Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
The Role of Mesenchymal Stem Cells in Modulating the Immune System and Repairing Lung Damage in ARDS Patients with SARS-COV-2
Amir Nejad-Moghaddam1,2,*, Aram Asareh Zadegan Dezfuli3, Saeed Rahmanzadeh4
1Marine Medicine Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran 2Department of Basic Sciences, Faculty of Science, Imam Khamenei University, Zibakenar, Rasht, Iran 3Department of Microbiology, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran 4Enzyme Technology Lab, Genetics & Metabolism Research Group, Pasteur Institute of Iran, Tehran, Iran *Corresponding Author: Amir Nejad-Moghaddam, Marine Medicine Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran; Tel: +98-9112276563; E-mail: [email protected]
Received Date: September 26, 2023
Publication Date: November 14, 2023
Citation: Nejad-Moghaddam A, et al. (2023). The Role of Mesenchymal Stem Cells in Modulating the Immune System and Repairing Lung Damage in ARDS Patients with SARS-COV-2. Mathews J Cytol Histol. 7(2):24.
DOI: https://doi.org/10.30654/MJCH.10024
Copyright: Nejad-Moghaddam A, et al. © (2023)
ABSTRACT Disease characteristics and pathogenesis of coronavirus 2019 (COVID-19) have been greatly elucidated, but there is currently no specific treatment to induce regeneration of lung damage. In severe cases, acute SARS-CoV-2 infection leads to a deficiency of the immune system and consequently damage to immune responses, resulting in impaired immune cell function. Mesenchymal stem cells (MSCs), which are involved in the regulation and regeneration of the immune system, can be considered as a treatment option because they may regulate the inflammatory response caused by cytokine storms and improve lung damage. Recently, MSCs according to their immunomodulatory and regenerative properties attract attention in clinical trials. Since the outbreak of COVID-19, a series of MSC-related clinical trials have been performed. The findings show that MSC treatment not only reduces lung damage but also improves immune function by reducing cytokine storms. In this article, we reviewed therapeutic advances and trials of using MSCs to treat SARS-CoV-2 injury. Keywords: Cytokine Storm, Cell Therapy, Mesenchymal Stem Cells, Inflammatory Response, Regeneration, Coronavirus 2019 (COVID-19), SARS-CoV-2, ARDS
INTRODUCTION
COVID-19 due to Acute Respiratory Syndrome of Coronavirus 2 (SARS-CoV-2) has affected more than 692 million patients and by Aug 8, 2023, more than 6.9 million deaths have been reported [1]. SARS-CoV-2 causes a range of clinical manifestations, ranging from mild to moderate respiratory symptoms to acute respiratory syndrome and eventual death. Patients with acute SARS-CoV-2 infection often show a set of symptoms similar to those of peer viruses such as SARS and influenza [2]. The innate and adaptive immune responses of the host, especially the adaptive immune against SARS-CoV-2, play a key role in controlling viral infection. Hyper inflammation and cytokine storm are considered to be the main causes of lung organ damage that cause severe progression of COVID-19 [3]. Thus, apart from conventional antiviral therapies and oxygen therapy, immunomodulatory therapeutic strategies may potentially prevent disease progression and save patients with COVID-19, especially in critical and acute cases. Many immunotherapeutic approaches have been used for COVID-19, including glucocorticoid therapy [4,5], plasma therapy [6,7], and the use of anti-interleukin monoclonal antibodies [8-10]. However, the side effects and efficacy of the various applied treatments have necessitated further studies to identify the safety and efficacy of alternative immune-modulating regimens.
In the last ten, the safety and efficacy of adult mesenchymal stem cells (MSCs) transplantation have been reported for the treatment various chronic diseases such as systemic lupus erythematosus [11], graft-versus-host disease (GVHD) [12], chronic obstructive pulmonary disease (COPD) [13], asthma [14] and lung injuries caused by sulfur mustard [15,16]. It should be noted that MSC therapy has been also used for animal models and patients with influenza, which significantly inhibited the inflammatory response induced by immune cells and reduced further lung damage [17-19]. Mesenchymal stem cells have also been used to treat patients with acute respiratory distress syndrome (ARDS) [20,21]. From the outbreak of COVID-19 until November 2021, 85 clinical trials of mesenchymal stem cells for the treatment of COVID-19 have been reported at ClinicalTrials.gov [22].
CYTOKINE STORM
Cytokines are a range of small proteins released by cells to control cellular functions such as proliferation and differentiation [23]. In COVID-19 infection, the virus uses interstitial serine protease-2 (TMPRSS2) and angiotensin-converting enzyme (ACE2) as its receptors through its epithelial spike glycoprotein. After binding to the ACE2 receptor on the surface of the target cell, the virus enters the uncoated RNA genome into the cell cytoplasm and replicates its viral genome using the capabilities of the infected cell [24]. The binding of the virus to the host through these cell surface receptors causes overactivity of the nuclear factor κB (NF-kB), mainly in non-immune cells, including lung epithelial cells, which produce more cytokines and chemokines [25]. Serum levels of angiotensin 2 (Ang2) increase with ACE2 occupancy at the cell surface by the virus [26]. Ang2 acts as both a vasoconstrictor cytokine and a pro-inflammatory cytokine via angiotensin receptor type 1 (AT1R) [27]. This action activates a cascading chain of molecules involved in inflammation and activation of the JAK2/1 kinase signal pathway and STAT3 transcription factor in non-immune cells such as epithelial, endothelial, and fibroblast cells [28]. Thus, SARS-CoV-2 infection activates NF-κB and STAT3 in the respiratory system (Figure 1). During the inflammatory process, the main stimulus of STAT3 is the inflammatory factor IL-6 [29]. Evidence has shown that immune impairment exacerbates the complications of COVID-19. The natural antiviral immune response requires the activation of the inflammatory pathways of the immune system. However, abnormal host immune responses can exacerbate the disease if left unchecked [30]. Cytokines are an important part of the inflammatory process and are produced by several immune cells, including macrophages, dendritic cells, natural killer cells (NK cells), and the T and B lymphocytes of the adaptive immune system [31]. During an innate immune response to viral infection, pattern recognition receptors (PRRs) detect the various molecular structures that characterize the invading virus [32]. These molecular structures are referred to as pathogen-related molecular patterns (PAMPs) [33]. The binding of PAMPs to PRRs initiates an inflammatory response against the invading virus, which activates several signaling pathways and subsequently transcription factors that induce the expression of genes responsible for producing several products involved in the host's immune response to the virus. Among them are genes that encode several pro-inflammatory cytokines [34]. The main transcription factors activated by PRRs include nuclear factor-kB (NFkβ), activation protein 1, and interferon response factors 3 and 7. These transcription factors induce the expression of genes encoding inflammatory cytokines, chemokines, and cell adhesion molecules. These events recruit leukocytes and plasma proteins to the site of infection to fight the virus [35].
Three of the most important pro-inflammatory cytokines of the innate immune response are IL-1, TNF-α, and IL-6. Tissue macrophages, mast cells, endothelial and epithelial cells are the main sources of these cytokines during the innate immune response. The "cytokine storm" is caused by a sudden sharp increase in the levels of various inflammatory cytokines, including IL-6, IL-1, TNF-α, and interferon (Figure 1).
