Information Links
Related Conferences
Current Issue Volume 10, Issue 1 - 2025
MLC Leaf Adjustment for Direct-Aperture Optimization Treatment Planning
Dangling Wu1, Ahmed Eldib2, Lili Chen2, CM Charlie Ma2,*
1Radiation Oncology Department, Guangxi People’s Hospital, Nanning, China
2Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, USA
*Corresponding author: Dr. CM Charlie Ma, Ph.D. Radiation Oncology Department Fox Chase Cancer Center, 333 Cottman Avenue Philadelphia, PA 19111, USA, Tel: (215) 728-2996, Fax: (215) 728-4789, Email: [email protected]
Received Date: December 27, 2024
Published Date: January 21, 2025
Citation: Wu D, et al. (2025). MLC Leaf Adjustment for Direct-Aperture Optimization Treatment Planning. Mathews J Cancer Sci. 10(1):50.
Copyrights: Wu D, et al. © (2025).
ABSTRACT
Direct-aperture optimization (DAO) combines both dose optimization and leaf sequencing in the same optimization process. Due to the random selection of aperture shapes it is often time- consuming to find optimal aperture shapes in DAO and prone to target hot/cold spots. This study investigates MLC leaf position optimization for DAO treatment planning. Fifteen patients were unarchived from our clinical database, who were previously planned using the Varian Eclipse treatment planning system. These patients were re-planned using Prowess RT Pro with the same beam angles, dose constraints and optimization parameters. Manual MLC leaf adjustment was performed for these RT Pro plans to remove hot spots inside the target and cold spots near the target border. Plan quality was evaluated using the homogeneity index (HI), conformity index (CI), Dmax (D1%), and Dmin (D99%) for IMRT/VMAT, and R50% and D2cm for SBRT, and dose- volume and Dmean for organs at risk (OAR). Treatment plan quality was significantly improved after adjusting MLC leaf positions following four simple rules for RT Pro plans generated using the DAO algorithm. The removal of hot spots inside the target and cold spots near the target border improved CI, HI and OAR mean doses as well as OAR dose-volume parameters. Minor adjustment of aperture shapes and/or removal of ineffective segments for RT Pro plans could significantly improve the plan quality to generate identical superior treatment plans as original Eclipse plans. The method developed in this work can be further programmed as a post- optimization tool to improve treatment planning quality and efficiency.
Keywords: Multileaf Collimator (MLC), Intensity Modulated Radiation Therapy (IMRT), Radiobiology, Direct-Aperture Optimization (DAO), Treatment Planning.
INTRODUCTION
Modern radiation therapy (RT) employs various imaging guidance techniques in the entire radiotherapy treatment process to facilitate target and critical structure delineation, treatment planning and pre-treatment quality assurance, patient treatment setup and target localization, and real-time treatment verification and outcome assessment. Recent RT developments in advanced delivery techniques such as intensity modulated radiotherapy (IMRT) and volumetric modulated arc therapy (VMAT) together with precise target localization techniques have enabled dose escalation and hypo-fractionation clinical trials for prostate cancer that also utilized stereotactic body radiation therapy (SBRT) techniques [1-5].
Advanced treatment planning systems (TPS) play an important role in modern RT treatment techniques, which relie on accurate dose calculation, advanced optimization algorithms and efficient multileaf collimator (MLC) leaf sequences to generate high-quality treatment plans. Treatment plan optimization can be achieved by either a two-step approach (e.g., beamlet-based intensity map optimization followed by MLC leaf sequencing) or a direct-aperture (e.g., MLC segment) optimization algorithm. For beamlet-based IMRT optimization, a fluence map is optimized for each beam angle. Then, a leaf sequence is determined that will closely reproduce the fluence map to achieve the planned dose distribution. However, the leaf sequence is constrained by machine parameters such as gantry rotation speed, collimator jaw/MLC leaf speed and radiation dose rate. A variation of dose distribution and delivery efficiency is inevitable [6]. For example, beamlet weights are stratified in intensity levels to improve delivery efficiency, and intensity levels are further grouped [7] or smoothed in leaf sequencing/plan optimization [8,9]. However, such attempts are often associated with the decrease of plan quality although sometimes it is used to improve a particular dose quantity, e.g., the maximum dose in the target volume. As a result, the final deliverable plan often cannot reproduce the “perfect” dose distribution from the initial optimization process in a beamlet-based approach.
