Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
Low Health Literacy (LHL): A Devious Enemy of Patient Treatment Adherence
Abdul Kader Mohiuddin*
Alumni, Faculty of Pharmacy, Dhaka University, Bangladesh
*Corresponding author: Abdul Kader Mohiuddin, Alumni, Faculty of Pharmacy, Dhaka University, Bangladesh. Tel: +01706221174, ORCID: 0000-0003-1596-9757, Web of Science Researcher ID: T-5428-2019; E-mail: [email protected].
Received Date: January 25, 2023
Published Date: March 16, 2023
Citation: Mohiuddin AK. (2023). Low Health Literacy (LHL): A Devious Enemy of Patient Treatment Adherence. Mathews J Psychiatry Ment Health. 8(2):38.
Copyrights: Mohiuddin AK. © (2023).
ABSTRACT
People must have certain personality traits and social resources, referred to as health literacy, to access, comprehend, and use the information to make health decisions. Patients' ability to manage complex diseases and care for themselves is strongly related to their level of health literacy. It can help us stay healthy by preventing illness and managing existing illnesses effectively. People with low health literacy (LHL) may struggle to manage their condition and prevent illness, leading to increased use of healthcare services. Furthermore, LHL is associated with more hospitalizations, elevated use of emergency care, decreased use of preventative services, and a decreased ability to understand labels and health messages, as well as a worsened state of health, higher mortality, and more expensive medical care.
Keywords: Parental Health Literacy, Necessary Health Education, Understanding Treatment Guidelines, Medication Non-Adherence, Healthcare, Avoidable Medical Costs, Global Health Burden, COVID-19 Vaccine Negligence.
ABBREVIATIONS
ADHD: Attention Deficit Hyperactivity Disorder; ASD: Autism Spectrum Disorder; AUD: Alcohol Use Disorder; CDC: US Centers for Disease Control and Prevention; COVID-19: Coronavirus Disease 2019; ED: Emergency Department; MC: Medical Cannabis; SMBG: Self-Monitoring of Blood Glucose; SUD: Substance Use Disorder; UNODC: UN Office on Drugs and Crime.
INTRODUCTION
"Health literacy" refers to the ability to comprehend common healthcare communications such as prescription instructions, test results, and insurance forms. Health literacy increases a population's ability to care for itself and helps to reduce health disparities. It influences the utilization of healthcare services, as well as patient satisfaction and physician-patient interaction. It is one of the major barriers to healthcare professionals effectively communicating information to those in their care. Personal health literacy corresponds to a person's quest to reach, understand, and apply information and services to help them and others make health-related decisions and actions. The World Health Organization recommends health literacy as a tool for achieving several important targets outlined in the Sustainable Development Goals. Many factors can affect a person's health literacy, including medical terminology knowledge, understanding of how the health care system works, ability to communicate with health care providers, and ability to locate health information, which may be related to age, income, education, language skills, and culture, and physical or psychological limitations. Treatment adherence is influenced by health literacy, which may have an impact on treatment outcomes. Despite the negative implications of LHL, clinicians are frequently unaware of their patients' levels of health literacy and the consequences for their patients' outcomes.

Figure 1. Graphical Abstract Health Literacy.
MATERIAL AND METHODS
Prioritized databases for public health topics included PubMed, ALTAVISTA, Embase, Scopus, Web of Science, and the Cochrane Central Registers. Along with other online sources, journals from Elsevier, Springer, Willey Online Library, and Wolters Kluwer were thoroughly searched. The infographic was prepared by Canva Illustrator, and the citation work was done by citationmachine.net.
Literature Review
Numerous studies have shown that patients from high-income nations do not consistently take their medications as directed. The reasons for non-adherence to diabetes management protocols in Middle Eastern nations include forgetfulness, a lack of clarity regarding the length of time that medication must be taken, and a lack of confidence in the medication's overall efficacy [1]. Taiwan, on the other hand, experienced extreme poverty following World War II, but today it has Asia's eighth-largest economy and is home to more than 80% of type 2 diabetes patients [2]. LHL is a widespread issue in Asia, Europe, and Africa. The three European nations with the lowest health literacy are Bulgaria, Lithuania, and Latvia [3]. LHL is most prevalent in rural areas and among people with low levels of education around the world. Surprisingly, LHL affects 50% of people in both developed and developing nations [4].
Prevalence, Reasons and Global Burden with LHL
The demands and complexities of the healthcare system combined with a person's aptitudes result in health literacy. Medical practices in a nation, as well as individual and social factors at play in interactions between people and the systemic requirements of the healthcare system, all have a significant impact on health literacy. The majority of the time, LHL is associated with older people with chronic illnesses who have little education and are not necessarily from lower socioeconomic backgrounds. Additionally, LHL is influenced by socioeconomic disadvantage, membership in an ethnic minority, higher psychological distress, physical limitations, inadequate social support, compromised mental health, and poor quality of life. Being literate in general does not necessarily translate into being literate in health [5,6]. However, in this submission, a few more sensational facts in the form of an infographic model about LHL are shared (Figure 1). However, this submission shares some additional sensational information about LHL in the form of an infographic model (Figure 1).
