Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Nephrectomy in an Infant during Intraoperative Cardiac Arrest, Requiring Prolonged Resuscitation. Case Report
Luiz Eduardo Imbelloni1,*, Anna Lúcia Calaça Rivoli2, Sylvio Valença de Lemos Neto3, Ana Cristina Pinho3, Livia dos Santos Pereira4
1Senior Nacional Cancer Institute (INCA) Researcher, Rio de Janeiro, RJ, Brazil
2Anesthesiologist at the National Cancer Institute (INCA), Responsible Coreme Residence INCA, Brazil
3Anesthesiologist at the National Cancer Institute (INCA), Responsible for the CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
4Resident in the 3rd year of Anesthesiology at INCA, Rio de Janeiro, RJ, Brazil
*Corresponding Author: Dr. Luiz Eduardo Imbelloni, Av. Epitácio Pessoa, 2356/203 – Lagoa, 22411-072- Rio de Janeiro, RJ – Brazil; Tel: + 55.11.99429-3637; Email: [email protected]
Received Date: August 21, 2023
Publication Date: September 04, 2023
Citation: Imbelloni LE, et al. (2023). Nephrectomy in an Infant during Intraoperative Cardiac Arrest, Requiring Prolonged Resuscitation. Case Report. Mathews J Cancer Sci. 8(3):42.
Copyright: Imbelloni LE, et al. © (2023)
ABSTRACT
Wilms' tumor is one of the main tumors in children, is characterized as a malignant renal neoplasm resulting in the abnormal reproduction of metanephric blastema cells. The incidence of the disease is higher between two and five years of age and rare after ten years. We present a case report involving a 7-month-old child with an extensive mass in the topography of the left kidney to the pelvis, with an expansive retroperitoneal lesion occupying the left hemiabdomen and displacing the aorta and inferior vena cava. Tumor resection was indicated, and after induction and intubation, the child had cardiac arrest. Resuscitation maneuvers were performed until the tumor was removed, 40 minutes later. ETCO2 remained within normal limits during this period, and the cardiac rhythm spontaneously returned to normal as soon as the mass was removed. The child remained hospitalized for 39 days, being discharged to your residence, and seven months after the surgery she did not have any neurological sequelae and was developing normally for her age.
Keywords: Wilms Tumor; Surgery; Cardiac Arrest; Cardiopulmonary Resuscitation; Children
KEY POINTS
What is already known?
- Embryonic tumors mostly affect the young children.
- Wilms' tumor is the most common renal’s tumor in children.
- The number of new cases of childhood cancer estimated for Brazil, for the next three-year period from 2023 to 2025, is 7,930 cases.
- In Brazil the incidence of cardiac arrest in children 22.9 per 10,000.
- In meta-analyses the global incidence of perioperative CA was 2.54 per 1,000 anesthetics in children.
- CPR for > 20 minutes has been considered futile after pediatric in-hospital CA.
- ETCO2 measurements during resuscitation are indirect measures of pulmonary blood flow, and cardiac output.
What this case report adds.
- CT scan showed extensive renal mass with retroabdominal involvement in a 7-month-old child with Wilms tumor.
- CT scan showed compression of the aorta and inferior vena cava, a frequent event in huge abdominal masses, which can increase the risk of cardiovascular collapse after induction of anesthesia.
- Anesthetic agents with sympatholytic effects may have contributed to CA after induction and intubation.
- CPR for 40 minutes with normal ETCO2 values and normal oximetry value allowed tumor removal and the return of spontaneous cardiac activity.
- The presence of normal capnography should always encourage continued resuscitation efforts.
- The neurological outcome and normal global development of the child demonstrates that CPR, despite 40 min long, was effective.
- Seven months after the surgery, the child has no sequelae and is developing normally.
- This case demonstrated that CRP was sufficient for 40 minutes for the child to recover completely
- The highlight in this case is not the duration of CRP but the effectiveness evaluated mainly by ETCO2 and pulse plethsmography/oximetry.