In contrast, the DAO approach uses a set of apertures for optimization and the MLC segments (i.e., leaf opening shapes) are deliverable directly and can be delivered sequentially, eliminating the leaf-sequencing step. Thus, the delivered dose distribution is the same as the optimized dose distribution without losing plan quality and delivery efficiency. The machine parameters such as dose rate, gantry rotation speed, and MLC leaf characteristics (leaf speed, tongue and groove effect, minimum gaps between opposing leaves and opposing adjacent leaves due to interdigitation) can also be considered in the optimization process [10-13]. The number of apertures can be set to reduce the delivery complexity of IMRT/VMAT plans, which is useful to older linac models with limited MLC capabilities. Aperture-based optimization is also key to VMAT because it is theoretically a sequential aperture delivery with gantry rotation.
DAO was proposed to handle the complexity of IMRT optimization using a stochastic approach. But the stochastic approach is computationally intensive and time-consuming due to the nature of the random sampling process, and the optimization result remains random. Previous studies have shown that DAO can produce IMRT plans comparable with those by beamlet-based optimization when the number of MLC segments per gantry angle is above 10. A further reduction in the segments and monitor units can be achieved by DAO, reducing the complexity of a plan to facilitate machine delivery. However, the target dose heterogeneity (e.g., the maximum/minimum target dose) may become worse because of the reduced number of apertures and faster optimization time [14-20].
This study investigates MLC leaf position optimization for DAO treatment planning. Previously treated patients were unarchived from our clinical database and replanned using the DAO algorithm with the same beam angles, dose constraints and optimization parameters. Manual MLC leaf position adjustments were performed for these treatment plans to remove hot spots inside the target and cold spots near the target border. Original treatment plans were compared to new treatment plans with and without MLC leaf position adjustments and the plan quality was evaluated using various dosimetric parameters for the target and organs at risk (OAR).
MATERIALS AND METHODS
This study is a retrospective dosimetric analysis of treatment plans for previously treated patients. Treatment plans of 15 anonymized patients were unachieved from our clinical database, who were previously planned using the Eclipse TPS (version 13.6, Varian Medical Systems, Palo Alto, CA) and treated on the Trilogy/iX accelerators (Varian Medical Systems, Palo Alto, CA) during 2019 to 2020.
These patients were re-planned using the RT-Pro TPS (version 5.60.4657, Prowess Inc., Concord, CA), which employs the DAO optimization algorithm. CT images and structure sets in Eclipse were DICOM exported to Prowess. The same prescription dose for the planning target volume (PTV) and OAR constraints were used in the re-planning process. For IMRT planning, the same beam configurations, dose metrics and delivery techniques were used as those in the original plans to facilitate a direct comparison of the optimization techniques. For VMAT planning, the same arc arrangements, dose metrics and delivery techniques were used. In some VMAT cases, partial arcs were used to avoid passing through critical structures. This was essentially a beam-orientation optimization but it consequently reduced the solution space as a result of fewer beam angles available for the optimization process. The dose calculation was performed using the collapsed cone convolution (CCC) algorithm [21]. All the treatment plans were deemed clinically acceptable by experienced planners and physicians.
Manual MLC leaf position adjustments were made to these RT Pro plans to remove hot spots inside the target and cold spots near the target border to improve the plan quality. This was achieved using four simple operations: (1) “Pull-in” those MLC leaves that are outside the target volume to reduce unnecessary dose outside the PTV; (2) “Push-out” those MLC leaves that are near the target border to increase target dose near the PTV edges; (3) “Open-up” those MLC leaves inside the target to remove “cold spots” within the PTV; and (4) “Close-off” those MLC leaves that are inside the target to reduce “hot spots” within the PTV.