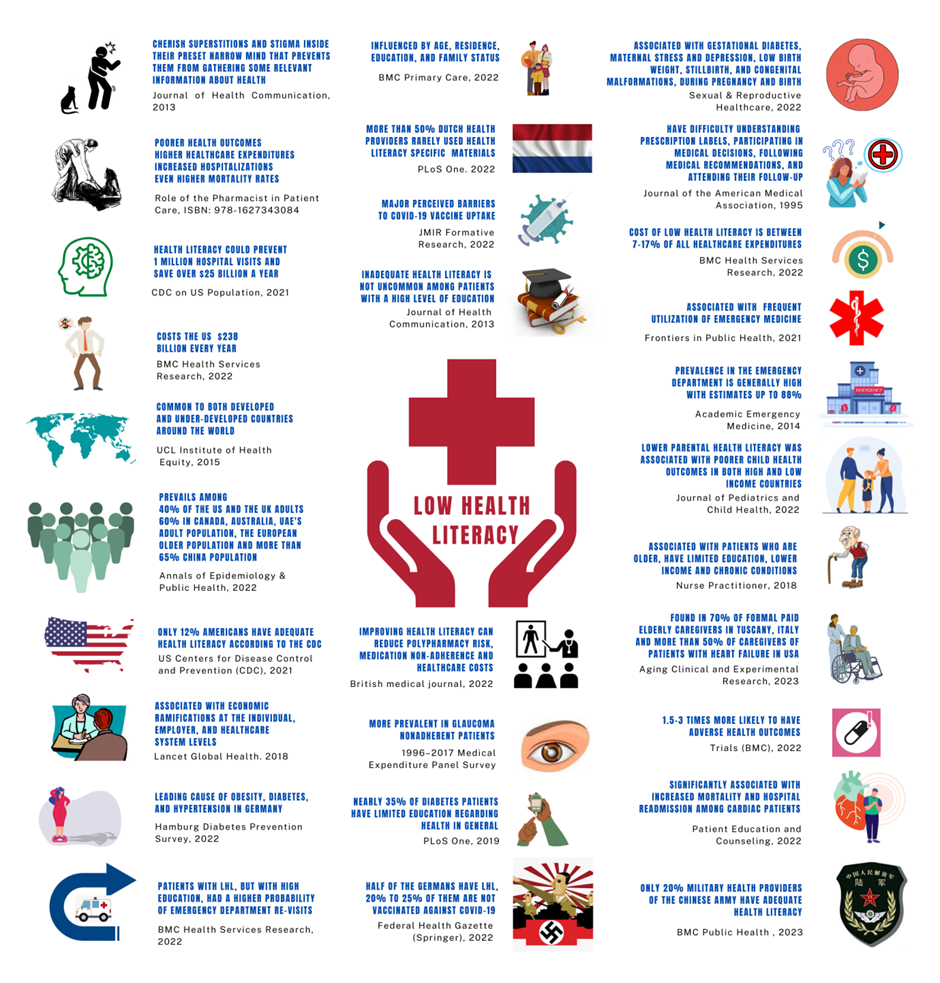
Figure 2. Low Health Literacy Facts.
- LHL is linked to individuals who value stigma and superstition within their preconceived, small minds, preventing them from gathering pertinent health information from their surroundings [5].
- LHL significantly affects how well patients follow their treatment plans or, more specifically, how well they take their medications, which harms health outcomes, raises healthcare costs, boosts hospitalizations, and even raises mortality rates [6].
- According to the US Centers for Disease Control and Prevention (CDC), only 12% of Americans have adequate health literacy, and increasing health literacy could prevent nearly 1 million hospital admissions and save more than $25 billion annually [7].
- Although it is estimated that illiteracy costs the global economy $1.19 trillion, LHL alone costs the US economy $238 billion annually [8].
- Worldwide, LHL is a problem in both developed and developing nations, and its causes are not solely socioeconomic [9].
- Surprisingly, only about 50% of adults in Europe, 60% of adults in Canada, Australia, and the United Arab Emirates, and nearly 70% of Chinese adults have LHL [10].
- Health literacy in China increased from 6.48% in 2008 to 23.15% in 2020 [11]. However, a recent study published in BMC Public Health [12] found that only 1 in 5 military healthcare providers in the Chinese People's Liberation Army had adequate health literacy.
- Evidence demonstrates that LHL has substantial economic effects on individuals, employers, and the healthcare system [13].
- LHL is a significant risk factor for the three conditions that make up the metabolic syndrome: obesity, diabetes, and hypertension, according to the authors of the Hamburg Diabetes Prevention Survey, a population-based cross-sectional study conducted in Germany [14].
- Health literacy is influenced by a person's age, place of residence, level of education, and family situation [15].
- The use of health literacy-specific resources is rare among more than half of Dutch healthcare professionals [16].
- Evidence supporting the idea that mistrust and LHL perceptions act as perceived obstacles to COVID-19 vaccine uptake was found to be associated with high levels of vaccine hesitancy [17].
- LHL is not uncommon among patients with a high level of education or with well-off patients. Moreover, patients with LHL, but with high education, had a higher probability of emergency department (ED) re-visits. Empirical research based on a conceptual model estimated that LHL costs between 7 and 17% of total healthcare expenditures [8].
- According to patient-centered interventions, improving health literacy can reduce the risk of polypharmacy, medication non-adherence, and healthcare costs [18].
- According to the 1996-2017 Medical Expenditure Panel Survey, LHL was more prevalent in glaucoma patients, and patients with LHL were prescribed more medications and had higher medication costs [19].
- Nearly 35% of diabetic patients worldwide have limited health-related education [20].
- LHL is linked to gestational diabetes, maternal stress and depression, low birth weight, stillbirth, and congenital malformations during pregnancy and birth, all of which have negative consequences for the woman and her child [21].
- Health literacy among the population is expected to rise over time in this era of modernization. According to a national survey conducted in the Czech Republic in 2015-16, nearly 60% of Czechs have LHL. Surprisingly, a 2018 survey revealed that health literacy in the Czech Republic was still declining [22].
- The prevalence of LHL in the ED varies greatly, with estimates as high as 88% depending on the patient mix and screening instruments used [23].
- In both low and high-income countries, low parental health literacy was linked to poorer child health outcomes [24].
- Older patients, who have less education, a lower income, and chronic conditions are more vulnerable [25].
- LHL was discovered in more than 70% of formal paid caregivers of non-self-supporting older adults in Tuscany, Italy, and in more than 50% of caregivers of heart failure patients in the United States [26].
- People with LHL may have 1.5-3 times the number of serious health outcomes, such as higher mortality, hospitalization rates, and disease management ability, as those with adequate health literacy [27].
- In cardiac patients, it has been linked to increased mortality, hospital readmission, and lower quality of life [28].
- LHL represents nearly 50% of Germans [29]. In Germany, every fourth to the fifth person is not immunized against COVID-19 [30].
