Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Prevalence and Associated Factors of Burnout among Midwives in Governmental Hospitals, Eastern Amhara, Ethiopia, 2022
Asrat Fenta Amede1,*, Awraris Hailu Bilchut2, Betelhem Bizuneh Teferi3
1Department of HIT, Debre Berhan Health Science College, Ethiopia
2Department of Public Health, Debre Birhan University, Asrat Woldeyes Health Science Campus, Ethiopia
3Department of Midwifery, Debre Berhan Health Science College, Ethiopia
*Corresponding author: Dr. Asrat Fenta Amede, Department of HIT, Debre Berhan Health Science College, Debre Berhan, P.O. Box 37, Ethiopia; Email: [email protected].
Received Date: May 25, 2023
Published Date: June 16, 2023
Citation: Amede AF, et al. (2023). Prevalence and Associated Factors of Burnout among Midwives in Governmental Hospitals, Eastern Amhara, Ethiopia, 2022. Mathews J Psychiatry Ment Health. 8(3):40.
Copyrights: Amede AF, et al. © (2023).
ABSTRACT
Background: Burnout syndrome is emotional exhaustion (EE), depersonalization (DP) and reduces personal accomplishment (PA). Burnout is resulted from long-term exposure to personal and/or work-related stressors and those stressors are negative effect on midwives’ performance of care and mitigate maternal mortality. Profession‐related stress among midwives has deleterious effects on their professional, physical, and psychological health. Objective: The study aims to assess the prevalence and associated factors of burnout among midwives work in East Amhara governmental hospital Ethiopia 2022. Methods: A facility-based cross cross-sectional study design was carried out. Two hundred sixteen (216) study participants were included in this study from 01 March 2021 – 01 May 2021 working in 11 governmental hospitals in North Shoa, 12 governmental hospitals in South Wollow, 6 governmental hospitals in North Wollow, 1 each from Oromia special Zone and Wagehemera Zones governmental hospitals. A simple Random sampling method was used for selection. Structured and pre-test questionnaires were used. The data were cleaned and checked using Epi info version 3.1 and exported to SPSS version 23 for analysis. Hosmer-Lemeshow goodness fit test and multicollinearity were checked. Bi-variable analysis was executed for variables with p-value of < 0.25 and entered into multivariable logistic regression. Multivariate analysis, AOR, 95% CI and p-value <0.05 were used to identify variables which had association with dependant variable. Data was collected through face-to-face interview. A structured questionnaire was adapted from mental health disorder questionnaire developed by Ethiopian psychiatry association. Pre-test of questionnaire was carried out on 1 referral and 1 primary hospital which are all found out of the study area. Ethical approval was obtained from the Research and Publications committee of Department of public health, College of Health Science, Debre Berhan University. Result: From the total respondents, 112(51.9%) midwives were suffered from professional burnout. There were association between burnout and intention to leave their work (AOR=2.320; 95% CI: (1.307, 4.119), shortage of staff member (AOR= 2.00; 95% CI: (1.141, 3.505), conflict with hospital manager (AOR=2.133; 95% CI: (1.189, 3.825) and having one or more children (AOR=3.348; 95% CI: (1.617, 6.930).
Recommendation and Conclusion
Recommendation:
The intention to leave their work should be given due attention by the Regional Health Bureau.
The hospital management should work together with midwives to avoid disagreement and conflict.
Managers in each hospital should work on human resource to avoid work overload among midwives.
Conclusion
The study showed that a higher proportion of midwives were suffered from burnout due to their work and have an intention to leave their work. There were also a significant association between factors.
Keywords: Midwives, burnout, emotional exhaustion, Eastern Amhara.
LIST OF ABBREVIATIONS
BO: Burn out; CBI: Copenhagen Burnout Inventory; DBU: Debre Berhan University; DP: Depersonalization; EE: Emotional Exhaustion; MBI: Maslach Burnout Inventory; MBI-GS: Maslach Burnout Inventory General Survey; MBI-HSS: Maslach Burnout Inventory Human Service Survey; OLBI: Oldenburg Burnout Inventory; PA: Personal Accomplishment; UK: United Kingdom.
INTRODUCTION
Background
'Burnout' was first used in the United States in the late 1960s and early 1970s to describe a state or process of mental exhaustion and also Freudenberg is considered to be the father of burnout syndrome [1,2].
Burnout is a syndrome of emotional exhaustion (EE), depersonalization (DP) and reduced personal accomplishment (PA) which occurs among workers who are involved in close human relationships [3,4]. According to the author, EE is explained when emotional resources are depleted, workers feel that they are no longer able to give of themselves at a psychological level; DP indicates negative, cynical attitudes and feelings about ones clients and correlated with emotional exhaustion; PA are the tendency to evaluate oneself negatively, particularly with regard to ones work with clients and also worker may feel unhappy about themselves and dissatisfied with their accomplishment on the job [3].
As a result of constant burnout, midwives may experience physical, behavioral and psychological signs which vary in symptom and degree from person to person and it usually occurs about one year after someone has begun working in an institution [5,6]. Exhaustion is the central quality of burnout and the most obvious manifestation of this complex syndrome [1]. Burnout is not similar to depression and mood disturbance and also a consequence of one event; it’s a complication of long term exposure to personal and/or work-related stress [1,7,8].
Most commonly the concept of occupational burnout itself reflects the six mismatches between people and their job, which include work overload, lack of control, insufficient reward, break down in the community, absence of fairness and conflicting values [1,9].