INTRODUCTION
Renal tumors account for approximately 7% of all pediatric tumors, and Wilms' tumor is the most common in children [1]. Wilms tumor (also known as nephroblastoma) is a malignant tumor originating in the kidney. It is the most common type of kidney tumor in childhood and can affect one or both kidneys [1]. The number of new cases of childhood cancer estimated for Brazil, for the three-year period from 2023 to 2025, is 7,930 cases [1]. The embryonic tumors (neuroblastoma, renal tumors and retinoblastoma) mostly affect the younger children.
In 2006, a Brazilian study evaluating cardiac arrest (CA) in children for 9 years in 15,253 anesthetics in a tertiary hospital, showed an incidence of 22.9 per 10,000, with no deaths being atributable to anesthesia [2]. Major risk factors for cardiac arrest were neonates and children under 1 year old, ASA III or poorer physical status, emergency surgery, and general anesthesia in cardiac, thoracic, or gastroenterological surgery.
Recent meta-analyses revealed that the global incidence of perioperative CA was 2.54 per 1,000 anesthetics in children, and that the incidence of these anesthetic complications and mortality was very high among in low-middle income countries, whiche has remained persistent in the last two decades [3].
We present a 7-month-old child and weighing 7.5 kg, who experienced a sudden CA following anesthetic induction and intubation for total left nephrectomy in the presence of an extensive abdominal mass in the topography of the left kidney to the pelvis, with an expansive retroperitoneal lesion occupying the left hemiabdome and displacing the aorta and inferior vena cava.
CASE REPORT
A fast-track protocol was registered on the Brazil platform (CAAE: 09091312.1.0000.5179), to study perioperative procedures in patients of the Brazilian Health System (SUS). The Ethics Research Committee approved the study protocol (Number: 171.924). The preparation of this case report followed the guidelines of the Department of Anesthesia and Pediatric Oncological Surgery of the Cancer National Institute. Female infant patient, seven months old and weighing 7.5 kg, with indication for a left nephrectomy. At six months of life, a CT scan revealed an extensive retroperitoneal mass in the topography of the left kidney down to the pelvis, displacing the aorta and inferior vena cava to the right (Figure 1). Chest CT scan was normal. Laboratory tests indicated anemia with 8.7% hemoglobin, absence of leukocytosis, normal electrolytes; C-reactive protein 0.42 mg/l, and normal coagulogram. Transthoracic echocardiogram showed an ejection fraction of 63%. She was in use of captopril (4mg/kg/day) due to arterial hypertension, being then classified as ASA II.
The patient was held nil per os for 4 hours and evaluated preoperatively by the attending anesthesiologist. The patient was transported to the operating room, where routine hospital monitoring was placed (pulse oximeter, cardioscope, capnography and non-invasive blood pressure). Initial parameters were HR 118bpm, BP 105X65mmHg, and a saturation of 100%.
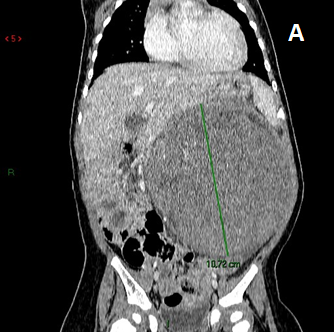
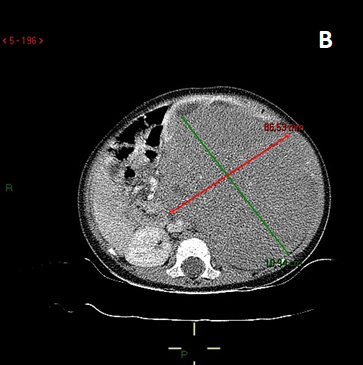
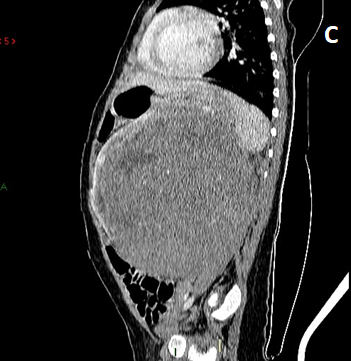
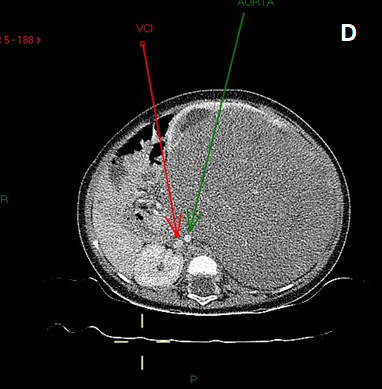
Figure 1: CT scan of the abdomen showed a large mass in the left renal topography up to the pelvis and retroperitoneal with compression of the aorta and inferior vena cava, in coronal, axial, and sagittal sections, measuring 86.53 cm and 70.94 cm.