- According to a Waystar (Health Care Billing Software) report from 2019, nearly 40% of healthcare consumers were unaware that the cost of their healthcare varied across facilities [31]. Factors or Consequences Associated with LHL
Superstitions: an elephant in the room
Superstition is the non-scientific belief in magical connection. Aspects of certain religions and supernatural ideologies, such as astrology, omens, witchcraft, and prophecies, are examples of such beliefs. Even after all of the modernization and enlightenment, superstitious beliefs still exist in our societies. Most people are thought to have irrational, superstitious beliefs to some extent. Epilepsy and schizophrenia are still viewed in the majority of the world as an evil spirit. Although two-thirds of patients could become seizure-free with proper care, poor adherence to proper guidelines is a major problem for effective recovery [32,33]. In an Indian study, 60% of the participants thought that illnesses were the result of luck or superstition [34]. In Northern Germany, superstitions were also reported in nearly 40% of men and 70% of women [35]. 70% of people in Africa use folk remedies like charms and witchcraft to treat their illnesses [36]. Surprisingly, researchers found that 73% of addiction treatment programs in the USA include a spirituality-based element and that more than 40% of Americans believe in spiritual therapies [37,38]. According to a South Iranian study, 60% of diabetic patients refused insulin despite doctor recommendations due to phobia [39]. Menstruation is fraught with taboos, restrictions, and misconceptions in low- and middle-income countries, especially in India and sub-Saharan Africa [40]. In India, nearly 80% of menstruating girls and women use an old cloth that is frequently reused. Further, around 90% of women in India sometimes resort to using ashes, rags, sand, newspapers, dried leaves, wood shavings, hay, plastic and husk sand to aid absorption [41-43]. Additionally, these two areas are home to more than 90% of the world's open defecation practitioners [44,45]. Many superstitious Indians hold the view that defecation is an impure act that should only be performed outside the home and that toilets should only be used in inclement weather [46]. It is not surprising that at least 90% of Indian adults have poor health literacy [47].
Medication or treatment guideline non-compliance
Medication noncompliance accounts for more than half of the $500 billion in total avoidable costs associated with suboptimal medicine use worldwide each year [48]. LHL was linked to increased unintentional non-adherence and poor medication self-management in a variety of domains, including forgetting or having difficulty remembering to take medications. However, no relationship was found between health literacy and intentional non-adherence, which includes stopping medications when feeling better or worse [49]. Studies show that LHL is connected with poorer disease knowledge and symptom recognition, poor glycemic or dyslipidemia control, greater difficulty interpreting food labels and estimating portion sizes, lower self-efficacy, higher level of body mass index, information gap in the use of medical devices for self-monitoring of blood glucose (SMBG), poorer communication with their providers, higher doses of insulin, more medical expenses and hospitalization among diabetes patients [50-57]. LHL is more common in people with hypertension and is associated with hypertension prevalence in selected ethnic groups [58]. Among hypertensive patients, LHL was associated with higher dietary salt intake, poor knowledge of blood pressure control, lower systolic blood pressure control, current smoking or higher nicotine dependence, as well as established predictors of smoking relapse [59-62]. Apart from these, LHL was associated with higher addiction severity [63], medication errors, misinterpreting physician’s instructions and disease symptoms [64], a greater number of unreconciled medications [65], reason behind the medication discrepancy [66], preventable adverse drug reactions [67], inequity of access to the benefits of prescription medication [68].
Substance use disorder
Drug addiction kills approximately 8 million people each year, and the UN Office on Drugs and Crime (UNODC)’s World Drug Report 2022 estimates that approximately 284 million people aged 15-64 used drugs worldwide in 2020 [69,70]. According to University of Pennsylvania research, America has spent over a trillion dollars enforcing its drug policy since 1971 [71]. People who use alcohol (AUD) or have a substance use disorder (SUD) are at risk of having lower health literacy due to a variety of negative health, psychosocial, and economic factors associated with substance use [72]. Another study confirms that both LHL and low academic performance have their role in tackling the disparities in substance use [73]. An Australian study with a mixed sample of people with AUD and SUD found that 90% of participants had LHL [74]. In people with alcohol and drug dependence, LHL is associated with worse depressive symptoms [63]. Patients with LHL poorly handle pain medications [75]. Around 300 metric tons of morphine-type painkillers are used (and/or abused) worldwide each year, more than 99% of which consumed by high income countries [76]. A study based on a mixed population of US citizens confirmed that LHL was strongly linked to opioid misuse among adult patients with chronic pain [77]. Use of cannabis for pain management has always been a controversial issue. Also, cannabis in the form of medical cannabis (MC) or recreational marijuana legalized or less restricted in Thailand, Canada, Uruguay, South Korea, Japan, India, Pakistan, Israel, Belgium, USA, UK, Germany, Italy, Singapore and Malaysia, probably among many others. However, Health literacy, social support, attitudes about MC, age, and duration of disease were significantly associated with demand for MC use among cancer patients in Thailand [78].
Poor COVID-19 or contagious disease management and vaccine negligence
A cross-sectional study of 259 school leaders in Hong Kong carried out during the COVID-19 pandemic between April 2021 and February 2022 shows that more than 50% of participants had LHL, and their LHL was strongly associated with a negative attitude about vaccination, low information, and confusion about COVID-19-related information [79]. However, an Oxford Academic study concluded that not health literacy directly but poor knowledge of selected diseases were associated with the vaccine confidence index [80]. Thankfully, another study from Oxford University Press established health literacy as the "social vaccine" to combat SARS-CoV-2 [81]. Even before Covid-19, WHO had listed vaccine hesitancy as one of the top ten global health threats in 2019 [82,83]. Also, a Swiss journal says that a percentage increase in vaccine hesitancy can lead to a decline in vaccination coverage by 30% [84]. Therefore, LHL was the major obstacle to creating vaccine hesitancy in China, Africa [85], India [86], Europe [87], and the USA [88,89]. As expected, in three different studies, close to 40% of Chinese participants (LHL persists among more than 70% of the population) [10,85], more than 60% of Bulgarians (the lowest health literacy among EU countries) [3,86] showed hesitancy, and above all, more than one-third of European adults are not fully vaccinated (LHL persists among half of the total population), says another Oxford University Press study [10,89]. Vaccinated people or people wearing masks, on the other hand, were careless about social distancing, believing that being vaccinated or wearing masks was sufficient and that other preventive measures, such as social distancing, were unnecessary. Even the CDC redeemed fully vaccinated people who wore a face mask or engaged in social distancing in most settings, whether outdoors or indoors, in updated public health guidance released on May 13, 2021. Also, conspiracy theories and rallies against masks/vaccines are vividly reported [90-97].