This increase in cytokine secretion leads to the invasion and migration of various immune cells such as macrophages, neutrophils, and T cells from the bloodstream to the site of infection. Additionally, tissue destruction is associated with endothelial cell instability, vascular barrier damage, alveolar cell damage, destruction of capillaries, and eventually death. Lung damage is one of the consequences of cytokine storms that can turn into acute lung damage or its more severe form acute respiratory distress syndrome (ARDS) [36]. ARDS, which is associated with lower blood oxygen saturation, is a major cause of death in patients with COVID-19. Although the exact mechanism of ARDS in COVID-19 patients is not fully understood, overproduction and secretion of pro-inflammatory cytokines are likely one of the main causes [37].
Evidence suggests that some patients with COVID-19 suffer from a "cytokine storm." Plasma analysis of cytokines in 41 patients with COVID-19 in China revealed high levels of IL-1β, IL-7, IL-8, IL-9, IL-10, FGF, G-CSF, IFN-γ, IP- 10, MCP-1, MIP-1A, MIP1-B, PDGF, TNF-α, and VEGF in ICU and non-ICU patients compared with healthy individuals. All patients included in the study had pneumonia, of which 1/3 patients were admitted to the intensive care unit and 6 of these patients died [38].
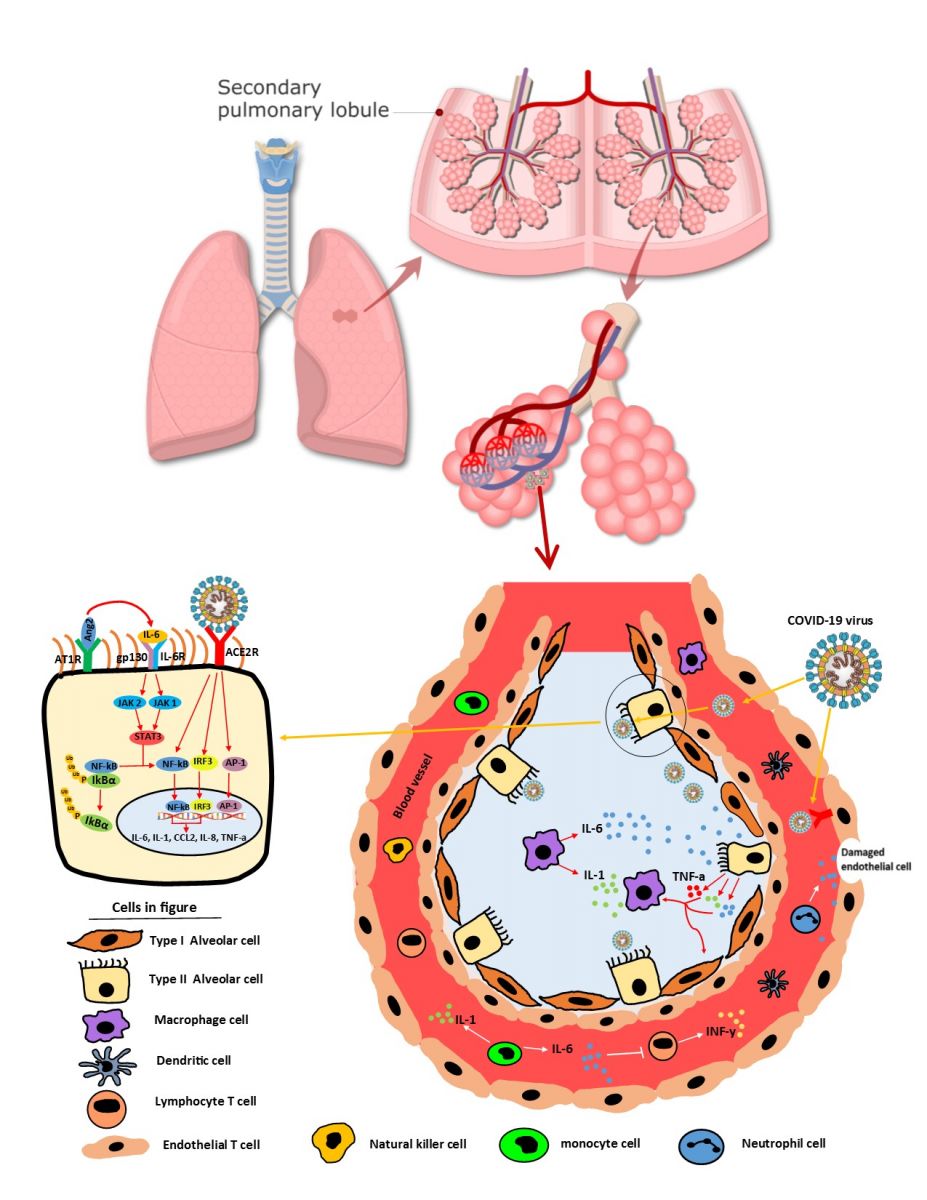
Figure 1: The process of creating a cytokine storm following the infection of lung cells with the Covid-19 virus. SARS-CoV-2 infects epithelial cells and immune cells, causing tissue damage and the release of inflammatory cytokines (such as IL-1, IL-6, and TNFα) by endothelial, epithelial, and immune cells. These inflammatory cytokines overwhelm innate immune cells (monocytes, macrophages, neutrophils, DCs, and NK cells) and adaptive immune cells (CD4 + T cells and CD8 + T cells) to the site of injury and cause storms. Overproduction of systemic cytokines activates macrophages and erythrophagocytosis, which cause anemia and impaired vascular homeostasis, resulting in capillary leakage syndrome and thrombosis. Together, these events lead to ARDS, multiple organ failure, and eventually death.
Numerous studies have reported that high levels of pro-inflammatory cytokines are produced as a result of interference between epithelial cells and immune cells in COVID-19, resulting in severe cytokine (CS) storms [39]. CS is a life-threatening vital condition that requires hospitalization in intensive care and has a very high mortality rate. CS is characterized by the clinical manifestations of severe systemic inflammation, hyperferritinemia, hemodynamic instability, and multiple organ failure, and can lead to death if left untreated [40]. CS stimulus is an uncontrolled immune response that leads to the activation and proliferation of lymphocytes, macrophages and other immune cells. Clinical findings of CS have been attributed to the function of pro-inflammatory cytokines such as IL-1, IL-6, IL-18, IFN-γ and TNF-α [41]. In the serum of CS patients, both pro-inflammatory cytokines (such as IL-1, IL-6 and TNF-α) and anti-inflammatory cytokines (such as IL-10 and the IL-1 receptor antagonist) are elevated. The main factors causing hurricane cytokines are IL-6 and TNF-α. In case of the lack of immediate and appropriate treatment for CS, patients will develop ARDS, which is associated with acute lung injury followed by multiple organ failure and death [42]. In addition to antiviral therapies that can directly target the virus, anti-inflammatory therapies that reduce cytokine responses are recommended to reduce morbidity and mortality in COVID-19 patients.
Immunomodulatory therapeutics
Given that there is no approved drug treatment for SARS-CoV-2 infection, vaccination seems to be the main prevention strategy and is ideal for meeting the current clinical need [43]. Based on previous epidemic history associated with SARS-CoV and Middle East Respiratory Syndrome (MERS) coronavirus, drugs such as ribavirin, remdesivir and lopinavir/ritonavir have been considered for the treatment of COVID-19 despite their controversial results [44,45]. With the rapid increase in critically ill patients, it is essential to identify specific molecular targets in key pathogenesis pathways that can be manipulated. Using these therapeutic targets to modulate immunity can reduce inflammatory conditions or CRS (cytokine release syndrome) in COVID-19 patients. However, many anti-inflammatory drugs commonly used in the treatment of rheumatic diseases have been suggested as immunomodulatory drugs for the treatment of SARS-CoV-2 [46].