Plan quality was evaluated between the original Eclipse plans and the new RT Pro plans with and without MLC leaf position adjustments using various dosimetric parameters including the maximum dose, Dmax (D1%), the minimum dose, Dmin(D99%), the homogeneity index (HI), which is defined as the ratio of Dmax/Dmin, and the conformity index (CI), which is defined as the ratio of the prescription isodose volume (PIV) to PTV, for the target for IMRT/VMAT, and R50%, which is the ratio of the 50% prescription isodose volume to PTV, and D2cm , which is the maximum dose (in % of the prescription dose) at a point 2 cm away from the PTV surface in any direction for SBRT, and dose-volume histogram and Dmean for OARs. Statistical analyses were performed using a paired Student’s t-test for normal distribution and a Wilcoxon signed rank tests for non-normal distribution using GraphPad Prism to determine the difference. If the P value was less than 0.05, it was statistically significant.
RESULTS
The four simple operations for MLC leaf adjustments can be used separately or jointly for a photon field. Figure 1 illustrates how to “pull-in” MLC leaves to reduce doses to normal tissues outside the target volume and to improve the dose conformity and gradient around the target border. Some random MLC leaf openings contribute little to the target dose and sometimes are simply the result of the insensitivity of the objective function to the normal tissue dose (e.g., no or weak constraints to the normal tissues involved), which can be either completely closed or partially closed based on the electron range and tissue density through this “pull-in” operation. Reversely, MLC leaves can be opened more to increase the dose near the target edges by the “push out” operation. The dose distribution is calculated after these operations and the changes are accepted if they improve the overall dose distribution (e.g., some operations such as “open up” or “close off” inside the target volume may not only change the hot or cold spots locally but also affect the dose distribution globally such as target coverage or surrounding dose gradient).
.png)
Figure 1. The MLC leaf openings of an original RT Pro plan optimized using DAO (a) and the adjusted leaf openings of the same plan (b). The target volume is shown in brown. Here MLC openings outside the target are pulled in to improve target dose conformity and normal tissue dose.
Figure 2 shows “pull-in”, “push out” and “close-off” operations in the same photon field. A hot spot of 110% prescription dose (upper arrow) can be easily removed by closing off a leaf.
Reversely, cold spots inside the target volume can be improved using the “open up” operation for selected beam angles where MLC leaves can be open more to increase the local dose. The MLC leaf openings (lower arrow) can be pulled in (lower borders) to improve the target dose conformity and reduce the dose to normal tissues or pushed out (upper borders) to increase the dose at the target edges. As seen in the figure, yellow block margin contours were used to guide the “pull in” and “push out” operations. The block margin is usually variable surrounding the target volume based on the local issue density and thus electron range.
.png)
Figure 2. The MLC leaf openings of an original RT Pro plan optimized using DAO (a) and the adjusted leaf openings of the same plan (b). The target is contoured in brown and the yellow contours are added block margins used as a guide to pull in or push out the MLC leaves. The top arrow points to a hot spot (blue line: the 110% of the prescription dose) in the target volume, which was removed by closing off a leaf. The lower arrow points to larger MLC leaf openings that can be pulled in to improve the target dose conformity and reduce normal tissue dose.
Figure 3 shows the axial view of the CT image and one of the beam incident directions for a RT Pro treatment plan in (a) and the MLC leaf openings for the selected photon field in (b). The target is contoured in blue and the 100% and 90% isodose lines are shown in yellow and red, respectively. The arrows in both figures point at the area of the target receiving doses below the prescription dose. The MLC leaf openings at the arrow location can be pushed out to boost the dose locally (likely because low density lung requires more build-up regions surrounding the target). The MLC leaves on the lower field edge in Fig. 3 (b) can be opened more to boost the local dose as well.
.png)
Figure 3. The axial view of the patient geometry and an incident beam direction (a) of a RT Pro treatment plan and the MLC leaf openings for the beam angle (b). The target is contoured in blue and the yellow and red isodose lines show 100% and 90% of the prescription doses, respectively. The arrow points to the cold spots in the target volume where MLC leaves can be opened more to improve target coverage.