Barriers to Autism Recovery and Progression
The social burden of autism can exceed $6 trillion in the US alone by 2060, and the WHO estimated that worldwide, about one in 100 children has autism [98,99]. The failure to recognize the first signs of autism can significantly postpone the age of diagnosis, the provision of informed supervision to families, and the execution of adapted initiatives during the critical period of early development. Parent health literacy may further contribute to autism services use for young children [100]. A misunderstanding of early signs as manifestations of a developmental condition may lead to increased stigma and non-conventional explanations [101-103]. Parents with LHL whose child has recently been diagnosed with autism spectrum disorder (ASD) report an information gap and a lack of resource adaptation during diagnosis [104]. Above all, health literacy is linked to help-seeking behaviors among parents of children with special health care needs (CSHCN), autism, and attention deficit hyperactivity disorder (ADHD); or people with Schizophrenia and Bipolar disorders [105-107].
RESULTS AND DISCUSSION
LHL contributes significantly to the healthcare system's incompetent socioeconomic culture. Health issues are not only overlooked but also neglected. It reflects how much health and wellbeing are overlooked in a community or country. Economic conditions should not be condemned because they persist in developed countries as well. LHL has grown to unbearable proportions all over the world. Reading, listening, analytical, and decision-making skills, as well as the ability to apply them to health situations, are all components of health literacy. Literacy can only be improved through health education, which necessitates multifaceted approaches. Many members of the health care team lack health literacy training are unaware of ways to improve communication, and forget to use effective communication practices on a regular basis when providing care. Health care professionals require assistance and training to better understand health literacy and how to address it through clear communication strategies. Customized patient education, on the other hand, engages, motivates, and strengthens patients to participate in their own health care and treatment decisions, resulting in better outcomes, fewer diagnostic tests, and significantly greater patient satisfaction.
CONCLUSION
Nonetheless, health literacy is clearly beneficial in addressing the healthcare needs of even the most marginalized and disadvantaged communities. Patients must clearly and appropriately recognize healthcare information related to their specific illness or disease in order to improve adherence. This understanding could be crucial in assisting patients in developing the motivation, beliefs, and appropriate health behaviors needed to improve overall adherence. LHL is a curse to be avoided. This effort should be supported by all healthcare providers, stakeholders, and even government and community leaders.
ACKNOWLEDGEMENTS
Dr. Rayhan A. Tariq, Drexel University College of Medicine for taking the time to review my paper and for his insightful comments. For lending me books, journals, and newsletters, the seminar library of the University of Dhaka's Faculty of Pharmacy and Bangladesh's BANSDOC Library are also to be thanked.
DECLARATIONS
The current research was carried out exclusively to look into problems associated with low health literacy. With time and the availability of newer investigation in the same field, the statistical evidence or variables presented here may transform.
FUNDING
The author has not received any fund from any authority.
AUTHOR CONTRIBUTIONS
The corresponding author is the sole contributor and the only author.
CONFLICTS OF INTEREST
The author declares that he has no competing interests.
REFERENCES
- Mohiuddin AK. (2022). Medication adherence: Fact or fictions? Current Research in Public Health.2(1):18-21. DOI: 10.31586/crph.2022.533.
- Lovrić B, Placento H, Farčić N, Lipič Baligač M, Mikšić Š, Mamić M, et al. (2022). Association between Health Literacy and Prevalence of Obesity, Arterial Hypertension, and Diabetes Mellitus. Int J Environ Res Public Health. 19(15):9002. DOI: 10.3390/ijerph19159002.
- Gatulytė I, Verdiņa V, Vārpiņa Z, Lublóy Á. (2022). Level of health literacy in Latvia and Lithuania: a population-based study. Arch Public Health. 80(1):166. DOI: 10.1186/s13690-022-00886-3.
- Buawangpong N, Sirikul W, Anukhro C, Seesen M, La-Up A, Siviroj P. (2022). Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens. Int J Environ Res Public Health. 19(10):6051. DOI: 10.3390/ijerph19106051.
- van der Heide I, Wang J, Droomers M, Spreeuwenberg P, Rademakers J, Uiters E. (2013). The relationship between health, education, and health literacy: results from the Dutch Adult Literacy and Life Skills Survey. J Health Commun. 18(Suppl 1):172-184. DOI: 10.1080/10810730.2013.825668.
- Mohiuddin AK. (2020). Chapter 11. The Enigma of Patient Behavior. In The role of the pharmacist in patient care: Achieving high quality, cost-effective and accessible healthcare through a team-based, patient-centered approach. USA: Universal-Publishers. pp. 189-210. ISBN-10: 1627343083, ISBN-13: 9781627343084.
- US CDC. (2021). Health Literacy Basics-Talking points about health literacy. Centers for Disease Control and Prevention. Retrieved February 27, 2023. Available at: https://www.cdc.gov/healthliteracy/shareinteract/TellOthers.html.
- Shahid R, Shoker M, Chu LM, Frehlick R, Ward H, Pahwa P. (2022). Impact of low health literacy on patients' health outcomes: a multicenter cohort study. BMC Health Serv Res. 22(1):1148. DOI: 10.1186/s12913-022-08527-9.
- UCL Institute of Health Equity/Public Health England. (2015). Local action on health inequalities: Improving health literacy to reduce health inequalities-Practice resource summary. UK Government Publishing Service. Retrieved February 27, 2023. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/460710/4b_Health_Literacy-Briefing.pdf.
- Mohiuddin AK. (2022). Low Health Literacy: Treacherous Foe of Patient Compliance in Developed Countries. Annals of Epidemiology & Public Health. 5(2):1097. Retrieved February 27, 2023. Available at: https://meddocsonline.org/annals-of-epidemiology-and-public-health/low-health-literacy-treacherous-foe-of-patient-compliance-in-developed-countries.pdf.
- Li Y, Lv X, Liang J, Dong H, Chen C. (2022). The development and progress of health literacy in China. Front Public Health. 10:1034907. DOI: 10.3389/fpubh.2022.1034907.
- Rong H, Lu L, Wang L, Liu C, Zhang L, Li F, et al. (2023). Investigation of health literacy status and related influencing factors in military health providers of Chinese People's liberation Army, a cross-sectional study. BMC Public Health. 23(1):4. DOI: 10.1186/s12889-022-14958-0.
- Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et.al. (2018). High-quality health systems in the Sustainable Development Goals era: time for a revolution. Lancet Glob Health. 6(11):e1196-e1252. DOI: 10.1016/S2214-109X(18)30386-3.
- Tajdar D, Schäfer I, Lühmann D, Fertmann R, Steinberg T, van den Bussche H, et al. (2022). The Link Between Health Literacy and Three Conditions of Metabolic Syndrome: Obesity, Diabetes and Hypertension. Diabetes Metab Syndr Obes. 15:1639-1650. DOI: 10.2147/DMSO.S363823.