One of these methods is the use of Janus Kinase Inhibitors (JAKi) to over-inhibit cytokine signaling or cytokine storms [47]. Most JAK inhibitors are specifically effective in inhibiting JAK1 and JAK2 (Figure 1), and therefore, multiple cytokines including IL-6, IL-2, interferon alpha and beta (IFN) -α/β, and the IFN signaling cascade [48]. Baricitinib is a JAKi that may inhibit the early stages of SARS-CoV-2 virus transmission through endocytosis and prohibit several cytokines-related signaling pathways that are associated with the pathogenesis of viral pneumonia. These results suggest that JAK inhibitors may be effective in reducing clinical symptoms through modulating inflammatory cytokines in various organs such as the lungs, kidneys, and heart. Several clinical trials have been performed to evaluate the use of Baricitinib and other JAK inhibitors in COVID-19 patients. The results show that patients treated with Baricitinib achieved better clinical improvement than others [49].
Another way is to use renin-angiotensin-aldosterone (RAAS) system inhibitors. Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are primary inhibitors of RAAS [50]. These RAAS inhibitors are recommended for patients with cardiovascular disease, diabetes and renal failure [51]. SARS-CoV-2 enters the cells of the lower respiratory tract of infected patients using membrane-bound protein ACE2 receptor (Figure 1). Therefore, it is hypothesized that treatment with ACEI and ARBs in COVID-19 patients may reduce inflammation and have potential benefits in treating COVID-19-induced lung injury [52].
In COVID-19 infection, phosphorylation and ubiquitination of the NF-κB inhibitor (called IkBα) cause the proteasome of IkBα to be degraded and the NF-κB complex to be isolated and transported to the nucleus (Figure 1). NF-κB then induces several pro-inflammatory cytokines such as TNF-α, IL-1, IL-6 and some chemokines [53]. In response to the production of these inflammatory cytokines, immune cells are recruited to the site of injury increases, which intensifies the inflammatory process and causes severe inflammation or CRS in patients with SARS-CoV-2. NF-κB to remain in binding to IκB and not be able to cross the nuclear membrane and bind to the target DNA, resulting in inhibition of the expression of pro-inflammatory chemokines and cytokines.
IL-6 is a type of cytokine that is involved in a wide range of immune and inflammatory events. IL-6 binds to IL-6R and glycoprotein-130 (gp130) to form a hexameric complex (Figure 1) [54]. Because IL-6 plays a vital role in immune and inflammatory disorders, anti-IL-6 or anti-IL-6R drug therapy can prevent IL-6 binding to IL-6R by targeting the cytokine or receptor itself [55]. Therefore, IL-6 inhibitor-based therapy can relieve various inflammatory symptoms such as fever, fatigue, pain, etc. [55]. It is hypothesized that an IL-6 inhibitor may be an option for the treatment of severe inflammation (due to high concentrations of IL-6) or ARDS due to CRS in patients with COVID-19 pneumonia [56]. In this regard, a phase 2 clinical trial was performed to evaluate the efficacy of an IL-6 inhibitor called Tocilizumab in patients with acute-phase COVID-19 [55]. Clinical trial findings are expected to expand the use of IL-6 inhibitor therapy for the treatment of CRS or inflammatory bowel disease in COVID-19 patients.
Mesenchymal stem cells and their implantation
Within the cell complex in the bone marrow, there is a subset of non-blood cells called mesenchymal progenitor cells. Mesenchymal stem cells are multivalent (multipotent) stem cells that can produce their own (self-renewal) and a copy of themselves to the left and also can be a variety of mesenchymal cell differentiation found [57]. MSCs can be isolated from a variety of sources, including the umbilical cord, adipose tissue, bone marrow, and human dental pulp (Figure 2) [58,59]. The shape of MSC colonies in the culture medium is similar to fibroblast cells and is known as colony-forming unit-fibroblast (CFU-F) [60].
MSCs have several features that can be identified and differentiated from other cells based on surface markers on the surface of these cells and can be examined by flow cytometry [61]. In addition, MSCs can produce different tissues such as bone, cartilage, and fat during in vitro differentiation [62]. MSCs can be differentiated into ectodermal and endodermal cells [63]. This property of ductility along with their easy culture from bone marrow or other tissues and having immunomodulatory potential and lack of moral consequences are the reasons for using MSCs in cell therapy [64].
The implantation process of MSCs involves their migration inside a tissue, following their transfer across the width of the vascular endothelium. There is very little data on the localization and implantation of MSCs after infusion. Several factors play a role in MSC implantation performance [65]. In general, in an inflammatory process during injury, activation of inflammatory cells requires a series of signaling and adhesion events, including selectin-mediated rotation, cell activation by cytokines and chemokines, activation of integrins, and adhesion function by integrins. Endothelium, migration from the endothelial width, and finally migration and invasion of the extracellular matrix include integrin-dependent interactions and matrix-degrading proteases [66]. It has been clearly shown that direct migration of MSCs follows a slope of the chemokine concentration. An increase in the concentration of inflammatory chemokines where inflammation is present is a key mediator for the transport of MSCs to the site of injury.
Chemokines are released after tissue destruction, and MSCs also express several receptors for chemokines [67]. Activation of chemokines is a very important step in the movement of MSCs to the site of injury. During several passages of MSCs cell culture, the expression of the number of surface receptors such as CXCR3, CXCR4, CXCR6, CCR9, and CCR10 is increased or decreased, which may contribute to the implantability of MSCs. Among these, CXCR4 is a chemotactic receptor for SDF-1 whose expression is increased in the bone marrow and damaged tissue [68]. The binding of SDF-1 to the CXCR4 receptor on the surface of MSCs activates mesenchymal cells to increase their proliferation, survival, and migration to the affected site (Figure 2). As long as the SDF-1 chemotaxis factor is produced from the affected site, the process of activating and recalling MSCs continues until the complete repair of the damaged tissue, but in cases of severe damage, the repair is not complete [69].
MSCs secrete many molecules such as growth factors, cytokines, chemokines, and hormones that are involved in cellular function, all of which have paracrine effects on immune cells and play a role in their implantation and migration to the damaged site [70]. Factors such as IL-37, TGF-β, VEGF (Vascular endothelial growth factor), PGE-2 (Prostaglandin-E2), HGF (Hepatocyte growth factor), NO (Nitric oxide), and HO-1 (Heme oxygenase) are secreted by MSCs and can provide an immunosuppressive environment by inhibiting T cell proliferation, cytotoxicity, and induction of Treg cell proliferation [71]. MSCs changed the cytokine secretion by dendritic cells (DCs), helper T cells, and NK cells by inhibiting the secretion of pro-inflammatory cytokines such as interferon-gamma (IFN-γ), IL-1β, and tumor necrosis factor (TNF-α) and alter the increase anti-inflammatory cytokines such as IL-10 [85]. IL-10 inhibits apoptosis and reduces the production and activation of lymphocytes [72]. IDO factor (indoleamine 2,3 dioxygenase) also has a regulatory effect on T cell proliferation and Treg cells [73]. Keratinocyte growth factor (KGF) causes progenitor cells to accumulate and repair the epithelium very quickly and plays an important role in repairing the precursor epithelial cell located in the affected area, especially the type II alveolar epithelial cells (Figure 2) [74].