Generally, treatment plan quality can be improved after adjusting MLC leaf positions following the four simple rules for RT Pro plans generated using the DAO algorithm, and sometimes significant improvement was possible. Figure 4 shows the axial, sagittal and coronal views of the target (in red) and the prescription isodose lines (in yellow) of an original RT Pro plan for a lung cancer treatment in (a) and the corresponding target and isodose lines for the same plan after the MLC-leaf adjustments (b). The target coverage is much improved, and the CI is reduced from 1.07 for the original plan to 1.00 for the adjusted plan. Figure 5 shows similar dose conformity improvement for a prostate treatment plan with MLC-leaf adjustments. The CI is improved from 1.11 for the original plan to 1.04 for the adjusted plan. Since the MLC leaf adjustments are generally small, the changes to the prescription isodose lines are minor and mainly around the target edges to improve the dose conformity. Therefore, only small differences are seen for lower isodose lines further away from the target.
.png)
Figure 4. The axial, sagittal and coronal views of the lung cancer target and the prescription isodose lines of a RT Pro treatment plan before (a) and after the MLC leaf openings are adjusted (b). The target is shown in red and the prescription isodose lines are in yellow.
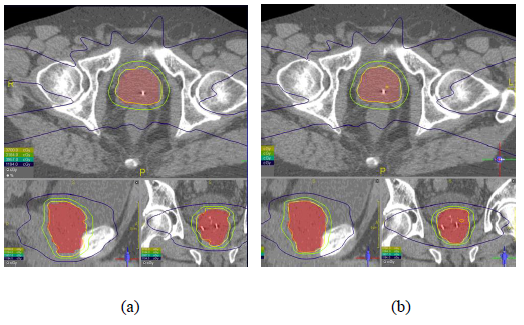
Figure 5. The axial, sagittal and coronal views of the prostate target and the isodose lines of a RT Pro treatment plan before (a) and after the MLC leaf openings are adjusted (b). The target is shown in red and the prescription isodose lines are in yellow.
The planning quality of the Prowess RT Pro system with the DAO approach is similar to that of the Varian Eclipse TPS with beamlet-based optimization. With finer MLC leaf position adjustments, it is possible to further improve the RT Pro planning quality for some patients.
Figure 6 shows a brain IMRT case with significant improvement in target coverage and OAR dose sparing after MLC leaf adjustments. The CI is reduced from 1.08 for the original RT Pro plan to 0.99 for the MLC-leaf adjusted plan. The DHV curves for the left and right optical nerves are much improved by slightly adjusting the MLC leaf positions as can be seen in Fig. 6 (c).
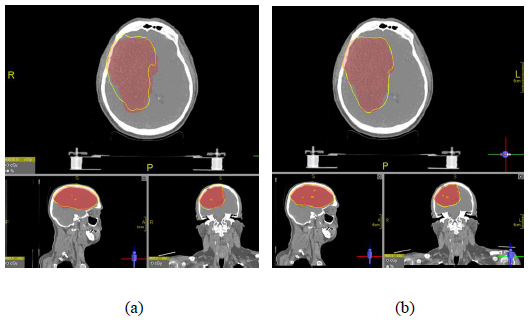
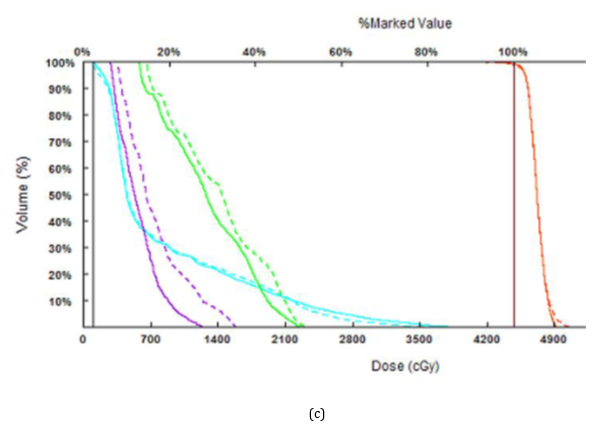
Figure 6. The axial, sagittal and coronal views of a brain IMRT case and the isodose lines of the RT Pro treatment plan before (a) and after the MLC leaf adjustments (b), and their DVH comparison (c). The target is shown in red and the prescription isodose lines are in yellow. Solid lines show DVHs for the target (red), brain stem (light blue), right optical nerve (green) and left optical nerve (purple) for the MLC leaf-adjusted plan and dashed lines show DVHs for the original plan.