- Šulinskaitė K, Zagurskienė D, Blaževičienė A. (2022). Patients' health literacy and health behaviour assessment in primary health care: evidence from a cross-sectional survey. BMC Prim Care. 23(1):223. DOI: 10.1186/s12875-022-01809-5.
- Murugesu L, Heijmans M, Rademakers J, Fransen MP. (2022). Challenges and solutions in communication with patients with low health literacy: Perspectives of healthcare providers. PLoS One. 17(5):e0267782. DOI: 10.1371/journal.pone.0267782.
- Weerakoon SM, Henson-Garcia M, Valerio-Shewmaker MA, Messiah SE, Knell G. (2022). Contributions of Trustworthiness, Health Literacy, and Self-Efficacy in Communicating With COVID-19 Vaccine-Hesitant Audiences: Web-Based Survey Study. JMIR Form Res. 6(8):e38076. DOI: 10.2196/38076.
- Shebehe J, Montgomery S, Hansson A, Hiyoshi A. (2022). Low health literacy and multiple medications in community-dwelling older adults: a population-based cohort study. BMJ Open. 12(2):e055117. DOI: 10.1136/bmjopen-2021-055117.
- Cheng BT, Tanna AP. (2023). Association of Health Literacy and Health Care Utilization Among Glaucoma Patients. J Glaucoma. 32(2):139-144. DOI: 10.1097/IJG.0000000000002133.
- Abdullah A, Liew SM, Salim H, Ng CJ, Chinna K. (2019). Prevalence of limited health literacy among patients with type 2 diabetes mellitus: A systematic review. PLoS One. 14(5):e0216402. DOI: 10.1371/journal.pone.0216402.
- Meldgaard M, Gamborg M, Terkildsen Maindal H. (2022). Health literacy levels among women in the prenatal period: A systematic review. Sex Reprod Healthc. 34:100796. DOI: 10.1016/j.srhc.2022.100796.
- Rolova G, Gavurova B, Petruzelka B. (2020). Exploring Health Literacy in Individuals with Alcohol Addiction: A Mixed Methods Clinical Study. Int J Environ Res Public Health. 17(18):6728. DOI: 10.3390/ijerph17186728.
- Griffey RT, Kennedy SK, D'Agostino McGowan L, Goodman M, Kaphingst KA. (2014). Is low health literacy associated with increased emergency department utilization and recidivism? Acad Emerg Med. 21(10):1109-1115. DOI: 10.1111/acem.12476.
- Zaidman EA, Scott KM, Hahn D, Bennett P, Caldwell PH. (2023). Impact of parental health literacy on the health outcomes of children with chronic disease globally: A systematic review. J Paediatr Child Health. 59(1):12-31. DOI: 10.1111/jpc.16297.
- Hickey KT, Masterson Creber RM, Reading M, Sciacca RR, Riga TC, Frulla AP, et al. (2018). Low health literacy: Implications for managing cardiac patients in practice. Nurse Pract. 43(8):49-55. DOI: 10.1097/01.NPR.0000541468.54290.49.
- Lorini C, Buscemi P, Mossello E, Schirripa A, Giammarco B, Rigon L, et al. (2023). Health literacy of informal caregivers of older adults with dementia: results from a cross-sectional study conducted in Florence (Italy). Aging Clin Exp Res. 35(1):61-71. DOI: 10.1007/s40520-022-02271-0.
- Gan W, Zhang Q, Yang D, Yin J, Wang Y, Song L, et al. (2022). A behavior change wheel-based interactive pictorial health education program for hypertensive patients with low blood pressure health literacy: study protocol for a randomized controlled trial. Trials. 23(1):369. DOI: 10.1186/s13063-022-06300-1.
- Kanejima Y, Shimogai T, Kitamura M, Ishihara K, Izawa KP. (2022). Impact of health literacy in patients with cardiovascular diseases: A systematic review and meta-analysis. Patient Educ Couns. 105(7):1793-1800. DOI: 10.1016/j.pec.2021.11.021.
- Achstetter K, Köppen J, Haltaufderheide M, Hengel P, Blümel M, Busse R. (2022). Health Literacy of People with Substitutive Private Health Insurance in Germany and Their Assessment of the Health System Performance According to Health Literacy Levels: Results from a Survey. Int J Environ Res Public Health. 19(24):16711. DOI: 10.3390/ijerph192416711.
- Bosle C, Orth B, Reibling N, Merkel C, Muschalik C, von Rüden U. (2022). Health information behaviour and health literacy on COVID-19 vaccination of the general population in Germany-findings from the CoSiD study. Federal Health-Gazette Health-Research-Health Protection (Springer). 65(12):1289-1298. DOI: 10.1007/s00103-022-03617-9.
- O'Mara CS, Young JP, Winkelmann ZK. (2022). Financial Health Literacy and the Shared Decision-Making Process in Healthcare. Int J Environ Res Public Health. 19(11):6510. DOI: 10.3390/ijerph19116510.
- Lossius MI, Alfstad KÅ, Aaberg KM, Nakken KO. (2017). Discontinuation of antiepileptic drugs in seizure-free patients-when and how? Tidsskr Nor Laegeforen. 137(6):451-454. DOI: 10.4045/tidsskr.16.0957.
- Caqueo-Urízar A, Urzúa A, Mena-Chamorro P, Bravo de la Fuente J. (2021). Effects of Adherence to Pharmacological Treatment on the Recovery of Patients with Schizophrenia. Healthcare (Basel). 9(9):1230. DOI: 10.3390/healthcare9091230.
- Banerjee S, Varma RP. (2013). Factors Affecting Non-Adherence among Patients Diagnosed with Unipolar Depression in a Psychiatric Department of a Tertiary Hospital in Kolkata, India. Depress Res Treat. 2013:809542. DOI: 10.1155/2013/809542.
- Graeupner D, Coman A. (2017). The dark side of meaning-making: How social exclusion leads to superstitious thinking. Journal of Experimental Social Psychology. 69:218-222. DOI: 10.1016/j.jesp.2016.10.003.
- Puckree T, Mkhize M, Mgobhozi Z, Lin J. (2002). African traditional healers: what health care professionals need to know. Int J Rehabil Res. 25(4):247-251. DOI: 10.1097/00004356-200212000-00001.