Studies have shown that MSCs can reduce innate immune responses and have the ability to alter adaptive immune responses associated with inflammatory lung disease by affecting T-cells [75].
Preclinical models support the hypothesis that MSCs may have clinical efficacy in the treatment of COPD. However, although clinical trials have demonstrated the safety of MSC therapy, they have not yet provided evidence for the efficacy of MSCs in the treatment of COPD [76]. Many studies have been conducted so far to investigate the safety of MSC-based therapies. Clinical trials show that human MSCs cultured in vitro are less prone to adverse changes [77]. Prolonged cell culture may lead to an increased likelihood of malignant transformation. Some components of the culture medium and growth factors may predispose the cells to such processes. There is also a risk of viral and prion transmission after administration of the cells [78].In addition to transient fever, which is the most common event, reported by researchers, other side effects such as constipation, fatigue, injection site side effects, and insomnia can also occur with MSC administration [79].
Mesenchymal stem cells cause the virus shedding and prevent virus replication and damage to the virus-induced lung epithelial cells (Figure 2) [17].Thus, mesenchymal stem cells may be an appropriate treatment option for patients with severe or critical COVID-19 that could potentially improve lung damage, suppress overactive inflammatory response, and influence the progression of pulmonary fibrosis (Figure 2). In both animal and human models, treatment with MSC has been observed to reduce lung lesions and inhibit the inflammatory response induced by influenza virus infection [80,81]. The efficacy and potential safety of MSC treatment in patients with ARDS have also been evaluated [82].
Figure 2: Proposed mechanisms for MSC function in patients with severe COVID-19. Mesenchymal cells can be isolated from different tissues and after processing, the cells injected intravenously. The number of infiltrated immune cells that cause the cytokine storm is significantly reduced and the damaged lung tissue is repaired. Mesenchymal stem cells are involved in the regeneration and regulation of the immune system, but the exact mechanisms of these effects have not yet been fully elucidated.
MSC Therapy Clinical Trials for SARS-CoV-2
Clinical trials have shown that intravenous MSC injections in patients with moderate or severe SARS-CoV-2 have been safe and well tolerated. Zhao et al. reported for the first-time intravenous administration of MSCs could improve the clinical outcome of COVID-19 patients and at the same time showed appropriate levels of immune tolerance, especially in critically ill patients [83]. Shi et al. conducted a randomized, phase 2, double-blind, placebo-controlled trial to evaluate the efficacy and safety of intravenous MSC treatment at two hospitals in Wuhan, China. 101 patients with severe COVID-19 were selected and randomly selected in a 2:1 ratio to receive UC-MSCs (placebo) or placebo. Compared with placebo, UC-MSC injection improved lung lesion volume from the start of injection to 28 days after injection [84]. Also, a significant improvement was observed in the gait test within 6 minutes (6MWD). In another study, umbilical cord MSC (UC-MSC) injections in patients with moderate to severe COVID-19 were safe, paving the way for phase 2 and 3 trials [85]. In two studies, the effectiveness of treatment using 2×108 MSC [86] and exogenous MSC-derived exosomes [87] in COVID-19 patients was evaluated and showed improvement in some clinical parameters. Lanzoni et al. found that the level of inflammatory cytokines was significantly reduced 6 days after UC-MSC injection. Moreover, an improvement was observed in survival without serious side effects in COVID-19 patients with ARDS [88]. In other trials, patients treated with MSC were discharged earlier due to improved pulmonary function than control patients [89]. Wu et al. Showed that fibrotic lung lesions decreased with MSC injection in pulmonary patients [90]. These data suggest that treatment with MSC is safe and may be beneficial for COVID-19 patients. Table 1 show several completed clinical trials related to the use of MSCs in the treatment of SARS-CoV-2-induced lung injury and their effectiveness at clinicaltrials.gov.
Table 1: Clinical studies of the treatment of SARS-CoV-2 patients with MSC taken from clinicaltrials.gov site.
|
Trial ID |
Trial design |
Cellular source |
Injection dose |
Number |
Clinical findings |
|
NCT04392778 [91] |
Phase I and II |
MSCs |
3×106 cell/dose 3 injections (0-3-6 days) |
30 |
Improve clinical signs associated with COVID-19 infection (including fever, pneumonia, shortness of breath). Improvement in the lungs was assessed by CT scan. |
|
NCT04400032 [92] |
Phase I and II |
UC-MSCs |
2.5×106 cell/ dose |
15 |
Umbilical Cord (UC) cells were safe and had no side effects. Survival rates increased in ARDS patients. |
|
NCT04348461 [93] |
Phase I |
AD-MSCs |
1×106 cell/kg 3 injections |
13 |
No adverse events were reported after injection of adipose-derived MSCs (AD). Improvements in respiratory parameters, pulmonary imaging and reduction of inflammation were observed in individuals with severe pulmonary symptoms. |
|
NCT04355728 [94] |
Phase I and II |
UC-MSCs |
2×107 cell/dose 2 injections (0-3 days) |
24 |
UC-MSC injection was safe. Inflammatory cytokines were significantly reduced and the survival rate of ARDS patients was increased. |
|
NCT04288102 [84] |
Phase II |
UC-MSCs |
4×107 cell/dose 3 injections (0-3-6 days) |
100 |
UC-MSCs were safe to administer and improved lung damage compared with those receiving placebo. Improvements were observed in the 6MWD test in patients treated with UC-MSC. |
|
NCT04713878 [95] |
Phase I I |
MSCs |
1×106 cell/kg 3 injections (0-2-4 days) |
21 |
Improve clinical symptoms, reduce cytokine storm damage to tissues and organs, and meet oxygen demand |
|
NCT04252118 [96] |
Phase I |
MSCs |
3×107 cell/dose 3 injections (0-3-6 days) |
20 |
Improve clinical symptoms including duration of fever and shortness of breath, no side effects |
|
Trial ID |
Trial design |
Cellular source |
Injection dose |
Number |
Clinical findings |
|
NCT04348435 [97] |
Phase II |
Allogeneic MSCs |
×107 cell/dose2 5 injections (0-2-6 10-14 days) |
55 |
Allogeneic MSC injection was safe. No upper / lower respiratory infection was observed. |
|
NCT04339660 [98] |
Phase I and II |
UC-MSCs |
1×106 cell/kg |
30 |
No side effects have been reported. Reduction of inflammation was observed in individuals with severe pulmonary symptoms. |
|
NCT04535856 [99] |
Phase I |
Allogeneic MSCs |
1×108 cell/ dose 5×107 cell/dose |
9 |
No side effects have been reported. Reduction of inflammation was observed in individuals with severe pulmonary symptoms. |
|
NCT04522986 [100] |
Phase I |
AD-MSCs |
1×106 cell/dose 4 injections |
6 |
AD-MSC injection was safe. Decreased pneumonia associated with patient survival. |
|
NCT04252118 [85] |
Phase I |
UC-MSCs |
3×107 cell/dose 3 injections (0-3-6 days) |
18 |
Intravenous injection of UC-MSCs was moderate and severely safe in COVID-19 patients. No side effects of the injection were observed. |
|
NCT04625738 [101] |
Phase II |
WJ-MSCs |
2×106 cell/kg 3 injections (0-3-6 days) |
30 |
Wharton's Jelly injection had no side effects. Improve respiratory symptoms by increasing the number of days without artificial oxygen and reducing the number of days hospitalized |
|
NCT04349631 [102] |
Phase II |
AD-MSCs |
1×106 cell/kg |
56 |
Improve upper / lower respiratory infection based on hospitalization criteria |
l
DISCUSSION
COVID-19 has imposed a great deal of public health and socioeconomic burden, especially in low and middle-income countries. There is an urgent global need for safe and effective treatments. The therapeutic effects of MSCs in animal and human models of various diseases reflect the therapeutic applications of these cells. The immunomodulatory and growth inhibitory properties of MSCs have led to their normal use in tissue repair and treatment of various diseases in the preclinical stages and study phases 1 to 3 [103-105]. Among the advantages of using the cell therapy method compared to other methods, the harmlessness of its side effects compared to conventional drug treatment methods, and also compared to transplantation and transplant rejection complications, the method is safer and cheaper. Studies over the past decade have shown that MSCs are highly ductile and can differentiate into bronchial, alveolar, vascular epithelium, and interstitial cell types [105]. Numerous studies have shown that change in cell transformation in normal lungs is relatively small but increases when cell proliferation is impaired [106-108]. Normally in the lungs, adult stem cells are located in special areas called niches that are needed for the survival of lung tissue homeostasis.