For the same brain IMRT case, the original Prowess RT Pro plan shows similar plan quality as that of the Varian Eclipse treatment plan in terms of target coverage and OAR sparing. However, the MLC-leaf adjusted RT Pro plan can further improve the target cold spots and OAR dose distributions, as shown in Fig. 6. The CI for the MLC-adjusted RT Pro plan is improved to 0.99, which is comparable to that of the Eclipse plan, which is 1.00. Since the TPS can only compare two treatment plans at the same time, the isodose distributions and the DVH curves are presented separately in Figs. 6 and 7. The DVH curves for critical structures (brain stem, left and right optical nerve) with MLC leaf adjustments are significantly improved compared to those of the original Prowess RT Pro plan (Fig. 6) and of the Varian Eclipse plan (Fig. 7), indicating that the MLC leaf position optimization technique may be beneficial to treatment plans generated by Varian Eclipse TPS as well.
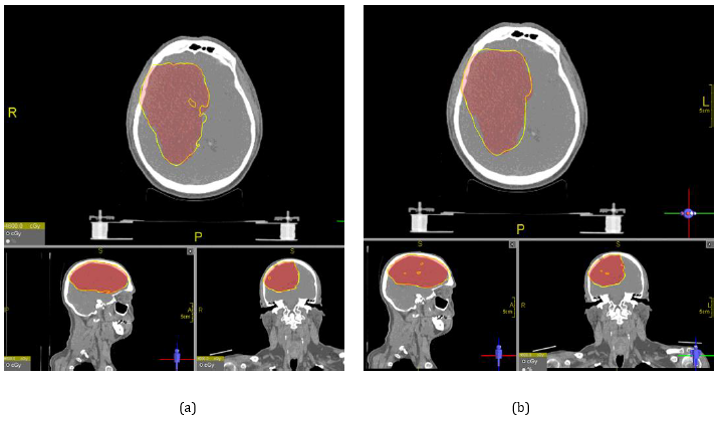
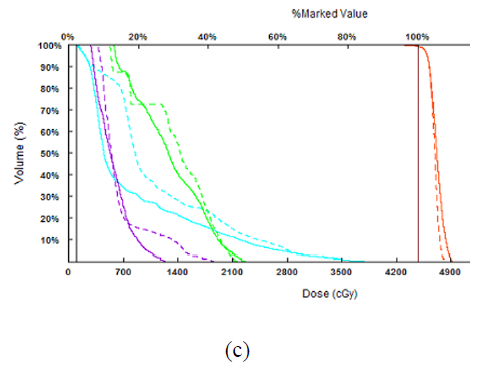
Figure 7. The axial, sagittal and coronal views of a brain IMRT case and the isodose lines of the Varian Eclipse treatment plan (a) and the Prowess RT Pro plan after the MLC leaf adjustments (b), and their DVH comparison (c). The target is shown in red and the prescription isodose lines are in yellow. Solid lines show DVHs for the target (red), brain stem (light blue), right optical nerve (green) and left optical nerve (purple) for the MLC leaf-adjusted RT Pro plan and dashed lines show DVHs for the Eclipse plan.
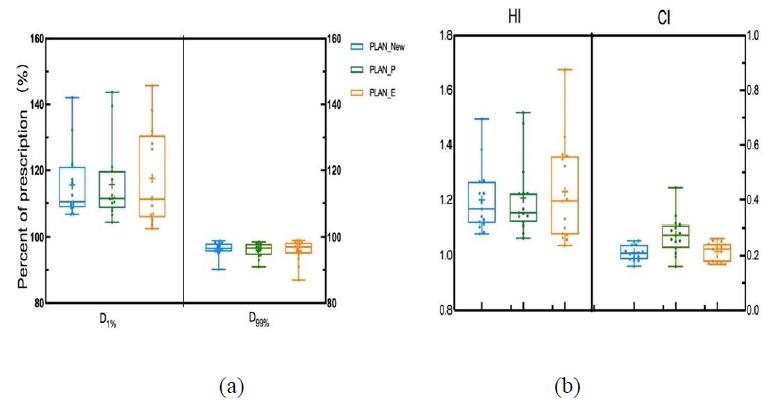
Figure 8. The maximum dose (D1%) and minimum dose (D99%) for the PTV (a), the dose heterogeneity index (HI) and dose conformity index (CI) for the PTV (b) of 15 original Varian Eclipse plans (PLAN_E), retrospective Prowess RT Pro plans (PLAN_P) and MLC leaf adjusted RT Pro plans (PLAN_New).