Occupational Burnout significantly affects the health professionals, accountants, lawyers, and teachers and other social workers [2,6,8], and is associated with adverse events that are directly related to the reduction in quality of care including medical errors, unexplained work absenteeism, job dissatisfaction, intention to exit the profession, low quality of personal and family life like physical exhaustion, insomnia, increased use of alcohol and drugs,marital and family problems [3,11].
Burnout is most common in health care professionals including midwifery as a result of physical, psychological and social aspects of the working environment [6,10,12]. The result of burnout affect’s their attitudes towards work, interpersonal skills and job performance and thus they can negatively influence the quality of care for clients [11,12]. The health and well-being of midwives are important to control sources of stress in the work place which appears to be important for the support of healthcare staffs, preservation of their performance and increase quality of healthcare [12,13].
The majority of studies on burnout in the international literature have employed the Maslach burnout inventory MBI [14,15]. This is designed to assess the three aspects of burnout; there are 22 items which are divided into three subscales and mostly measuring burnout in human service workers especially professions in which contact with clients or patients.
Conceptual Framework
This conceptual framework represents the relationship between variable and clearly (Figure 1)
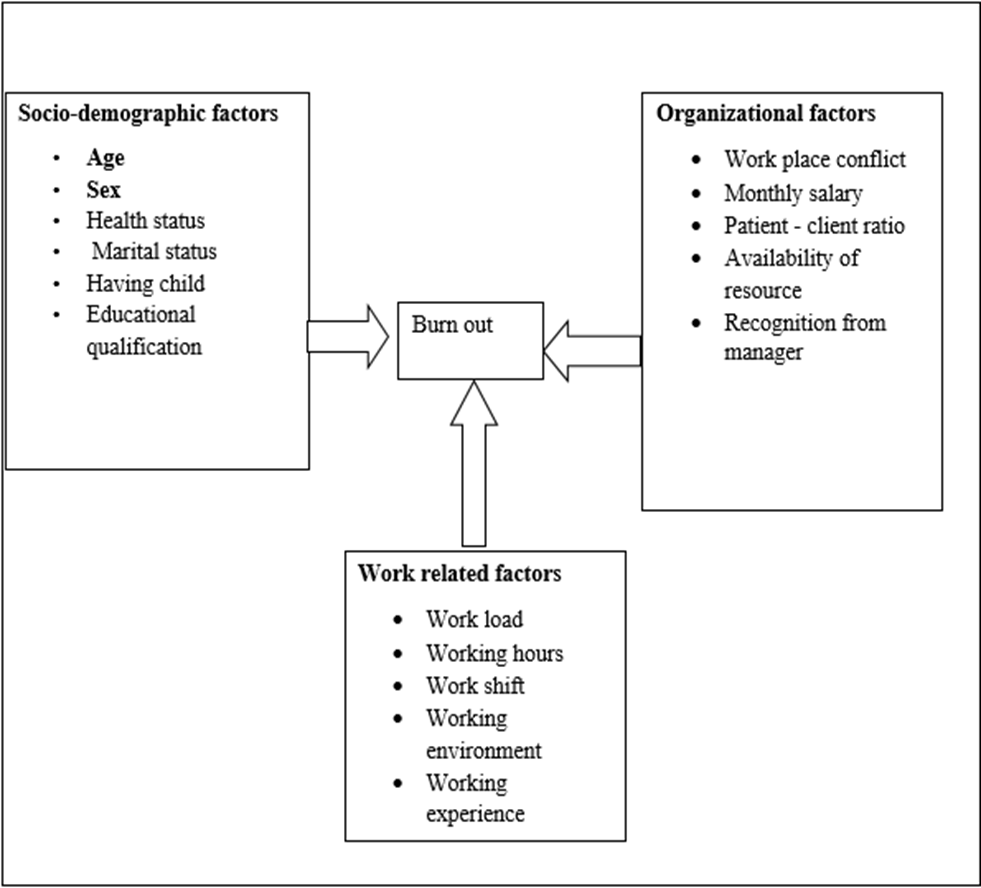
Figure 1. A figure showing conceptual framework of the prevalence and associated factors of burnout among midwives in governmental hospitals, Easter Amhara, Ethiopia, 2022.
MATERIALS AND METHODS
Study Area
This study was conducted in East Amhara region which is located in the North-eastern part of Ethiopia. It is bounded by Tigray region in the North and Northeast, Afar region in the east, Oromia region in the South and Southwest and also by West-east Gojjam and South Gonder zones. Eastern Amhara region is divided into 6 zones: North Showa, South Wollo, North Wollo, Wagehimra, Oromia special zone and Awei zones and had sixty-seven districts. The total surface area is 57,684mkm2. According to the 2007 E.C., the National Population and Housing Census of Ethiopia, the total population of Eastern Amhara was estimated 7,379,652, among this, 3,688,548 were females, and the rest 3,691,104 were males. In Eastern Amhara, there are 34 hospitals, of which two are referral hospitals (Desse referral and Debre Berhan referral hospitals) (Figure 2).
Study Design and Period
Facility based cross–sectional study was conducted on selected governmental hospitals of Eastern part of Amhara region of Ethiopia, from March 01-May 01 2021.
Source Population: All midwives who are working in governmental hospitals of East Amhara region
Study Population: Selected midwives who are working in selected governmental hospitals in East Amhara region.
