxiety High frequency of driving prior to accident
Attribution Post accident bereavement Feelings of injustice Pre-existing vulnerability to anxiety Use of 'but for' theorem to assess attribution (10)
Prognosis Evidence-based 'default' model for post trauma recovery
Credibility of Claimant Given the complex area of claimant reliability in personal injuries previously described (3), a list of credibility variables were addressed by the interviewer which included verbal and nonverbal behavioral cues and content analysis of self-report, witness statement and pre-interview questionnaire. An overall aggregated score was consistent with Mr. Smith being a highly credible/reliable historian.
CONCLUSION
This case study and description of clinical and medico-legal aspects of assessing and treating a trauma reaction diagnosed as a specific phobia illustrates the many facets of this type of evidence collection in civil cases including the essential proof of causation [10]. It has shown the need for concise and reliable assessment followed by rapid formulation of treatment requirements in line with recommended guidelines [11]. It is essential that experts and lawyers are fully aware of diagnostic factors such as range of opinion and decision-making analysis as well as the medico-legal postulates underpinning the whole assessment process.
REFERENCES
- Koch HCH. (2016). Medico Legal Case Commentary: Interface Between Clinical Opinion and Legal Case Reporting in Personal Injury Litigation. Mathews Open Access Journal. 1(1): 1-5.
- Koch HCH and Elson P. (2017). Areas of Medico-legal Unreliability in Personal Injury Cases. MJ Case. 2(1): 1-3.
- Koch HCH, Court K and Bates S. (2017). Medico-Legal Implications of Assessing Unreliability in Civil Compensation Cases: A Case Study Reflecting Potential Unreliability. Scholarena SAJ Case Reports. 4:106.
- APA. (2013). Diagnostic and Statistical Manual of Mental Disorders - V. Washington DC. USA
- First MB, Frances A and Pincus HA. (1995). DSM-IV Handbook of Differential Diagnosis. APA. Washington.
- De Jongh A, Holmshaw M, Carswell W and Van Wijk A. (2011). Usefulness of a Trauma-Focused Approach to Travel Phobia. Clin Psychol. Psychother. 8(2): 124-137.
- Spitzer RL, Kroenke K and Williams JB. (1999). Validation and Utility of a Self-Report Version of PRIME-MD: The PHQ Primary Care Study. JAMA. 282(18): 1737-1744
- Spitzer ARL, Kroenke K, Williams JB and Lowe B. (2006). A brief measure for assessment and generalised anxiety dis-order: the GAD-7. Arch Intern Med. 166(10): 1092-1097
- Koch HCH. (2016). Legal Mind: Contemporary Issues in Psychological Injury and Law. Expert Witness Publications. Manchester.
- Steel S. (2015). Proof of Causation in Tort Law. Cambridge Press.
- . Koch HCH, Knight A, Payne L and Thorns T. (2011). Managing Travel Phobia and Anxiety. British Journal of Wellbeing. 2(4): 41-45.