Detailed dosimetric comparisons are made between the original 15 Varian Eclipse plans and the retrospective Prowess RT Pro plans with and without MLC leaf adjustments. Figure 8 shows the maximum dose, minimum dose, dose heterogeneity and dose conformity for the PTV of all treatment plans investigated. It is apparent that MLC leaf adjustment can effectively reduce target hot and cold spots and significantly improve target dose conformity and heterogeneity for Prowess RT Pro plans. All treatment plans show similar target dose maximum and minimum, but the RT Pro plans exhibit smaller variation in D1% and D99% compared to the Eclipse plans. The target dose is less heterogenous for the RT Pro plans in comparison to the Eclipse plans, while the target dose is equally conformal between the Eclipse plans and the RT Pro plans after MLC leaf adjustments. It should be mentioned that all Eclipse and RT Pro plans meet the departmental acceptance criteria for clinical treatment.
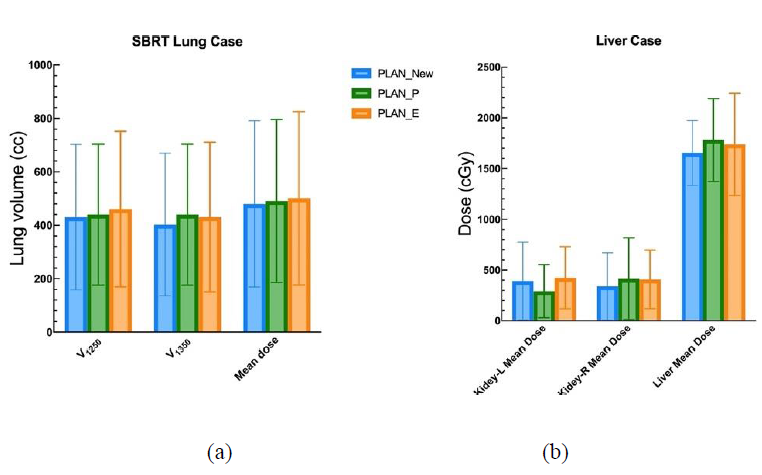
Figure 9. Comparison of OAR dose volumes for lung (a) and liver (b) treatments of Varian Eclipse plans (PLAN_E), retrospective Prowess RT Pro plans (PLAN_P) and MLC leaf adjusted RT Pro plans (PLAN_New).
Figure 9 demonstrates the improvement in the OAR doses for SBRT lung cancer and IMRT/VMAT liver cancer treatment. Both the mean lung dose and other lung dose-volume parameters are improved for RT Pro plans with MLC leaf adjustments, which make their plan quality better compared to Eclipse plans (Fig. 9a). The same can be seen for the liver plans in which both the mean liver dose and the mean doses for the left and right kidneys for RT Pro plans with MLC leaf adjustments are lower than those of Eclipse plans (Fig. 9b). Figure 10 compares the OAR doses between RT Pro plans and Eclipse plans for IMRT/VMAT prostate treatment. MLC leaf adjustments can significantly improve the mean doses of the rectum and bladder (Fig. 10a) and all other dose-volume parameters (Fig. 10b) for the RT Pro treatment plans although the Eclipse plans still show better quality in these parameters.