- Taher M, Pashaeypoor S, Cheraghi MA, Karimy M, Hoseini ASS. (2020). Superstition in health beliefs: Concept exploration and development. J Family Med Prim Care. 9(3):1325-1330. DOI: 10.4103/jfmpc.jfmpc_871_19.
- Grim BJ, Grim ME. (2019). Belief, Behavior, and Belonging: How Faith is Indispensable in Preventing and Recovering from Substance Abuse. J Relig Health. 58(5):1713-1750. DOI: 10.1007/s10943-019-00876-w.
- Mirahmadizadeh A, Delam H, Seif M, Banihashemi SA, Tabatabaee H. (2019). Factors Affecting Insulin Compliance in Patients with Type 2 Diabetes in South Iran, 2017: We Are Faced with Insulin Phobia. Iran J Med Sci. 44(3):204-213.
- Anbesu EW, Asgedom DK. (2023). Menstrual hygiene practice and associated factors among adolescent girls in sub-Saharan Africa: a systematic review and meta-analysis. BMC Public Health. 23(1):33. DOI: 10.1186/s12889-022-14942-8.
- Garg S, Anand T. (2015). Menstruation related myths in India: strategies for combating it. J Family Med Prim Care. 4(2):184-186. DOI: 10.4103/2249-4863.154627.
- Gopalan M. (2019). Less than 20% menstruating girls & women in India use pads. Here's how to overcome barriers. The Print is retrieved February 27, 2023. Available at: https://theprint.in/health/less-than-20-per-cent-menstruating-girls-women-in-india-use-pads/317570/.
- Web Desk. (2017). Can a campaign to remove tax on sanitary pads help Indian women adopt better hygiene? Zee Business. Retrieved February 27, 2023. Available at: https://www.zeebiz.com/india/news-can-a-campaign-to-remove-tax-on-sanitary-pads-help-women-adopt-better-hygiene-15513.
- Patwa J, Pandit N. (2018). Open Defecation-Free India by 2019: How Villages are Progressing? Indian J Community Med. 43(3):246-247. DOI: 10.4103/ijcm.IJCM_83_18.
- Belay DG, Asratie MH, Aragaw FM, Tsega NT, Endalew M, Gashaw M. (2022). Open defecation practice and its determinants among households in sub-Saharan Africa: pooled prevalence and multilevel analysis of 33 sub-Saharan Africa countries demographic and health survey. Trop Med Health. 50(1):28. DOI: 10.1186/s41182-022-00416-5.
- Upadhyay A. (2019). From a luxury to suffocating, here are some unusual myths regarding toilets debunked. NDTV. Retrieved February 27, 2023. Available at: https://swachhindia.ndtv.com/toilets-myth-debunked-swachh-india-33462/.
- Cuthino FL, Sheilini M, Chandrababu R. (2021). The comparison of health literacy between health science and non-health Science members-a cross sectional study of multifaceted Public Health Affair. Clinical Epidemiology and Global Health. 12:100893. DOI: 10.1016/j.cegh.2021.100893.
- Mohiuddin AK. (2022). Medication adherence: Fact or fictions? Current Research in Public Health. 2(1):18-21. DOI: 10.31586/crph.2022.533.
- Fan JH, Lyons SA, Goodman MS, Blanchard MS, Kaphingst KA. (2016). Relationship Between Health Literacy and Unintentional and Intentional Medication Nonadherence in Medically Underserved Patients With Type 2 Diabetes. Diabetes Educ. 42(2):199-208. DOI: 10.1177/0145721715624969.
- ALSharit BA, Alhalal EA. (2022). Effects of health literacy on type 2 diabetic patients' glycemic control, self-management, and quality of life. Saudi Med J. 43(5):465-472. DOI: 10.15537/smj.2022.43.5.20210917.
- Tefera YG, Gebresillassie BM, Emiru YK, Yilma R, Hafiz F, Akalu H, Ayele AA. (2020). Diabetic health literacy and its association with glycemic control among adult patients with type 2 diabetes mellitus attending the outpatient clinic of a university hospital in Ethiopia. PLoS One. 15(4):e0231291. DOI: 10.1371/journal.pone.0231291.
- Ziapour A, Ebadi Fard Azar F, Mahaki B, Mansourian M. (2022). Factors affecting the health literacy status of patients with type 2 diabetes through demographic variables: A cross-sectional study. J Educ Health Promot. 11:306. DOI: 10.4103/jehp.jehp_1759_21.
- Mogessie HM, Gebeyehu MA, Kenbaw MG, Tadesse TA. (2022). Diabetic health literacy and associated factors among diabetes mellitus patients on follow up at public hospitals, Bale Zone, South East Ethiopia, 2021. PLoS One. 17(7):e0270161. DOI: 10.1371/journal.pone.0270161.
- Chiou SJ, Chang YJ, Liao K, Chen CD. (2022). Modest association between health literacy and risk for peripheral vascular disease in patients with type 2 diabetes. Front Public Health. 10:946889. DOI: 10.3389/fpubh.2022.946889.
- White RO, Wolff K, Cavanaugh KL, Rothman R. (2010). Addressing Health Literacy and Numeracy to Improve Diabetes Education and Care. Diabetes Spectr. 23(4):238-243. DOI: 10.2337/diaspect.23.4.238.
- Osborn CY, Cavanaugh K, Wallston KA, Rothman RL. (2010). Self-efficacy links health literacy and numeracy to glycemic control. J Health Commun. 15(Suppl 2):146-58. DOI: 10.1080/10810730.2010.499980.
- Brockmeyer M, Wies E, Joerges J, Sommer J, Borgmann SO, Chernyak N, et al. (2023). Knowledge of HbA1c and LDL-C treatment goals, subjective level of disease-related information and information needs in patients with atherosclerotic cardiovascular disease. Clin Cardiol. 46(2):223-231. DOI: 10.1002/clc.23948.
- Miranda R, Meeks KAC, Snijder MB, van den Born BJ, Fransen MP, Peters RJ, et al. (2020). Health literacy and hypertension outcomes in a multi-ethnic population: the HELIUS study. Eur J Public Health. 30(3):545-550. DOI: 10.1093/eurpub/ckz174.
- Mohd Isa D, Shahar S, He FJ, Majid HA. (2021). Associations of Health Literacy with Blood Pressure and Dietary Salt Intake among Adults: A Systematic Review. Nutrients. 13(12):4534. DOI: 10.3390/nu13124534.