Study Unit
The study unit was selected midwives.
Inclusion and Exclusion Criteria
Inclusion Criteria
All midwives work in maternal and child health rooms who have greater than or equal to one year experience.
Exclusion Criteria
Midwives who are on annual leaves, sick leaves and maternity leave during the data collection period.
Sample Size Determination
The sample size required for the study was calculated using the formula to estimate a single population proportion by considering the following assumptions:
Assumptions: With the assumptions of 95% Confidence interval,
Where
n= required sample size,
 = critical value for normal distribution at 95%confidence interval which equals to1.96 (Z value at alpha=0.05),
= critical value for normal distribution at 95%confidence interval which equals to1.96 (Z value at alpha=0.05),
P= Established prevalence of burn out among midwives.
d= desired precision (5% margin of error).
Since I can’t find researches on similar title in Ethiopia, I prefer to use 50%.
Since the total population is 420 midwifes, which is less than 10,000, it is advisable to use population correction formula
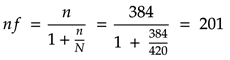
Considering 10% for non-response rate, the final sample size were 221 Midwives.
Sampling Technique
From 34 public hospitals that are found in east Amhara, 29 hospitals were selected by using the simple random sampling technique which was considered to be participated in the study, and then study subjects were proportionally allocated for each hospital. A total (221) study subjects were selected by simple random sampling technique from 420 midwives that are distributed in (29) governmental hospitals of East Amhara region of Ethiopia.
Study Variables
Dependent Variable
Midwives Burnout
Independent Variable
Socio-demographic variables:- Sex, Age, Health status, marital status, having child, Educational qualification; Work-related variables:- Workload, working hour, working shift, working environment, intention to leave in their work and work experience. Organizational variables:- workplace conflict, monthly salary, patient-client ratio, availability of resources, and receive recognition from managers.
Operational Definition
Burnout: It is a psychological syndrome characterized by emotional exhaustion (EE), depersonalization (DP) or cynicism and low personal achievements (PA)
Emotional Exhaustion (EE): emotional resources are depleted; workers feel they are no longer able to give of themselves at a psychological level.
Depersonalization (DP): negative, cynical attitudes and feelings about one's clients
Reduced Personal Accomplishment (PA): the tendency to evaluate oneself negatively particularly with regard to ones work with clients. (Referred to as a negative evaluation of one‘s work).
Measurement of variable in the study
Burnout was the outcome variable. It used the Maslach Burnout Inventory-Human Service Survey (MBIHSS) questionnaire to assess burnout. It is derived from the Maslach Burnout Inventory (MBI), it contains 22 questions which ask participants to indicate the frequency of various feelings experience. Each question has a six-point response scale (0: “never”, 1: “a few times a year or less”, 2: “once a month or less”, 3: “a few times a month”, 4: “once a week”, 5: “a few times a week”, and 6: “every day”), and is designed to measure the three domains of burnout; i.e., EE, DP, and PA. Scores in each of the three subscales were categorized into high, average, or low scores according to cut-offs detailed in the MBI manual
Emotional exhaustion: low (<16), moderate (17-26), high (≥27).
Depersonalization: low (<6), moderate (7-12), high (≥13).
Personal accomplishment: low (≤31) moderate (32-38), high (≥39).
High EE is indicated by a score ≥ 27, high DP is indicated by a score ≥ 13, and low PA is indicated by a score ≤ 31.
Participants were identified as having a burnout if they scored high in EE and DP, and low in PA. The MBI-HSS is a reliable and valid instrument to assess burnout [16-41,42,43].
Data Collection Method
To assess prevalence of burnout and its associated factors among midwives Amharic version of Maslacs Burnout Inventory- Human Services Survey (MBI-HSS) was use, which comprises 22 items with 9 items for emotional exhaustion (EE), 5 items for depersonalization (DP), and 8 items personal accomplishment (PA).
Each item was answered on a 7-point which ranging from never (= 0) to daily (= 6). The data was collected by using self-administered questionnaire MBI-HSS was reliable and valid. The first questioner was prepared in English language including MBI questionnaire then translated to the Amharic version for ease of understanding by the data collector and the respondents.
To obtain socio-demographic data relevant to the study participants was also be asked to provide information with regard to their age, sex, marital status, health status, educational level, work unit, service years of experience, working shift, work load, and finally intention to leave work within the next 12 months.
The data collectors were BSc nurse students who were taken from the nearest study area. The number of data collectors is varying based on the number of hospitals found in each zone. A total of 16 data collector was included. For North showa zone with 11 governmental hospital, 5 data collectors were assigned, for South wollo zone with 12 governmental hospitals, a total of 6 data collectors were trained and assigned, for North Wollo which has 6 governmental hospitals, I allocate 3 data collectors and Oromia special zone and Wagehemera zones with one governmental hospital each, I assigned 1 data collector for each. And 8 supervisors were actively involved in the supervision of the data collection. Each data collected and supervisors were appropriately trained for one day.
Data Quality Assurance
In order to assure the quality of data the following measures were taken. Quality and reliability were assessed using pre-test conduct in hospital which was not included in the study on 5% of the sample size before 2 weeks of the actual data collection period. The training was given to data collectors and supervisors. The data collectors were BSc nurse students who were taken from the nearest study area. The principal investigator and supervisors were actively involved in supervision of the data collection. Data collectors were supervised at each site. The complete questionnaire was checked for miss values and completeness on daily basis. Data cleaning were done using EPi version 3.7 by removing the instruments with missed values. Two times Revisiting was done if respondents were not found in the first visit.