The results of two clinical trials showed that mesenchymal stem cells and their EVs (extracellular vesicles) effectively suppress harmful immune responses in the lungs, reduce persistent inflammation, and significantly reduce respiratory function in patients with ARDS [83,87]. Most importantly, exacerbation of COVID-19-associated symptoms and side effects associated with MSC or MSC-Exos injection have not been reported, suggesting that MSCs and EVs are a safe and effective treatment approach for patients with SARS-CoV-2. Despite these promising results, it should be noted that the safety and efficacy of MSCs or MSC-EVs in both studies were evaluated in a small number of COVID-19 patients. Sengupta et al. examined the therapeutic potential of MSC-Exos in 24 patients and showed that MSC-Exos was not able to improve respiratory function in patients with SARS-CoV-2 [87]. According to these results, more research should be done with more patients to decide on the effectiveness of MSC and its products for the treatment of SARS-CoV-2.
The ability of stem cells to be located in the lungs and to adapt to epithelial cells is one of the most challenging topics in recent years [109,110]. It is hoped that bone marrow-derived cells can be isolated, cultured, manipulated ex vivo, and then released into the lung to repair damaged lung tissue. It is assumed that injecting mesenchymal stem cells and replacing them with damaged progenitor cells, it produces functional epithelial cells that can prevent airway remodeling and provided a stable condition for proper epithelial cell proliferation. Transformation of bone marrow-derived cells into the airway and alveolar epithelial cells is rare and therefore further studies on the effective efficacy of cell therapy are needed.
As MSCs provide a new tool for the treatment of various human diseases, more knowledge of the MSCs ability to suppress immunity seems essential, while MSCs can undergo spontaneous mutations and show tumorigenic potential [111]. Although the use of MSCs has reduced the severity of the disease, long-term data on the safety of this treatment are needed. Further information is needed on the functional differences and proliferative characteristics of MSCs derived from bone marrow or adipose tissue obtained from sick versus healthy individuals. The use of high-safety conditions for mesenchymal stem cell culture is essential to prevent the transmission of viral and prion infections to cell recipients [112]. In addition, the use of allogeneic MSCs may have potential risk for infections acquired from the donor. Therefore, it is necessary to study all phenotypic features of MSCs to facilitate pre-clinical studies with good design to better achieve its clinical applications. Although there is a potential risk in the human application of MSCs, due to the modulatory properties of MSCs for the treatment of inflammatory and immune-related diseases, it can be considered a great dream and promise shortly to be able to it was used as a complementary treatment based on repair, modulation of the immune system and reduction of inflammation to improve the damage caused by SARS-CoV-2 and similar viruses.
DECLARATION
Ethics Approval and Consent to Participate
Not applicate
Consent for Publication
Not all authors have a problem publishing an article
Availability of Data and Materials
All data generated or analyzed during this study are included in the present published article and its supplementary information file.
Competing Interests
The authors declare that they have no competing interests.
Authors' Contributions
The concept and the design of the study were developed by Aram Asareh Zadegan Dezfuli. The methodology was designed by Saeed Rahmanzadeh. The original draft was prepared by Amir Nejad-Moghaddam and reviewed by Amir Nejad-Moghaddam.
Acknowledgments
This project was supported by Marine Medicine Research Center, Baqiyatallah University of Medical Sciences.
Disclosure Statement
All the authors have read and approved the final version of the manuscript. The authors confirm that there are no conflicts of interest
REFERENCES
- Yao SY, Lei CQ, Liao X, Liu RX, Chang X, Liu ZM. (2021). Integrated chinese and Western medicine in treatment of critical coronavirus disease (COVID-19) patient with endotracheal intubation:a case report. Chin J Integr Med. 27(4):300.
- Petersen E, Koopmans M, Go U, Hamer DH, Petrosillo N, Castelli F, et al. (2020). Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis. 20(9):e238-e244.
- Song JW, Zhang C, Fan X, Meng FP, Xu Z, Xia P, et al. (2020). Immunological and inflammatory profiles in mild and severe cases of COVID-19. Nat Commun. 11(1):3410.
- Hu Y, Wang T, Hu Z, Wang X, Zhang Z, Li L, et al. (2020). Clinical efficacy of glucocorticoid on the treatment of patients with COVID-19 pneumonia:a single-center experience. Biomed Pharmacother. 130:110529.
- Han D, Peng C, Meng R, Yao J, Zhou Q, Xiao Y, et al. (2020). Estimating the release of inflammatory factors and use of glucocorticoid therapy for COVID-19 patients with comorbidities. Aging (Albany NY). 12(22):22413.
- Duan K, Liu B, Li C, Zhang H, Yu T, Qu J, et al. (2020). Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci U S A. 117(17):9490-9496.
- Zhao Q, He Y. (2020). Challenges of convalescent plasma therapy on COVID-19. J Clin Virol. 127:104358.
- Ameratunga R, Woon ST, Lea E, Steele R, Lehnert K, Leung E, et al. (2022). The (apparent) antibody paradox in COVID-19. Expert Rev Clin Immunol. 18(4):335-345.
- Pecetta S, Finco O, Seubert A. (2020). Quantum leap of monoclonal antibody (mAb) discovery and development in the COVID-19 era. Semin Immunol. 50:101427.
- Winkler ES, Gilchuk P, Yu J, Bailey AL, Chen RE, Chong Z, et al. (2021). Human neutralizing antibodies against SARS-CoV-2 require intact Fc effector functions for optimal therapeutic protection. Cell. 184(7):1804-1820.
- Nie M, Chen G, Zhao C, Gan J, Alip M, Zhao Y, et al. (2021). Bio-inspired adhesive porous particles with human MSCs encapsulation for systemic lupus erythematosus treatment. Bioact Mater. 6(1):84-90.
- Ringden O, Keating A. (2011). Mesenchymal stromal cells as treatment for chronic GVHD. Bone Marrow Transplant. 46(2):163-164.
- Weiss DJ, Casaburi R, Flannery R, LeRoux-Williams M, Tashkin DP, et al. (2013). A placebo-controlled, randomized trial of mesenchymal stem cells in COPD. Chest. 143(6):1590-1598.