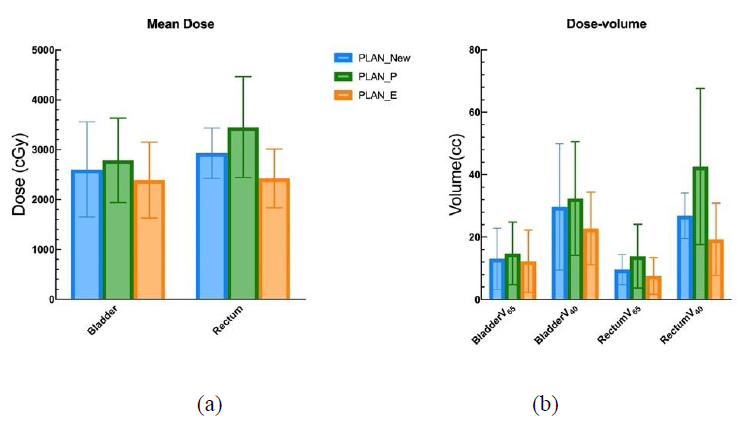
Figure 10. Comparison of mean doses to the rectum and bladder (a) and dose volumes for the same organs (b) for prostate treatment of Varian Eclipse plans (PLAN_E), retrospective Prowess RT Pro plans (PLAN_P) and MLC leaf adjusted RT Pro plans (PLAN_New).
DISCUSSION
In this study, we have investigated a manual MLC leaf position optimization technique to improve the quality of treatment plans generated using the Prowess RT Pro system with the DAO algorithm. This technique is different from those leaf optimization methods that were part of the step-and-shoot IMRT leaf sequencing algorithm [8,9,22]. The random nature of DAO may result in MLC segments that are less ideal in the target region and around the target/OAR boundaries especially with limited iterations in the optimization process. Finer adjustments of the MLC leaf position by either opening or closing MLC leaves based on beamlets or taking smaller steps within a beamlet (also see below) can further optimize the shape of the leaf opening to remove hot spots inside the target or cold spots at the target edges, and sometimes can lead to significant improvement in target coverage and critical structure sparing. This optimization strategy is being implemented in the Prowess RT Pro TPS as an additional step in the DAO- based optimization process to improve the treatment plan quality.
This MLC leaf position optimization technique may also work for other treatment planning systems that employ different optimization algorithms. Since MLC-based dose delivery generally use finite-size pencil beam algorithms for pre-optimization beamlet dose calculation, the MLC leaf positions are discrete and correlated with the beamlet size (e.g., MLC leaf width and preset step length), which may not be ideal in the target region or around the target/OAR boundaries causing hot/cold spots as with a DAO algorithm (either due to the optimization algorithm or the discrete MCL step). Finer adjustments of the MLC leaf positions can optimize the shapes of the MLC segments in the same manner as for the DAO generated treatment plans to improve the plan quality for other treatment planning systems.
Finally, it should be noted that this work was done with Varian Eclipse treatment plans from only 15 previously treated patients. The results and quality improvement scale may vary depending on the TPS used and individual plan details. Although only some MLC leaf position adjustments may be needed to improve the quality of a plan, any accepted MLC leaf adjustments will bring incremental and definitive dosimetric benefits to the plan. Thus, this technique will be useful to most treatment plans optimized with DAO or other beamlet-based optimization algorithms. It should also be stressed that finer dose calculation grids (wrt the beamlet size) are needed to calculate the changes in dose distribution if the leaf position adjustment is smaller than the size of the beamlet.
CONCLUSIONS
Minor adjustment of MLC aperture shapes and/or removal of invalid segments for DAO generated plans could significantly improve the plan quality to generate identical superior treatment plans using Eclipse and RT Pro TPS employing either DAO and/or beamlet-based approach. The method developed in this work can be further programmed as a post-optimization tool to improve treatment planning effectiveness and efficiency.
ACKNOWLEDGMENTS
Technical support from Prowess Inc. is greatly appreciated for DAO treatment planning and MLC leaf position optimization using the Panther TPS.
CONFLICT OF INTEREST
Authors declare that there is no conflict of interest.
REFERENCES
- Ma CM. (2011). Adaptive radiation therapy for prostate cancer, in Adaptive Radiation Therapy. Ed. X. Allen Li. CRC Press, New York, USA. pp. 331-350.
- De Los Santos J, Popple R, Agazaryan N, Bayouth JE, Bissonnette JP, Bucci MK, et al. (2013). Image guided radiation therapy (IGRT) technologies for radiation therapy localization and delivery. Int J Radiat Oncol Biol Phys. 87(1):33-45.