Data processing, analysis and presentation
Data entry was performed by using Epi version software and for data analysis transferred to SPSS version 23 statistical software. Different frequency tables, graphs and descriptive summaries were used to describe the study variables Model goodness of fit test were checked by Hosmer-Lemeshaw test and insignificant result (larger P-value) were considered as a good fit. Multicollinearity between independent variables was assessed. Binary logistic regression model was used to measure the association between burn out and risk factors. A variable that has P-value ≤ 0.25 on bi-variable regression analysis and had association with burnout in previous studies was fitted into the multivariate logistic regression model to assess their association with the outcome variable. Adjusted Odds ratio (AOR) with 95 % confidence interval (CI) was calculated and P value ≤ 0.05 were declared statistically significant.
RESULT AND DISCUSSION
RESULT
Midwives’ socio-demographic characters
A total of 221 midwives participated in this study, with 97.7% a response rate. The analysis of socio-demographic profile of midwives’ population showed that there were 102(47.2%) male and 114(59.3 %) of them were married and 45.8% midwives were found between the age of 31-40. With regard to the educational level majority 135(62.5%) were BSc and above around 154(71.3%) midwives had good health (Table 1).
Table 1. Socio-demographic characteristics of midwives worked in East Amhara hospitals Ethiopia, 2021.n=216.
|
Variables |
Category |
Frequency |
Percentage |
|
Sex |
Male Female |
102 114 |
47.2 52.8 |
|
Age |
20-30 31-40 >40 |
90 99 27 |
41.7 45.8 12.5 |
|
Marital status |
Single Married
|
88 128
|
40.7 59.3
|
|
Having child |
Have child Have no child |
140 76 |
64.8 35.2 |
|
Current health status |
Health Poor health |
154 62 |
71.3 28.7 |
|
Current educational level |
Diploma Degree and above |
81 135 |
37.5 62.5 |
Work-related factors 99 (45.8%) midwives were 5-8 years’ experience. Regarding current duty shift around 103(47.7%), midwives were working in day shift. 102(47.2%) midwives work in the stressful unit and 126(58.3%) have the intention to leave their current work within the next 12 months (Table 2).
Table 2. Work-related character of midwives worked in East Amhara hospitals Ethiopia 2021. n=216.
|
Variables |
Category |
Frequency |
Percentage |
|
Service year |
1-4 5-8 >8 |
84 99 33 |
38.9 45.8 15.3 |
|
Current duty shift |
Day Night Alternative |
103 49 64 |
47.7 22.7 29.6 |
|
Workload |
Yes No |
135 81 |
62.5 37.5 |
|
Working hour |
Up to 40 41-60 >60 |
44 57 115 |
20.4 26.4 53.2 |
|
Work in a stressful unit |
Yes No |
102 114 |
47.2 52.8 |
|
Plan to leave work within 12 month |
Yes No |
126 90 |
58.3 41.7 |
In organizational factors 99(45.8%) midwives were reports the shortage of staff member and 87(40.3%) describe the hospital has enough resources.75 (34.7%) midwives are in conflict with hospital manager and 67 (31%) midwives consider the manager give recognition to the workers (Table 3).
Table 3. Organizational-related characters of midwives worked in East Amhara hospitals Ethiopia 2021.n=216.
|
Variables |
category |
Frequency |
Percentage |
|
Shortage of staff member |
Yes No |
99 117 |
45.8 54.2 |
|
Availability resource |
Yes No |
87 129 |
40.3 59.7 |
|
Conflict with manager |
Yes No |
75 141 |
34.7 65.3 |
|
Conflict with co-workers |
Yes No |
53 163 |
24.5 75.5 |
|
Salary is enough to current work |
Yes No |
62 154 |
28.7 71.3 |
|
Manager give recognition |
Yes No |
67 149 |
31 69 |
Of the 216 participants, 112(51.9%), 95% CI: (45.4-58.8) midwives have experienced burnout. Among those respondents 113 (52.3%), 111 (51.4%), and 127 (58.8%) midwives had scored the high level of Emotional Exhaustion (EE), high Depersonalization (DP) and low personal achievement (PA) sub-scales respectively (Table 4).
Table 4. Description of burnout sub-scales of MBI-HSS midwives work in East Amhara hospital, Ethiopia, 2021. n= 216.
|
Sub-scales |
High |
Moderate |
Low |
|||
|
Frequency |
% |
frequency |
% |
Frequency |
% |
|
|
Emotional Exhaustion |
113 |
52.3 |
14 |
6.5 |
89 |
41.2 |
|
Depersonalization |
111 |
51.4 |
10 |
4.6 |
95 |
44.0 |
|
Personal Achievement |
44 |
20.4 |
45 |
(0.8 |
127 |
58.8 |
.png)
Figure 2. Map of Amhara Region, Amhara, Ethiopia, 2022.