- Yao Y, Fan XL, Jiang D, Zhang Y, Li X, Xu ZB, et al. (2018). Connexin 43-mediated mitochondrial transfer of iPSC-MSCs alleviates asthma inflammation. Stem Cell Reports. 11(5):1120-1135.
- Nejad-Moghaddam A, Ajdari S, Tahmasbpour E, Goodarzi H, Panahi Y, Ghanei M. et al. (2017). Adipose-derived mesenchymal stem cells for treatment of airway injuries in a patient after long-term exposure to sulfur mustard. Cell Journal (Yakhteh). 19(1):117.
- Marzouni ET, Dorcheh SP, Nejad-Moghaddam A, Ghanei M, Goodarzi H, et al. (2020). Adipose-derived mesenchymal stem cells ameliorate lung epithelial injury through mitigating of oxidative stress in mustard lung. Regen Med. 15(7):1861-1876.
- Khatri M, Richardson LA, Meulia T. (2018). Mesenchymal stem cell-derived extracellular vesicles attenuate influenza virus-induced acute lung injury in a pig model. Stem Cell Res Ther. 9(1):1-13.
- Darwish I, Banner D, Mubareka S, Kim H, Besla R, Kelvin DJ, et al. (2013). Mesenchymal stromal (stem) cell therapy fails to improve outcomes in experimental severe influenza. PLoS One. 8(8):e71761.
- Loy H, Kuok DIT, Hui KPY, Choi MHL, Yuen W, Nicholls JM, et al. (2019). Therapeutic implications of human umbilical cord mesenchymal stromal cells in attenuating influenza A (H5N1) virus–associated acute lung injury. J Infect Dis. 219(2):186-196.
- Walter J, Ware LB, Matthay MA. (2014). Mesenchymal stem cells:mechanisms of potential therapeutic benefit in ARDS and sepsis. Lancet Respir Med. 2(12):1016-1026.
- Wilson JG, Liu KD, Zhuo H, Caballero L, McMillan M, Fang X, et al. (2015). Mesenchymal stem (stromal) cells for treatment of ARDS:a phase 1 clinical trial. Lancet Respir Med. 3(1):24-32.
- https://clinicaltrials.gov/ct2/results. mesenchymal stem cell | COVID-19. november 2021.
- Stanley AC, Lacy P. (2010). Pathways for cytokine secretion. Physiology. 2010. 25(4):218-229.
- Zhang X, Li S, Niu S. (2020). ACE2 and COVID-19 and the resulting ARDS. Postgrad Med J. 96(1137):403-407.
- Zhao J, He S, Minassian A, Li J, Feng P. (2015). Recent advances on viral manipulation of NF-κB signaling pathway. Curr Opin Virol. 15:103-111.
- Varagic J, Ahmad S, Nagata S, Ferrario CM. (2014). ACE2:angiotensin II/angiotensin-(1–7) balance in cardiac and renal injury. Curr Hypertens Rep. 16(3):420.
- Benigni A, Cassis P, Remuzzi G. (2010). Angiotensin II revisited:new roles in inflammation, immunology and aging. EMBO Mol Med. 2(7):247-257.
- Murakami M, Kamimura D, Hirano T. (2019). Pleiotropy and specificity: insights from the interleukin 6 family of cytokines. Immunity. 50(4):812-831.
- Wang Y, van Boxel-Dezaire AH, Cheon H, Yang J, Stark GR. (2013). STAT3 activation in response to IL-6 is prolonged by the binding of IL-6 receptor to EGF receptor. Proc Natl Acad Sci U S A. 110(42):16975-16980.
- Braciale TJ, Hahn YS. (2013). Immunity to viruses. Immunol Rev. 255(1):5-12.
- Hu B, Huang S, Yin L. (2021). The cytokine storm and COVID‐19. J Med Virol. 93(1):250-256.
- Menezes MCS, Veiga ADM, Martins de Lima T, Kunimi Kubo Ariga S, Vieira Barbeiro H, de Lucena Moreira C, et al. (2021). Lower peripheral blood Toll-like receptor 3 expression is associated with an unfavorable outcome in severe COVID-19 patients. Sci Rep. 11(1):1-12.
- Mukundan H, Kubicek-Sutherland JZ, Stromberg Z, Stromberg LR. (2021). Fieldable Optical Biosensors with Integrated Sample Processing for Universal Surveillance and Diagnostics–Application to COVID-19. in ECS Meeting Abstracts. 2021. IOP Publishing.
- Zhou R, Liu L, Wang Y. (2021). Viral proteins recognized by different TLRs. J Med Virol. 93(11):6116-6123.
- Thompson MR, Kaminski JJ, Kurt-Jones EA, Fitzgerald KA. (2011). Pattern recognition receptors and the innate immune response to viral infection. Viruses. 3(6):920-940.
- Hou QQ, Ge H, Gao YM. (2019). Cytokines in cytokine storm syndrome. Cytokine Storm Syndrome. 2019:197-207.
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. (2020). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 55(3):105924.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 395(10223):497-506.
- Ragab D, Salah Eldin H, Taeimah M, Khattab R, Salem R. (2020). The COVID-19 cytokine storm; what we know so far. Front Immunol. 2020:1446.
- Caricchio R, Gallucci M, Dass C, Zhang X, Gallucci S, Fleece D, et al. (2021). Preliminary predictive criteria for COVID-19 cytokine storm. Ann Rheum Dis. 80(1):88-95.
- Yang L, Xie X, Tu Z, Fu J, Xu D, Zhou Y. (2021). The signal pathways and treatment of cytokine storm in COVID-19. Signal Transduct Target Ther. 6(1):1-20.
- Shcherbak SG, Anisenkova AY, Mosenko SV, Glotov OS, Chernov AN, Apalko SV, et al. (2021). Basic predictive risk factors for cytokine storms in COVID-19 patients. Front Immunol. 12.
- Tu YF, Chien CS, Yarmishyn AA, Lin YY, Luo YH, Lin YT, et al. (2020). A review of SARS-CoV-2 and the ongoing clinical trials. Int J Mol Sci. 21(7):2657.
- Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, Brown AJ, et al. (2020). Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS-CoV. Nat Commun. 11(1):222.
- Khalili JS, Zhu H, Mak NSA, Yan Y, Zhu Y. (2020). Novel coronavirus treatment with ribavirin: groundwork for an evaluation concerning COVID‐19. J Med Virol. 92(7):740-746.
- Gianfrancesco MA, Hyrich KL, Gossec L, Strangfeld A, Carmona L, Mateus EF, et al. (2020). Rheumatic disease and COVID-19:initial data from the COVID-19 global rheumatology alliance provider registries. Lancet Rheumatol. 2(5):e250-e253.
- Seif F, Aazami H, Khoshmirsafa M, Kamali M, Mohsenzadegan M, Pornour M, et al. (2020). JAK inhibition as a new treatment strategy for patients with COVID-19. Int Arch Allergy Immunol. 181(6):467-475.
- Morinobu A. (2020). JAK inhibitors for the treatment of rheumatoid arthritis. Immunological Med. 43(4):148-155.
- Spinelli FR, Conti F, Gadina M. (2020). HiJAKing SARS-CoV-2? The potential role of JAK inhibitors in the management of COVID-19. Sci Immunol. 5(47):eabc5367.