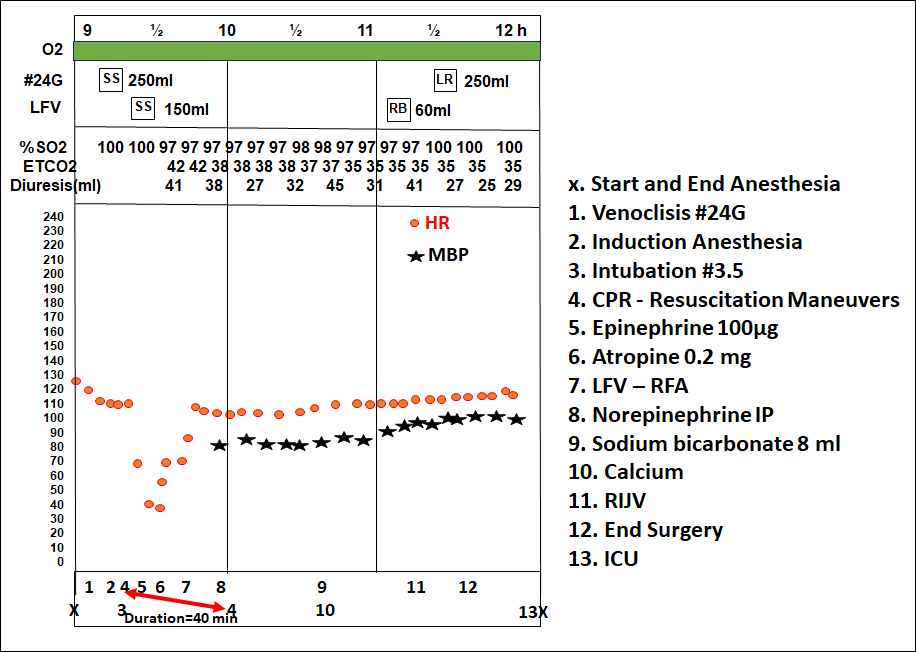
Figure 2: Anesthesia record throughout the procedure.

Figure 3: Seven days after cardiac arrest in the ICU.

Figura 4: Seven months after tumor removal.
Anesthesia was induced with the inhalation of incremental concentrations of sevoflurane in a mix of nitrous oxide and oxygen. After loss of consciousness, a 24G peripheral intravenous cannula was placed, and lidocaine 10mg, esmolol 5mg, propofol 20mg, rocuronium 10mg were administered. Intubation was performed with an uncuffed 3.5 orotracheal tube, under direct laryngoscopy and without intercurrences.
After confirmation of intubation by capnography, bilateral thoracic expansion and present pulmonary auscultation, the infant presented bradycardia followed by cardiopulmonary arrest (CPA) in asystole. Cardiopulmonary resuscitation maneuvers were initiated, with no return of cardiac activity. At this time, sevoflurane and nitrous oxide were discontinued and the patient was ventilated with 100% oxygen. Left femoral vein (LFV) and right femoral artery (RFA) were punctured. In discussion with the anesthetic and surgical team about the cause of the CA compression of the aorta-caval system was considred, and the decision towards the removal of the mass was made.
CPR was performed according the Advanced Cardiac Life Support (ACLS) protocols for 40 minutes, the time period for the excision of the tumor. Immediately afterwards,cardiac activity returned spontaneously, and external chest compressions were interrupted. During the procedure, a total of 650ml of crystalloid solution and 60ml of red blood cell concentrate were administered, as well as the replacement of sodium bicarbonate and calcium chloride. Total blood loss was 800ml, and diuresis 336ml (Figure 2). The right internal jugular vein was. At the end of the surgery the child was referred to the ICU intubated, monitored, and with a norepinephrine infusion (0.5µg/kg/min).