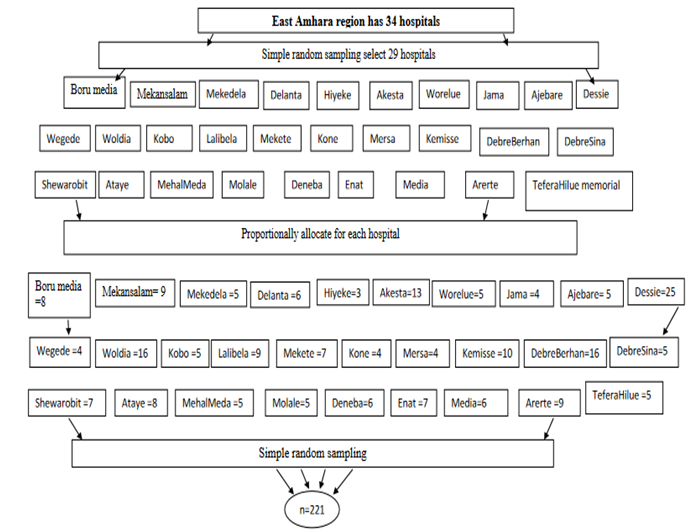
Figure 3: Sampling procedure of midwives on Burnout and its associated factors.
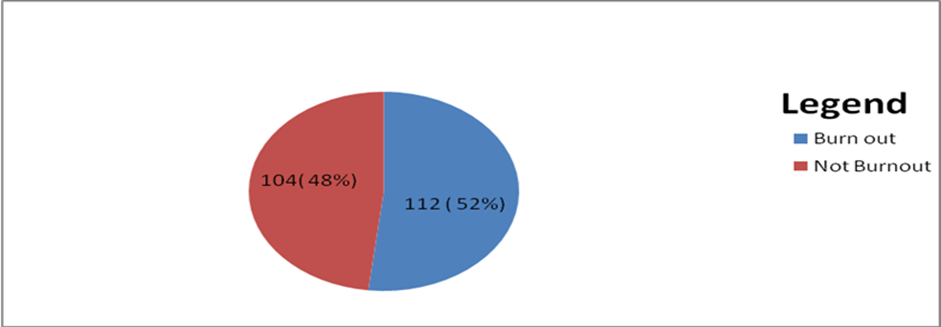
Figure 4. Prevalence of midwives burnout in public hospitals of East Amhara region, Ethiopia, 2021.
Associations of midwives Burnout
Bivariate logistic regression analysis of midwives’ burnout
The bivariate logistic regression analysis results of the burnout among the study participant of midwives work in east Amhara public hospital revealed that variables such. Midwives age, marital status, midwives have child, current health status, duty shift, workload, working hour, intention to leave work within 12 months, client patent ratio, availability of resources, conflict with manager, salary enough to the current work and recognition from manger had an association with midwives’ professional burn out in bivariate logistic regression analysis.
Multivariate logistic regression analysis of midwives’ burnout
All variables that have an association with the outcome variables in bivariate logistic regression analyses were included in the multiple logistic regression models. After controlling for the effects of potentially confounding variables using multiple logistic regression; midwives’ intention to leave their work, shortage of staff member, having child and conflict with the hospital manager were significantly associated with midwife’s professional burnout.
Midwives who had the intention to leave their work were 2.3 times [AOR=2.320; 95% CI: (1.307, 4.119)] more likely develop professional burnout than those midwives who do not plan to leave their work in the next 12 months. Regarding the staff members of the midwives work in the shortage of staff member were 2 times [AOR= 2.00; 95% CI: (1.141, 3.505) more likely develop burn out than those midwives works with enough staff members. Midwives conflict with hospital manager were 2.1 times [AOR=2.133; 95% CI: (1.189, 3.825)] more likely experience burnout than those midwives work without conflict to the hospital manager. Additionally, midwives have one or more child 3.3 times [AOR=3.348; 95% CI: (1.617, 6.930)] more likely to develop professional burnout than those midwives how had no child (Table 5).
Table 5. Multivariate and bivariate logistic regression analysis burnout among midwives work in East Amhara hospitals, Ethiopia, 2021.
|
Variables |
Burn out |
COR(95%CI) |
p-value |
AOR (95%CI) |
p-value |
|
|
Yes |
no |
|
|
|
|
|
|
Age |
|
|
|
|
|
. |
|
20-30 |
54 |
36 |
0.458 (.191-1.100) |
0.081 |
0.693(.267-1.797) |
0.451 |
|
31-40 |
47 |
52 |
0.761 (.321-1.803) |
0.534 |
0.963(.381-2.431) |
0.937 |
|
>40 |
11 |
16 |
1 |
|
|
|
|
Marital status |
|
|
|
|
|
|
|
Single |
57 |
31 |
0.410 (.234-.717) |
0.002 |
0.680(.362-1.278) |
0.231 |
|
Marred |
55 |
73 |
1 |
|
|
|
|
Number of child |
|
|
|
|
|
|
|
Have 1 or more child |
89 |
51 |
4.021(2.221-7.315) |
0.000 |
3.348 (1.617, 6.930) |
0.001* |
|
Have no child |
23 |
53 |
1 |
|
|
|
|
Current health status |
|
|
|
|
|
|
|
Good health |
87 |
67 |
0.520(.286-947) |
0.033 |
1.091(.527-2.260) |
0.814 |
|
Poor health |
25 |
37 |
1 |
0.130 |
|
|
|
Duty shift |
|
|
|
|
|
|
|
Alternative |
26 |
38 |
1.741(.926-3.76) |
0.085 |
1.297(.305-1.301 |
0.481 |
|
Night |
30 |
19 |
0.755 (.377-1.509) |
0.426 |
0.629(.315-1.137) |
0.211 |
|
Day |
56 |
47 |
1 |
0.376 |
|
|
|
Work load |
|
|
|
|
|
|
|
Yes |
78 |
57 |
0.529(.303-.924) |
0.025 |
0.599(.315-1.137) |
0.117 |
|
No |
34 |
47 |
1 |
|
|
|
|
Work hour |
|
|
|
|
|
|
|
1-40 hr |
19 |
25 |
1.837(.910-3.707) |
0.090 |
1.164(.502-2.699) |
0.724 |
|
41-60hr |
26 |
31 |
1.664(.878-3.155) |
0.119 |
1.419(.716-2.812) |
0.316 |
|
>60 |
67 |
48 |
1 |
|
|
|
|
Plan to leave work |
|
|
|
|
|
|
|
Yes |
55 |
71 |
2.230(1.280-3.883) |
0.005 |
2.320(1.307-4.119) |
0.004* |
|
No |
57 |
33 |
1 |
0.012 |
|
|
|
Shortage of staff |
|
|
|
|
|
|
|
Yes |
42 |
57 |
2.021(1.174-3.481) |
0.011 |
2.00(1.141-3.505) |
0.015* |
|
No |
70 |
47 |
1 |
0.035 |
|
|
|
Availability of resource |
|
|
|
|
|
|
|
Yes |
40 |
47 |
1.484(.859-2.563) |
0.157 |
1.588(.898-2.808) |
0.111 |
|
No |
72 |
57 |
1 |
0.188 |
|
|
|
Conflict with manager |
|
|
|
|
|
|
|
Yes |
30 |
45 |
2.085(1.178-3.688) |
0.012 |
2.133(1.189-3.825) |
0.011* |
|
No |
82 |
59 |
1 |
0.054 |
|