- Dang A, Kupelian PA, Cao M, Agazaryan N, Kishan AU. (2018). Image-guided radiotherapy for prostate cancer. Transl Androl Urol. 7(3):308-320.
- Grégoire V, Guckenberger M, Haustermans K, Lagendijk JJW, Ménard C, Pötter R, et al. (2020). Image guidance in radiation therapy for better cure of cancer. Mol Oncol. 14(7):1470-1491.
- Ma CM. (2019). Physics and Dosimetric Principles of SRS and SBRT. Mathews J Cancer Sci. 4(2):22.
- Cho PS, Marks RJ 2nd. (2000). Hardware-sensitive optimization for intensity modulated radiotherapy. Phys Med Biol. 45(2):429-440.
- Wu Y, Yan D, Sharpe MB, Miller B, Wong JW. (2001). Implementing multiple static field delivery for intensity modulated beams. Med Phys. 28(11):2188-2197.
- Spirou SV, Fournier-Bidoz N, Yang J, Chui CS, Ling CC. (2001). Smoothing intensity-modulated beam profiles to improve the efficiency of delivery. Med Phys. 28(10):2105-2012.
- Siebers JV, Lauterbach M, Keall PJ, Mohan R. (2002). Incorporating multi-leaf collimator leaf sequencing into iterative IMRT optimization. Med Phys. 29(6):952-959.
- Niemierko A. (1992). Random search algorithm (RONSC) for optimization of radiation therapy with both physical and biological end points and constraints. Int J Radiat Oncol Biol Phys. 23(1):89-98.
- Shepard DM, Earl MA, Li XA, Naqvi S, Yu C. (2002). Direct aperture optimization: a turnkey solution for step-and-shoot IMRT. Med Phys. 29(6):1007-1018.
- Cotrutz C, Xing L. (2003). Segment-based dose optimization using a genetic algorithm. Phys Med Biol. 48(18):2987-2998.
- Yu C, Shepard D, Earl M, Cao D, Luan S, Wang C, Chen DZ. (2006). New developments in intensity modulated radiation therapy. Technol Cancer Res Treat. 5(5):451-464.
- Lo A, et al. (2004). Quantitative comparison of aperture-based and beamlet-based inverse planning techniques. Int J Radiat Oncol Biol Phys. 60(1):s630-s630.
- Xiao Y, Werner-Wasik M, Michalski D, Houser C, Bednarz G, Curran W, et al. (2004). Comparison of three IMRT inverse planning techniques that allow for partial esophagus sparing in patients receiving thoracic radiation therapy for lung cancer. Med Dosim. 29(3):210-216.
- Ahunbay EE, Chen GP, Thatcher S, Jursinic PA, White J, Albano K, et al. (2007). Direct aperture optimization-based intensity-modulated radiotherapy for whole breast irradiation. Int J Radiat Oncol Biol Phys. 67(4):1248-1258.
- Dobler B, Pohl F, Bogner L, Koelbl O. (2007). Comparison of direct machine parameter optimization versus fluence optimization with sequential sequencing in IMRT of hypopharyngeal carcinoma. Radiat Oncol. 2:33.
- Broderick M, Leech M, Coffey M. (2009). Direct aperture optimization as a means of reducing the complexity of Intensity Modulated Radiation Therapy plans. Radiat Oncol. 4:8.
- Qi P, Xia P. (2013). Relationship of segment area and monitor unit efficiency in aperture-based IMRT optimization. J Appl Clin Med Phys. 14(3):4056.
- Smilowitz JB, Das IJ, Feygelman V, Fraass BA, Kry SF, Marshall IR, et al. (2015). AAPM Medical Physics Practice Guideline 5.a.: Commissioning and QA of Treatment Planning Dose Calculations - Megavoltage Photon and Electron Beams. J Appl Clin Med Phys. 16(5):14-34.
- Luong O, et al. (2019). Dosimetric evaluation of lung treatment plans produced by the Prowess Panther system using Monte Carlo simulation. Biomedical Physics & Engineering Express. 5(5):055005.
- De Gersem W, Claus F, De Wagter C, Van Duyse B, De Neve W. (2001). Leaf position optimization for step-and-shoot IMRT. Int J Radiat Oncol Biol Phys. 51(5):1371-1388.