Histological analysis of the mass (kidney and tumor), which measured 12.0x8.0 cm, confirmed a Wilms tumor, with a stage III hilar lymph node and chronic pyelonephritis.
The infant remained intubated in the ICU for six days, under neuroprotective care. After extubation on the seventh postoperative day, the patient was kept monitored and fed through a nasoduodenal tube (Figure 3). Neuroimaging examination revealed ischemia in the frontal and occipital region, along with complications such as global cardiac dysfunction and seizures, controlled with medication. She was discharged home 39 days after surgery. She underwent adjuvant chemotherapy and radiotherapy, and is currently (seven months after surgery) with the disease under control. She has presented a satisfactory motor and cognitive development (Figure 4).
DISCUSSION
We have reported a case of unexpected intraoperative CA in a 7-month-old child undergoing an extensive retroperitoneal mass in the topography of the left kidney, with a remarkable displacement of the great vessels. The etiology of the CA was attributed to the compression of the aorta and vena cava, exacerbated by muscle relaxation with rocuronium, and critical impairment of the venous return. A pharmacologically mediated sympathectomy by the association of a volatile agent (sevoflurane), an opioid, lidocaine, propofol and a beta-blocker may have also contributed to the adverse event.
With regard to the management of CA, the patient received immediate uninterrupted resuscitation guided by ACLS protocol, until tumor removal. An important parameter was the immediate appearance of ETCO2 on capnography/capnometry, confirming that the external chest compressions were effective, and, thus, generating cardiac output. The resection of the extensive tumor was only possible 40 minutes after the CA, which caused spontaneous cardiac activity to return.
Chest compressions, ventilation, and early defibrillation, when applicable, are the cornerstones of CA treatment [4]. Quality of chest compressions and of CPR in general have been associated with better outcomes in patients with CA [5]. End-tidal carbon dioxide (ETCO2) measurements during resuscitation are indirect measures of pulmonary blood flow, a proxy for overall cardiac output, in the low-flow state generated by chest compressions [6]. In a recent systematic review and meta-analysis on ETCO2 measurements during CPR reflect variable cardiac output over time, and low values have been associated with decreased survival [7]. In our 7-month-old child , ETCO2 was continuously present during CPR, ranging from 42 to 35 mmHg, which certainly contributed to the spontaneous return of cardiac activity and the favorable outcome.
In a meta-analysis carried out in 2022, a total of 397 articles were identified from different databases, including 38 studies with 3.35 million participants, and it showed that the incidence of CA and mortality among children was very high in low-income countries, and were persistent for the last two decades [3]. Factors such as children under the age of one year, ASA status >3, congenital heart disease, and emergency surgery were independent predictors of perioperative CA and mortality. In this case, a huge abdominal mass combined with the induction of general anesthesia, was a fundamental factor for CA.
A retrospective intraoperative study of CA during anesthesia in 218,274 anesthetics of non-cardiac surgery in a US teaching hospital showed that most CA were not related to anesthetic causes [8]. In addition, the study showed that CA related to anesthesia may have a higher survival rate when compared to other possible causes of CA in the operating room. In this child, the prompt start of CPR along with its quality, the skill of the surgical team, as well as the association of neuroprotective drugs like dexmedetomidine and lidocaine in the anesthetic technique may have contibuted with the good global outcome.
In a recent study, the duration of CPR was independently associated with survival to hospital discharge and neurological outcome. Among survivors, the neurological outcome was favorable for most patients [9]. Performing CPR for > 20 minutes is not insignificant in some disease categories of patients, as shown in this case.
Usually, a renal mass is diagnosed by ultrasonography (US), followed by images of the chest, abdomen, pelvis and a CT scan that identifies nephroblastoma of the left kidney, with significant compression of the aorta and inferior vena cava [10]. Ten percent of Wilms tumor patients present with metastases, most commonly in the lung or liver [10]. In this case, no metastases were identified.