|
|
Salary is enough |
|
|
|
|
|
|
|
Yes |
25 |
37 |
1.922(1.056-3.499) |
0.033 |
1.836 (.983-3.432) |
0.057 |
|
No |
87 |
67 |
1 |
0.108 |
|
|
|
Manager recognition |
|
|
|
|
|
|
|
Yes |
30 |
37 |
1.509(.845-2.695) |
0.164 |
1.425(.775-2.617) |
0.254 |
|
No |
82 |
67 |
1 |
0.220 |
|
|
In order to successfully tackle burnout problems in Ethiopia particularly in the present study area, there appears a need to investigate the level of burnout and associated factors among midwives. Accordingly, this study had tried to look into the level of burnout and associated factors in the study area. The finding of this study showed that 51.9 % of midwives who were working in East Amhara hospitals experienced burnout on the MBI, with 52.3% reporting high on emotional exhaustion, 51.4 % high on depersonalization, and 58.8 % low on personal accomplishment. The result is relatively in line with studies done in Mekelle, systemic review in sub-Sahara Africa and Senegal 47.6% 55%, 55% respectively [4,11,28]. The consistency may possibly be due to African countries are developing and almost similar economic development, similar nature of work environment like patient demand, payment system, work load and health policy.
Other Similarly studies in Norway and west Canada which indicated that midwife professionals are highly susceptible and affected by burnout with prevalence 50% and 47.7% respectively [7,22]. The alignment between the results adds strength to the argument that the issues fuelling burnout are potentially consistent across maternity work environments.
In this study an intention to leave their work in the next 12 months showed positive association with burnout than those midwives who do not plan to leave their work in the next 12 months .The result of this finding was consistent with the findings in west Canada and Swedish [22,30]. This may be due to workplace characteristics linked to intention to leave work with high demand (e.g. time constraints on time to task completion, work distribution, time to talk with patients) and low control (e.g. lack of autonomous task prioritization and completion) in addition to this Inadequate staffing and unsupportive management are reasons for midwives to leave their profession and could be the reason for midwives experiencing high levels of stress [44].
This study also revealed that the midwives having 1 or more children strongly associated with burnout as compared to the midwives have no child. This finding is consistent with the findings of previous studies done in West Canada, burn out in an international setting New York, Rwanda and Malawi [22,29,37,38]. This may probably due to domestic duties, such as child rearing and being accountable to one’s spouse, may introduce additional and sometimes intensive responsibilities. The preoccupation with providing and caring for one’s child and or completing domestic duties, with possibly low spousal support, may create distractions that thwart job performance. This illustrates family-to-work conflicts where the demands from the family/home and work domains are mutually incompatible such that fulfilling the parental role makes it difficult to perform the work role satisfactorily [45].
This study revealed that the shortage of staff member to client ratio associated to professional burn out than those midwives works without shortage in the staff members. This finding is consistent with a Systematic Review and Meta-Analysis in an international setting, Systematic review in sub-Saharan Africa and Swedish [11,20,30].This may be due to under-staffing and attrition can reduce job satisfaction. Opportunities for collegial interaction and support, identified as contributing to job satisfaction are restricted [46]. Teamwork is an essential component of high quality maternal health care, and loss of team members can also reduce job satisfaction and lower morale [47]. With increasing workload and changing role expectations, levels of stress, fatigue and emotional exhaustion can increase, all of which compromise both quality and safety of care [48]. A continued inability to provide quality care can contribute to job dissatisfaction, stress, de-motivation and intentions to seek other employment, creating a vicious cycle of staff attrition.