- Quinn KL, Fralick M, Zipursky JS, Stall NM. (2020). Renin–angiotensin–aldosterone system inhibitors and COVID-19. CMAJ. 192(20):E553-E554.
- Ma TK, Kam KK, Yan BP, Lam YY. (2010). Renin–angiotensin–aldosterone system blockade for cardiovascular diseases:current status. Br J Pharmacol. 160(6):1273-1292.
- Saavedra JM. (2020). Angiotensin receptor blockers and COVID-19. Pharmacol Res. 156:104832.
- Sehnert B, Burkhardt H, Dübel S, Voll RE. (2020). Cell-type targeted NF-kappaB inhibition for the treatment of inflammatory diseases. Cells. 9(7):1627.
- Heo TH, Wahler J, Suh N. (2016). Potential therapeutic implications of IL-6/IL-6R/gp130-targeting agents in breast cancer. Oncotarget. 7(13):15460.
- Choy EH, De Benedetti F, Takeuchi T, Hashizume M, John MR, Kishimoto T. (2020). Translating IL-6 biology into effective treatments. Nat Rev Rheumatol. 16(6):335-345.
- Liu B, Li M, Zhou Z, Guan X, Xiang Y. (2020). Can we use interleukin-6 (IL-6) blockade for coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? J Autoimmun. 111:102452.
- Mareschi K, Biasin E, Piacibello W, Aglietta M, Madon E, Fagioli F. (2001). Isolation of human mesenchymal stem cells:bone marrow versus umbilical cord blood. Haematologica. 86(10):1099-1100.
- Nejad-Moghaddam A, Panahi Y, Abdollahpour Alitappeh M, Borna H, Shokrgozar MA, Ghanei M. (2015). Therapeutic potential of mesenchymal stem cells for the treatment of airway remodeling in pulmonary diseases. Iran J Allergy Asthma Immunol. 14(6):552-568.
- Nejad-Moghaddam A, Tahmasbpour E, Sohrabiyan M, Jafari H, Ghanei M. (2018). Stem cells therapy:a review on approaches that can be used for treatment of respiratory failures in sulfur mustard-injured patients. Immunopharmacol Immunotoxicol. 40(5):359-367.
- Bianco P, Riminucci M, Gronthos S, Robey PG. (2001). Bone marrow stromal stem cells:nature, biology, and potential applications. Stem cells. 19(3):180-192.
- Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, et al. (2006). Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 8(4):315-317.
- da Silva Meirelles L, Caplan AI, Nardi NB. (2008). In search of the in vivo identity of mesenchymal stem cells. Stem cells. 26(9):2287-2299.
- Sato T, Hidaka K, Iwanaga A, Ito M, Asano M, Nakabeppu Y, et al. (2005). Impairment of cardiomyogenesis in embryonic stem cells lacking scaffold protein JSAP1. Biochem Biophys Res Commun. 338(2):1152-1157.
- Le Blanc K, Ringdén O. (2007). Immunomodulation by mesenchymal stem cells and clinical experience. J Intern Med. 262(5):509-525.
- Nejad-Moghaddam A, Ajdary S, Tahmasbpour E, Rad FR, Panahi Y, Ghanei M. (2016). Immunomodulatory properties of mesenchymal stem cells can mitigate oxidative stress and inflammation process in human mustard lung. Biochem Genet. 54(6):769-783.
- Löbel M, Bauer S, Meisel C, Eisenreich A, Kudernatsch R, Tank J, et al. (2012). CCN1:a novel inflammation-regulated biphasic immune cell migration modulator. Cellular and Molecular Life Sciences. 69(18):3101-3113.
- Cuesta-Gomez N, Graham GJ, Campbell JDM. (2021). Chemokines and their receptors:Predictors of the therapeutic potential of mesenchymal stromal cells. Journal of Translational Medicine. 19(1):1-10.
- Kallmeyer K, Pepper MS. (2015). Homing properties of mesenchymal stromal cells. Taylor & Francis:477-479.
- Marquez-Curtis LA, Janowska-Wieczorek A. (2013). Enhancing the migration ability of mesenchymal stromal cells by targeting the SDF-1/CXCR4 axis. Biomed Res Int. 2013:561098.
- Von Lüttichau I, Notohamiprodjo M, Wechselberger A, Peters C, Henger A, Seliger C, et al. (2005). Human adult CD34− progenitor cells functionally express the chemokine receptors CCR1, CCR4, CCR7, CXCR5, and CCR10 but not CXCR4. Stem cells and development. 14(3):329-336.
- Meirelles Lda S, Fontes AM, Covas DT, Caplan AI. (2009). Mechanisms involved in the therapeutic properties of mesenchymal stem cells. Cytokine Growth Factor Rev. 20(5-6):419-427.
- Németh K, Leelahavanichkul A, Yuen PS, Mayer B, Parmelee A, Doi K, et al. (2009). Bone marrow stromal cells attenuate sepsis via prostaglandin E2–dependent reprogramming of host macrophages to increase their interleukin-10 production. Nat Med. 15(1):42-49.
- Ling W, Zhang J, Yuan Z, Ren G, Zhang L, Chen X, et al. (2014). Mesenchymal Stem Cells Use IDO to Regulate Immunity in Tumor Microenvironment IDO-Expressing Murine MSCs and Tumor Immunity. Cancer Res. 74(5):1576-1587.
- Lee JW, Fang X, Gupta N, Serikov V, Matthay MA. (2009). Allogeneic human mesenchymal stem cells for treatment of E. coli endotoxin-induced acute lung injury in the ex vivo perfused human lung. Proc Natl Acad Sci U S A. 106(38):16357-16362.
- Abreu SC, Antunes MA, Xisto DG, Cruz FF, Branco VC, Bandeira E, et al. (2017). Bone marrow, adipose, and lung tissue-derived murine mesenchymal stromal cells release different mediators and differentially affect airway and lung parenchyma in experimental asthma. Stem Cells Transl Med. 6(6):1557-1567.
- Broekman W, Khedoe PPSJ, Schepers K, Roelofs H, Stolk J, Hiemstra PS. (2018). Mesenchymal stromal cells:a novel therapy for the treatment of chronic obstructive pulmonary disease? Thorax. 73(6):565-574.
- Musiał-Wysocka A, Kot M, Majka M. (2019). The Pros and Cons of Mesenchymal Stem Cell-Based Therapies. Cell Transplant. 28(7):801-812.
- Chen G, Yue A, Ruan Z, Yin Y, Wang R, Ren Y, et al. (2014). Monitoring the biology stability of human umbilical cord-derived mesenchymal stem cells during long-term culture in serum-free medium. Cell Tissue Bank. 15(4):513-521.
- Wang Y. (2021). The safety of MSC therapy over the past 15 years: a meta-analysis. Stem Cell Res Ther. 12(1):545.
- Chen J, Hu C, Chen L, Tang L, Zhu Y, Xu X, et al. (2020). Clinical study of mesenchymal stem cell treatment for acute respiratory distress syndrome induced by epidemic influenza A (H7N9) infection:a hint for COVID-19 treatment. Engineering. 6(10):1153-1161.
- Chan MC, Kuok DI, Leung CY, Hui KP, Valkenburg SA, Lau EH, et al. (2016). Human mesenchymal stromal cells reduce influenza A H5N1-associated acute lung injury in vitro and in vivo. Proc Natl Acad Sci U S A. 113(13):3621-3626.