During 10 years, children with renal tumors were evaluated, finding 48 children with renal tumor (28 males and 20 females), with Wilms tumor (n=33; 68.8%) being the most common pediatric renal neoplasm [11]. There are two different protocols to treat Wilms tumor: nephrectomy with adjuvant chemotherapy, or neoadjuvant chemotherapy to facilitate surgical removal [12]. In the present case, the choice was the adjuvant regimen.
CONCLUSION
Perioperative CA in children is a rare but catastrophic adverse event, and it is difficult to investigate its incidence, risk factors, causes, and outcomes from these events. Few studies and even case reports on CA in children with cancer under 1 year of age are found in the medical literature.
Rarely, CA can be sudden and unexpected without an initially obvious etiology in an otherwise apparently healthy patient. Huge abdominal masses are risk factors for cardiovascular collapse after the induction of general anesthesia and/or neuraxial blockade. In the present case, we report a 7-month-old child who experienced a sudden CA following anesthetic induction for an extensive tumor urologic procedure. Added to the compression of retroperitoneum vessels some important anesthetics that can provide sympathectomy, possibly contributed to CA after anesthetic induction. On the other hand, the use of a neuroprotective agent like dexmedetomidine may have favored the good outcome after CA. This case also highlights the importance of capnometry during CPR, and it should always encourage continued resuscitation efforts once it shows good pulmonary flow.
REFERENCES
- Ministério da Saúde. Instituto Nacional de Câncer (Brasil). Estimativa 2023: Incidência de Câncer no Brasil / Instituto Nacional de Câncer. Rio de Janeiro : INCA, 2022.
- Gobbo Braz L, Braz JR, Módolo NS, do Nascimento P, Brushi BA, Raquel de Carvalho L. (2006). Perioperative cardiac arrest and its mortality in children. A 9-year survey in a Brazilian tertiary teaching hospital. Paediatr Anaesth. 16:860-866.
- Abate SM, Nega S, Basu B, Tamrat K. (2022). Global mortality of children after perioperative cardiac arrest: A systematic review, meta-analysis, and meta-regression. Ann Med Surg (Lond):1-12.
- Andersen LW, Holmberg JM. Berg KM, Donnino MW. Granfeldt A. (2019). In-Hospital Cardiac Arrest: A Review. JAMA. 321(12):1200-1210.
- Wallace SK, Abella BS, Becker LB. (2013). Quantifying the effect of cardiopulmonary resuscitation quality on cardiac arrest outcome: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 6(2):148-156.
- Steedman DJ, Robertson CE. (1990). Measurement of end-tidal carbon dioxide concentration during cardiopulmonary resuscitation. Arch Emerg Med. 7(3):129-134.
- Hatmann SM, Farris RWD, Di Gennaro JL, Roberts JS. (2015). Systematic review and meta-analysis of end-tidal carbon dioxide values associated with return of spontaneous circulation during cardiopulmonary resuscitation. J Intensive Care Med. 30(7):426-435.
- An JX, Zhang LM, Sullivan EA, Guo QL, Williams JP. (2011). Intraoperative cardiac arrest during anesthesia: a retrospective study of 218,274 anesthetics undergoing non-cardiac surgery. Chin Med J (Engl). 124:227-232.
- Matos RI, Watson RS, Nadkarni VM, Huang HH, Berg RA, Meaney PA, et al. (2013). Duration of cardiopulmonary resuscitation and illness category impact survival and neurologic outcomes for in-hospital pediatric cardiac arrests. Circulation. 127:442-451.
- Aldrink JH, Heaton TE, Dasgupta R, Lautz TB, Malek MM, Abdessalam SF, et al. (2019). Summary article: Update on Wilms tumor. J Pediatr Surg. 54(3):390-397.
- Bozlu G, Çitak EÇ. (2018). Evaluation of renal tumors in children. Turk J Urol. 44(3):268-273.
- Dome JS, Perlman EJ, Graf N. (2014). Risk stratification for Wilms tumor: Current approach and future directions. Am Soc Clin Oncol Educ Book. 2014:215-223.