This finding revealed that conflict or disagreement with hospital manager associated to burnout than those midwives who work with an agreement or without conflict of the hospital manager. This finding is consistent with the Systematic review of burnout in sub-Saharan, in weast canada and Swedish midwives [11,22,30]. may be probably increased tension decrease motivation to work this leads to work disruptions, decreased productivity, absenteeism, turnover, stress and termination.
CONCLUSION
This study presents a significant proportion of midwives were suffer from professional burnout due to their jobs. From the total of the participants, more than half of midwives were suffered from professional burnout. Statistically significant associations were identified between burnout and its associate factors: like, midwives’ intention to leave their work in the next 12 months, shortage of staff member, having child and conflict with the hospital manager.
DATA AVAILABILITY
The data used to support the findings of this study are included in the manuscript.
CONFLICTS OF INTEREST
The author has no conflicts of interest to declare. All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report. We certify that the submission is original work and is not under review at any other publication.
FUNDING
Fieldwork of this research was self-sponsored.
ACKNOWLEDGMENTS
First and foremost, we praise the almighty God who has never left me alone at every step of my life, for giving me the endurance during the write-up of this research thesis. Our gratitude extends to hospital managers in east Amhara who supported us from the beginning of the data collection until the end. It is also our pleasure to thank study participants, midwives working in hospital in eastern Amhara, and data collectors, without their honest participation this work would have been nothing.
ETHICAL APPROVAL AND CONSENT TO PARTICIPATE
The permission was obtained from Debre Berhan University School of health science department of public health and selected hospital administration to conduct the study. All concerned officials at all levels of selected hospitals were communicated and informed about the purpose of the study. Confidentiality of the response was assured by informing the data collector not to record the name of the participant on the questioners. Written consent and sign by the participant were obtained for each study subject before the data collection. Participation in the study was on a voluntary basis.
REFERENCES
- Maslach C, Schaufeli WB, Leiter MP. (2001). Job Burnout. Annu Rev Psychol. 52(1):397-422.
- Schaufeli WB, Buunk BP. (2003). Burnout: An overview of 25 years of research and theorizing. The handbook of work and health psychology. 2(1):282-424.
- Maslach C JSE, Leiter MP. (1996). The maslach burn out invontery manual palo Alto, CA consulting psycologists press. pp. 191-218.
- Redae GH, Dai YC. (2019). Prevalence and associated factors of burnout syndrome among healthcare workers in public and private hospitals in Mekelle City, Ethiopia. SSMJ. 12(1):5-8.
- Freudenberger HJ. (1974). Staff burn‐out. Journal of social issues. 30(1):159-165.
- Freudenberger HJ. (1975). The staff burn-out syndrome in alternative institutions. Psychotherapy: Theory, Research & Practice. 12(1):73-82.
- Henriksen L, Lukasse M. (2016). Burnout among Norwegian midwives and the contribution of personal and work-related factors: a cross-sectional study. Sexual & Reproductive Healthcare. 9:42-47.
- Leiter MP, Maslach C. (2005). Banishing burnout: Six strategies for improving your relationship with work. New Jersey, United States: John Wiley & Sons.
- Maslach C, Leiter MP. (2008). The truth about burnout: How organizations cause personal stress and what to do about it. New Jersey, United States: John Wiley & Sons.
- Lemu HA. (2015). Prevalence of nurses burnout and its determinant factors in public Hospitals, Addis Ababa. Ethiopia: Addis Ababa University.
- Dubale BW, Friedman LE, Chemali Z, Denninger JW, Mehta DH, Alem A, et al. (2019). Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC public health. 19(1):1247.
- Banovcinova L, Baskova M. (2014). Sources of work-related stress and their effect on burnout in midwifery. Procedia-Social and Behavioral Sciences. 132:248-254.
- Creedy D, Sidebotham M, Gamble J, Pallant J, Fenwick J. (2017). Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC pregnancy and childbirth. 17(1):1-8.
- Kristensen TS, Borritz M, Villadsen E, Christensen KB. (2005). The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work & Stress. 19(3):192-207.
- Woodside JR, Miller MN, Floyd MR, McGowen KR, Pfortmiller DT. (2008). Observations on burnout in family medicine and psychiatry residents. Acad Psychiatry. 32(1):13-19.
- Wright EM, Matthai MT, Budhathoki C. (2018). Midwifery professional stress and its sources: a mixed‐methods study. J Midwifery Womens Health. 63(6):660-667.
- Lamont S, Brunero S, Perry L. (2017). 'Mental health day' sickness absence amongst nurses and midwives: workplace, workforce, psychosocial and health characteristics. J Adv Nurs. 73(5):1172-1181.
- Harvie K, Sidebotham M, Fenwick J. (2019). Australian midwives' intentions to leave the profession and the reasons why. Women birth. 32(6):e584-e593.
- Hunter L, Magill-Cuerden J, McCourt C. (2015). ‘Oh no, no, no, we haven׳ t got time to be doing that’: Challenges encountered introducing a breast-feeding support intervention on a postnatal ward. Midwifery. 31(8):798-804.
- Suleiman-Martos N, Albendín-García L, Gómez-Urquiza JL, Vargas-Román K, Ramirez-Baena L, Ortega-Campos E, et al. (2020). Prevalence and predictors of burnout in midwives: a systematic review and meta-analysis. Int J Environ Res Public Health. 17(2):641.
- Shirom A. (2005). Reflections on the study of burnout. Work & Stress. 19(3):263-270.