- Zheng G, Huang L, Tong H, Shu Q, Hu Y, Ge M, et al. (2014). Treatment of acute respiratory distress syndrome with allogeneic adipose-derived mesenchymal stem cells:a randomized, placebo-controlled pilot study. Respir Res. 15(1):1-10.
- Leng Z, Zhu R, Hou W, Feng Y, Yang Y, Han Q, et al. (2020). Transplantation of ACE2-mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging Dis. 11(2):216.
- Shi L, Huang H, Lu X, Yan X, Jiang X, Xu R, et al. (2021). Effect of human umbilical cord-derived mesenchymal stem cells on lung damage in severe COVID-19 patients:a randomized, double-blind, placebo-controlled phase 2 trial. Signal transduction and targeted therapy, 6(1):1-9.
- Meng F, Xu R, Wang S, Xu Z, Zhang C, Li Y, et al. (2020.). Human umbilical cord-derived mesenchymal stem cell therapy in patients with COVID-19: a phase 1 clinical trial. Signal transduction and targeted therapy. 5(1):1-7.
- Hashemian SR, Aliannejad R, Zarrabi M, Soleimani M, Vosough M, Hosseini SE, et al. (2021). Mesenchymal stem cells derived from perinatal tissues for treatment of critically ill COVID-19-induced ARDS patients:a case series. Stem Cell Res Ther. 12(1):1-12.
- Sengupta V, Sengupta S, Lazo A, Woods P, Nolan A, Bremer N. (2020). Exosomes derived from bone marrow mesenchymal stem cells as treatment for severe COVID-19. Stem cells and development. 29(12):747-754.
- Lanzoni G, Linetsky E, Correa D, Messinger Cayetano S, Alvarez RA, Kouroupis D, et al. (2021). Umbilical cord mesenchymal stem cells for COVID-19 acute respiratory distress syndrome:A double-blind, phase 1/2a, randomized controlled trial. Stem Cells Transl Med. 10(5):660-673.
- Shu L, Niu C, Li R, Huang T, Wang Y, Huang M, et al. (2020). Treatment of severe COVID-19 with human umbilical cord mesenchymal stem cells. Stem Cell Res Ther. 11(1):1-11.
- Wu J, Zhou X, Tan Y, Wang L, Li T, Li Z, et al. (2020). Phase 1 trial for treatment of COVID‐19 patients with pulmonary fibrosis using hESC‐IMRCs. Cell Prolif. 53(12):e12944.
- Clinical Use of Stem Cells for the Treatment of Covid-19. https://clinicaltrials.gov/ct2/show/NCT04392778. 2021.
- Cellular Immuno-Therapy for COVID-19 Acute Respiratory Distress Syndrome (CIRCA-19). https://clinicaltrials.gov/ct2/show/NCT04400032.2021.
- Sánchez-Guijo F, García-Arranz M, López-Parra M, Monedero P, Mata-Martínez C, Santos A, et al. (2020). Adipose-derived mesenchymal stromal cells for the treatment of patients with severe SARS-CoV-2 pneumonia requiring mechanical ventilation. A proof of concept study. EClinicalMedicine. 25:100454.
- Lanzoni G, Linetsky E, Correa D, Messinger Cayetano S, Alvarez RA, Kouroupis D, et al. (2021). Umbilical cord mesenchymal stem cells for COVID‐19 acute respiratory distress syndrome:A double‐blind, phase 1/2a, randomized controlled trial. Stem Cells Transl Med. 10(5):660-673.
- Training KSS. (2021). Mesenchymal Stem Cells Therapy in Patients With COVID-19 Pneumonia.
- Mesenchymal Stem Cell Treatment for Pneumonia Patients Infected With COVID-19. https://clinicaltrials.gov/ct2/show/NCT04252118. 2020.
- Biosciences H. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial to Determine the Safety and Efficacy of Hope Biosciences Allogeneic Mesenchymal Stem Cell Therapy (HB-adMSCs) to Provide Protection Against COVID-19. 2020.
- Clinical Research of Human Mesenchymal Stem Cells in the Treatment of COVID-19 Pneumonia. https://clinicaltrials.gov/ct2/show/NCT04339660. 2020.
- Therapeutic Study to Evaluate the Safety and Efficacy of DW-MSC in COVID-19 Patients (DW-MSC). https://clinicaltrials.gov/ct2/show/NCT04535856. 2021.
- An Exploratory Study of ADR-001 in Patients with Severe Pneumonia caused by SARS-CoV-2 infection (COVID-19). 2020.
- Efficacy of Infusions of MSC From Wharton Jelly in the SARS-Cov-2 (COVID-19) Related Acute Respiratory Distress Syndrome (MSC-COVID19). https://clinicaltrials.gov/ct2/show/NCT04625738. 2021.
- Biosciences H. (2020). A Clinical Trial to Determine the Safety and Efficacy of Hope Biosciences Autologous Mesenchymal Stem Cell Therapy (HB-adMSCs) to Provide Protection Against COVID-19.
- Kim Y, Kim H, Cho H, Bae Y, Suh K, Jung J, et al. (2007). Direct comparison of human mesenchymal stem cells derived from adipose tissues and bone marrow in mediating neovascularization in response to vascular ischemia. Cell Physiol Biochem. 20(6):867-876.
- Caimi PF, Reese J, Lee Z, Lazarus HM. (2010). Emerging therapeutic approaches for multipotent mesenchymal stromal cells (MSCs). Current opinion in hematology, 17(6):505.
- García-Gómez I, Elvira G, Zapata AG, Lamana ML, Ramírez M, Castro JG, et al. (2010). Mesenchymal stem cells:biological properties and clinical applications. Expert Opin Biol Ther. 10(10):1453-1468.
- Wilmas KM, Aria AB, Landis LN, Chaitanya SK, Prieto VG, Duvic M. (2022). CD4/CD8 double-negative mycosis fungoides with large cell transformation and involvement of the lungs and leptomeninges. Dermatol Online J. 28.
- Sun W, Liu X, Yang X, Jing X, Duan C, Yang G, et al. (2022). SENP1 regulates the transformation of lung resident mesenchymal stem cells and is associated with idiopathic pulmonary fibrosis progression. Cell Commun Signal. 20(1):1-14.
- Hu L, Wang J, Lin D, Shen Y, Huang H, Cao Y, et al. (2022). Mesenchymal stem cell-derived nanovesicles as a credible agent for therapy of pulmonary hypertension. Am J Respir Cell Mol Biol. 67(1):61-75.
- Wang X, Zhao Y, Li D, Feng Y, Xie Y, Zhou Y, et al. (2021). Intrapulmonary distal airway stem cell transplantation repairs lung injury in chronic obstructive pulmonary disease. Cell proliferation. 54(6):e13046.
- Chan M, Liu Y. (2022). Function of epithelial stem cell in the repair of alveolar injury. Stem Cell Res Ther. 13(1):1-8.
- Sole A, Grossetête S, Heintzé M, Babin L, Zaïdi S, Revy P, et al. (2021). Unraveling Ewing sarcoma tumorigenesis originating from patient-derived Mesenchymal Stem Cells. Cancer Res. 81(19):4994-5006.
- Babu S, Krishnan M, Panneerselvam A, Chinnaiyan M. (2021). Therapeutic Applications of Mesenchymal Stem Cells::A Comprehensive Review. Life Sci. 16(3):323-353.