- Du S, Zhou Y, Fu C, Wang Y, Du X, Xie R. (2018). Health literacy and health outcomes in hypertension: An integrative review. Int J Nurs Sci. 5(3):301-309. DOI: 10.1016/j.ijnss.2018.06.001.
- Halladay JR, Donahue KE, Cené CW, Li Q, Cummings DM, Hinderliter AL, et al. (2017). The association of health literacy and blood pressure reduction in a cohort of patients with hypertension: The heart healthy lenoir trial. Patient Educ Couns. 100(3):542-549. DOI: 10.1016/j.pec.2016.10.015.
- Hoover DS, Vidrine JI, Shete S, Spears CA, Cano MA, Correa-Fernández V, et al. (2015). Health Literacy, Smoking, and Health Indicators in African American Adults. J Health Commun. 20 Suppl 2(02):24-33. DOI: 10.1080/10810730.2015.1066465.
- Lincoln A, Paasche-Orlow MK, Cheng DM, Lloyd-Travaglini C, Caruso C, Saitz R, et al. (2006). Impact of health literacy on depressive symptoms and mental health-related: quality of life among adults with addiction. J Gen Intern Med. 21(8):818-822. DOI: 10.1111/j.1525-1497.2006.00533.x.
- Rahman FI, Aziz F, Huque S, Ether SA. (2020). Medication understanding and health literacy among patients with multiple chronic conditions: A study conducted in Bangladesh. J Public Health Res. 9(1):1792. DOI: 10.4081/jphr.2020.1792.
- Persell SD, Osborn CY, Richard R, Skripkauskas S, Wolf MS. (2007). Limited health literacy is a barrier to medication reconciliation in ambulatory care. J Gen Intern Med. 22(11):1523-1526. DOI: 10.1007/s11606-007-0334-x.
- Lindquist LA, Go L, Fleisher J, Jain N, Friesema E, Baker DW. (2012). Relationship of health literacy to intentional and unintentional non-adherence of hospital discharge medications. J Gen Intern Med. 27(2):173-178. DOI: 10.1007/s11606-011-1886-3.
- Kim M, Suh D, Barone JA, Jung SY, Wu W, Suh DC. (2022). Health Literacy Level and Comprehension of Prescription and Nonprescription Drug Information. Int J Environ Res Public Health. 19(11):6665. DOI: 10.3390/ijerph19116665.
- Protheroe J, Nutbeam D, Rowlands G. (2009). Health literacy: a necessity for increasing participation in health care. Br J Gen Pract. 59(567):721-723. DOI: 10.3399/bjgp09X472584.
- Dalal PK. (2020). Changing scenario of addiction psychiatry: Challenges and opportunities. Indian J Psychiatry. 62(3):235-241. DOI:10.4103/psychiatry.IndianJPsychiatry_346_20.
- UN. (2022). UNODC World Drug Report 2022 highlights trends on cannabis post-legalization, environmental impacts of illicit drugs, and drug use among women and Youth. United Nations: Office on Drugs and Crime. Available at: https://www.unodc.org/unodc/frontpage/2022/June/unodc-world-drug-report-2022-highlights-trends-on-cannabis-post-legalization--environmental-impacts-of-illicit-drugs--and-drug-use-among-women-and-youth.html.
- Lee J. (2021). America has spent over a trillion dollars fighting the war on drugs. 50 years later, drug use in the U.S. is climbing again. CNBC. Available at: https://www.cnbc.com/2021/06/17/the-us-has-spent-over-a-trillion-dollars-fighting-war-on-drugs.html.
- Rolova G, Gavurova B, Petruzelka B. (2021). Health Literacy, Self-Perceived Health, and Substance Use Behavior among Young People with Alcohol and Substance Use Disorders. Int J Environ Res Public Health. 18(8):4337. DOI: 10.3390/ijerph18084337.
- Kinnunen JM, Paakkari L, Rimpelä AH, Kulmala M, Richter M, Kuipers MAG, et al. (2022). The role of health literacy in the association between academic performance and substance use. Eur J Public Health. 32(2):182-187. DOI: 10.1093/eurpub/ckab213.
- Degan TJ, Kelly PJ, Robinson LD, Deane FP. (2019). Health literacy in substance use disorder treatment: A latent profile analysis. J Subst Abuse Treat. 96:46-52. DOI: 10.1016/j.jsat.2018.10.009.
- Devraj R, Herndon CM, Griffin J. (2013). Pain awareness and medication knowledge: a health literacy evaluation. J Pain Palliat Care Pharmacother. 27(1):19-27. DOI: 10.3109/15360288.2012.751955.
- Mohiuddin AK. (2022). Rational use of medications: Eccentric or non-existent? Mathews Journal of Pharmaceutical Science. 6(1):1-4. DOI: 10.30654/mjps.10009.
- Rogers AH, Bakhshaie J, Orr MF, Ditre JW, Zvolensky MJ. (2020). Health Literacy, Opioid Misuse, and Pain Experience Among Adults with Chronic Pain. Pain Med. 21(4):670-676. DOI: 10.1093/pm/pnz062.
- Sukrueangkul A, Panomai N, Laohasiriwong W, Sakphisutthikul C, Phimha S. (2022). Factors Influencing Demand for Medical Cannabis Use among Cancer Patients in the North of Thailand. Asian Pac J Cancer Prev. 23(1):319-325. DOI: 10.31557/APJCP.2022.23.1.319.
- Lau SSS, Shum ENY, Man JOT, Cheung ETH, Amoah PA, Leung AYM, et al. (2022). COVID-19-Related Health Literacy of School Leaders in Hong Kong: A Cross-Sectional Study. Int J Environ Res Public Health. 19(19):12790. DOI: 10.3390/ijerph191912790.
- Casigliani V, Arzilli G, Menicagli D, Scardina G, Lopalco PL. (2020). Vaccine hesitancy and health literacy: We need to change our paradigm. European Journal of Public Health. 30(Supplement_5). DOI: 10.1093/eurpub/ckaa165.032.
- Okan O, Messer M, Levin-Zamir D, Paakkari L, Sørensen K. (2022). Health literacy as a social vaccine in the COVID-19 pandemic. Health Promot Int. daab197. DOI: 10.1093/heapro/daab197.
- Singh P, Dhalaria P, Kashyap S, Soni GK, Nandi P, Ghosh S, et al. (2022). Strategies to overcome vaccine hesitancy: a systematic review. Syst Rev. 11(1):78. DOI: 10.1186/s13643-022-01941-4.