- Stoll K, Gallagher J. (2019). A Survey of burnout and intentions to leave the profession among Western Canadian midwives. women and birth. 32(4): e441-e449.
- Winter GF. (2019). Dealing with burnout: British Journal of Midwifery.
- McCrossan R, Stacey K, Redfern N. (2019). Time to extinguish burnout. Anaesthesia. 74(10):1215-1218.
- Katsantoni K, Zartaloudi A, Papageorgiou D, Drakopoulou M, Misouridou E. (2019). Prevalence of Compassion Fatigue, Burn-Out and Compassion Satisfaction Among Maternity and Gynecology Care Providers in Greece. Mater Sociomed. 31(3):172-176.
- Uchmanowicz I, Manulik S, Lomper K, Rozensztrauch A, Zborowska A, Kolasińska J, et al. (2019). Life satisfaction, job satisfaction, life orientation and occupational burnout among nurses and midwives in medical institutions in Poland: a cross-sectional study. BMJ Open. 9(1):e024296.
- Zarei E, Ahmadi F, Sial MS, Hwang J, Thu PA, Usman SM. (2019). Prevalence of Burnout among Primary Health Care Staff and Its Predictors: A Study in Iran. Int J Environ Res Public Health. 16(12):2249.
- Rouleau D, Fournier P, Philibert A, Mbengue B, Dumont A. (2012). The effects of midwives’ job satisfaction on burnout, intention to quit and turnover: a longitudinal study in Senegal. Hum Resour Health. 10(1):9.
- Paul SSJ. (2012). Predictors of burnout amongst nurses in paediatric and maternity wards of district hospitals of Kigali City, Rwanda.
- Hildingsson IWK, Wiklund I. (2013). Sexual & Reproductive Healthcare Burnout in Swedish midwives. Sex Report Health. 4:87-91.
- Lrago T, Asefa F, Yitbarek K. (2018). Physicians' Burnout and Factors in Southern Ethiopia Affecting It. Ethiop J Health Sci. 28(5):589-98.
- Adbaru DG AZ, Demelew TM, Teshome GS. (2019). Magnitude of burnout and its associated factors among nurses working in public hospitals of Amhara regional state, Ethiopia. 8(2):133-141.
- Zewdu AT AH, Abebe N, Dessie G. Level of burnout and associated factors among nurses working in public health institutions north shoa zone, Amhara. Int J Soc Relev Concern. 2017;5(8):17-26.
- Bhagavathula AS, Abegaz TM, Belachew SA, Gebreyohannes EA, Gebresillassie BM, Chattu VK. (2018). Prevalence of burnout syndrome among health-care professionals working at Gondar University Hospital, Ethiopia. J Educ Health Promot. 7:145.
- Hailay A, Aberhe W, Mebrahtom G, Zereabruk K, Gebreayezgi G, Haile T. (2020). Burnout among nurses working in Ethiopia. Behav Neurol. 2020:8814557.
- Yavuzşen HT, Vupa Çilengiroğlu Ö. (2015). Burnout in physicians and nurses working in Obstetrics/Gynecology clinics in Turkey. Turkiye Klinikleri J Gynecol Obst. 25(1):160-167.
- Thorsen VC, Tharp ALT, Meguid T. (2011). High rates of burnout among maternal health staff at a referral hospital in Malawi: A cross-sectional study. BMC Nurs. 10(1):9.
- Carod-Artal FJ, Vázquez-Cabrera C. (2013). Burnout syndrome in an international setting. Burnout for experts: Springer. p. 15-35.
- Oe M, Ishida T, Favrod C, Martin-Soelch C, Horsch A. (2018). Burnout, psychological symptoms, and secondary traumatic stress among midwives working on perinatal wards: A cross-cultural study between Japan and Switzerland. Front Psychiatry. 9:387.
- Muliira RS, Ssendikadiwa VB. (2016). Professional quality of life and associated factors among Ugandan midwives working in Mubende and Mityana rural districts. Matern Child Health J. 20(3):567-576.
- Metlaine A, Sauvet F, Gomez-Merino D, Boucher T, Elbaz M, Delafosse JY, et al. (2018). Sleep and biological parameters in professional burnout: A psychophysiological characterization. PLoS One. 13(1):e0190607.
- Maslach C, Jackson SE. (1981). The measurement of experienced burnout. Journal of organizational behavior. 2(2):99-113.
- Maslach C, Jackson S, Leiter M. (1996). MBI: Maslach burnout inventory: CPP. USA: Incorporated Sunnyvale (CA).
- Curtis P, Ball L, Kirkham M. (2006). Ceasing to practise midwifery: working life and employment choices. British journal of midwifery. 14(6):336-338.
- Hasselhorn HM, Conway PM, Widerszal-Bazyl M, Simon M, Tackenberg P, Schmidt S, et al. (2008). Contribution of job strain to nurses' consideration of leaving the profession--Results from the longitudinal European nurses' early exit study. Scandinavian journal of work, environment & health. 34(6):75-82.
- Hall E. (2004). Nursing attrition and the work environment in South African health facilities. Curationis. 27(4):28-36.
- Xaba J, Phillips G. (2001). Understanding nurse emigration: final report. Pretoria: Trade Union Research Project.
- Al-Hassan M. (2004). The causes and effects of international migration of health professionals: the case of nurses at the Korle-Bu Teaching Hospital in Ghana: Dissertation, Leeds: University of Leeds.