- Lazarus JV, Wyka K, White TM, Picchio CA, Rabin K, Ratzan SC, et al. (2022). Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat Commun. 13(1):3801. DOI: 10.1038/s41467-022-31441-x.
- Dhalaria P, Arora H, Singh AK, Mathur M, S AK. (2022). COVID-19 Vaccine Hesitancy and Vaccination Coverage in India: An Exploratory Analysis. Vaccines (Basel). 10(5):739. DOI: 10.3390/vaccines10050739.
- Zhang H, Li Y, Peng S, Jiang Y, Jin H, Zhang F. (2022). The effect of health literacy on COVID-19 vaccine hesitancy among community population in China: The moderating role of stress. Vaccine. 40(32):4473-4478. DOI: 10.1016/j.vaccine.2022.06.015.
- Steinert JI, Sternberg H, Prince H, Fasolo B, Galizzi MM, Büthe T, et al. (2022). COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci Adv. 8(17):eabm9825. DOI: 10.1126/sciadv.abm9825.
- Nguyen QC, Yardi I, Gutierrez FXM, Mane H, Yue X. (2022). Leveraging 13 million responses to the U.S. COVID-19 Trends and Impact Survey to examine vaccine hesitancy, vaccination, and mask wearing, January 2021-February 2022. BMC Public Health. 22(1):1911. DOI: 10.1186/s12889-022-14286-3.
- Becerra MB, Becerra BJ. (2022). COVID-19 Vaccine Hesitancy among Behavioral Risk Takers. Vaccines (Basel). 10(5):767. DOI: 10.3390/vaccines10050767.
- Kouvari K, Hadjikou A, Heraclidou I, Heraclides A. (2022). Health Literacy, consciousness, and locus of control in relation to vaccine hesitancy and refusal. European Journal of Public Health. 32(Supplement_3). DOI: 10.1093/eurpub/ckac129.640.
- Lin C, Tu P, Beitsch LM. (2020). Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines (Basel). 9(1):16. DOI: 10.3390/vaccines9010016.
- Khanna M. (2020). Face masks make people more careless with social distancing reveals study. India Times. Available at: https://www.indiatimes.com/technology/science-and-future/face-mask-social-distancing-study-521226.html.
- Mohiuddin AK. (2020). Covid-19 and 20 resolutions for Bangladesh. European Journal of Sustainable Development Research. 4(4). DOI: 10.29333/ejosdr/8433.
- Esmaeilzadeh P. (2022). Public concerns and burdens associated with face mask-wearing: Lessons learned from the COVID-19 pandemic. Prog Disaster Sci. 13:100215. DOI: 10.1016/j.pdisas.2022.100215.
- Lovelace B. (2021). CDC says fully vaccinated people don't need to wear face masks indoors or outdoors in most settings. CNBC. Available at: https://www.cnbc.com/2021/05/13/cdc-says-fully-vaccinated-people-dont-need-to-wear-face-masks-indoors-or-outdoors-in-most-settings.html.
- Taylor S, Asmundson GJG. (2021). Negative attitudes about facemasks during the COVID-19 pandemic: The dual importance of perceived ineffectiveness and psychological reactance. PloS One. 16(2):e0246317. DOI: 10.1371/journal.pone.0246317.
- Lewandowsky S, Holford D, Schmid P. (2022). Public policy and conspiracies: The case of mandates. Curr Opin Psychol. 47:101427. DOI: 10.1016/j.copsyc.2022.101427.
- Ray E. (2022. Truckers protesting Covid mandates are amassing outside the capital. The New York Times. Available at: https://www.nytimes.com/live/2022/03/05/world/covid-19-tests-cases-vaccine.
- Blaxill M, Rogers T, Nevison C. (2022). Autism Tsunami: the Impact of Rising Prevalence on the Societal Cost of Autism in the United States. J Autism Dev Disord. 52(6):2627-2643. DOI: 10.1007/s10803-021-05120-7.
- WHO. (2022). Autism. World Health Organization. Available at: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders.
- Lindly OJ, Cabral J, Mohammed R, Garber I, Mistry KB, Kuhlthau KA. (2022). I Don't Do Much Without Researching Things Myself": A Mixed Methods Study Exploring the Role of Parent Health Literacy in Autism Services Use for Young Children. J Autism Dev Disord. 52(8):3598-3611. DOI: 10.1007/s10803-021-05240-0.
- Ozonoff S, Young GS, Steinfeld MB, Hill MM, Cook I, Hutman T, et al. (2009). How early do parent concerns predict later autism diagnosis? J Dev Behav Pediatr. 30(5):367-75. DOI: 10.1097/dbp.0b013e3181ba0fcf.
- Buffle P, Gentaz E, Vivanti G. (2022). Perception, Beliefs, and Causal Attribution of Autism Early Signs in Ecuadorian General Population. Front Psychol. 13:915817. DOI: 10.3389/fpsyg.2022.915817.
- Chen YH, Chen Q, Kong L, Liu G. (2022). Early detection of autism spectrum disorder in young children with machine learning using medical claims data. BMJ Health Care Inform. 29(1):e100544. DOI: 10.1136/bmjhci-2022-100544.
- Valderrama A, Courcy I, Weis-Heitner L, Forgeot d'Arc B. (2020). Les enjeux de littératie dans la communication aux parents du diagnostic de trouble du spectre de l’autisme chez l’enfant [Health Literacy Issues of Parents Seeking Information on Autism Spectrum Disorder Around Time of Diagnosis]. Sante Ment Que. 45(1):127-145.
- Vovou F, Hull L, Petrides KV. (2021). Mental health literacy of ADHD, autism, schizophrenia, and bipolar disorder: a cross-cultural investigation. J Ment Health. 30(4):470-480. DOI: 10.1080/09638237.2020.1713999.
- Tm H, S Q, A G, Lj H, Gp B, P S, M K. (2023). Developmental disorders among Norwegian-born children with immigrant parents. Child Adolesc Psychiatry Ment Health. 17(1):3. DOI: 10.1186/s13034-022-00547-x.
- Keim-Malpass J, Letzkus LC, Kennedy C. (2015). Parent/caregiver health literacy among children with special health care needs: a systematic review of the literature. BMC Pediatr. 15:92. DOI: 10.1186/s12887-015-0412-x.