Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
First Report of M-My Mind Study
Humberto Martínez-Cordero1,2,3,*, Luis Antonio Salazar2, Jair Figueroa2, Maria Isabel Arbeláez2, Alejandro Rico Mendoza3,4, Alexandra Porras Ramírez3,4,5, Henry Idrobo2, Viviana Olaya2, Kenny Gálvez2, Sergio Cancelado2, Juan Manuel Herrera2, Leonardo Bautista Toloza2, Jessica Zapata Malagón3, Lorena Cubillos Osorio3, Isabella Novoa-Caicedo3, On Behalf of GRIMMCO (Colombian Multiple Myeloma Research Group) and GRHEMUB (El Bosque University Hematology Group)
1Princess Margaret Cancer Centre UHN, University of Toronto, Toronto, Canada
2Colombian Multiple Myeloma Research Group, Colombia
3El Bosque University Hematology Group, Colombia
4Community Medicine and Collective Health Group, El Bosque University, Colombia
5Coordination of Epidemiology and Research, Los Cobos Medical Center, Colombia
*Corresponding author: Dr. Humberto Martínez-Cordero, MD MSc, Hematology Clinical and Research Fellowship in Multiple Myeloma, Princess Margaret Cancer Center, University of Toronto, Canada; E-mails: [email protected], [email protected].
Received Date: March 15, 2023
Published Date: April 25, 2023
Citation: Martínez-Cordero H, et al. (2023). First Report of M-My Mind Study. Mathews J Cancer Sci. 8(2):41.
Copyrights: Martínez-Cordero H, et al. © (2023).
ABSTRACT
Multiple myeloma (MM) is a heterogeneous and incurable disease considered the second most common hematologic malignancy globally. The incidence, prevalence, and mortality worldwide are well-known thanks to the data reported by the International Agency for Research on Cancer (IARC) and by the Global Cancer Observatory GLOBOCAN. Our objective was to estimate the incidence, prevalence, and mortality of MM in Colombia in this work. The total population diagnosed with multiple myeloma (ICD Code 10 C900) during the 2008-2018 period was used, which was included in the RIPS (Registro Individual de Prestación de Servicios) in Colombia.
The standardized incidence and prevalence rates for Colombia in 2018 were 1.79 (CI 1.76-1.81) and 8.97 x 100,000 inhabitants/year (CI8.94-8.99), respectively. The age-standardized mortality rate for Colombia was 1.39 x 100,000 inhabitants (1.36-1.41) (adjusted with the population of the United States). The prevalence was higher than that reported by other sources and is comparable with those of the whole world, North America, and Spain. MM must be one of the cancers in which epidemiology must prioritize and organize health cancer care due to the ageing population.
Keywords: Multiple Myeloma, Colombia, Incidence, Prevalence, Epidemology.
AIM
This is the first report of the MiMENTe study that shows the incidence, prevalence, and mortality of patients with 10-year-old multiple myeloma in Colombia. The prevalence of the disease is higher than that reported by international registries.
ABBREVIATIONS
DANE: National Department of Statistics (Departamento Administrativo Nacional de Estadística); GLOBOCAN: Global Cancer Observatory; IARC: Agency for Research on Cancer; MM: Multiple Myeloma; M-My Mind Study / MiMENTE: Multiple Myeloma, National and Territorial Epidemiology (Mieloma Múltiple, Epidemiología Nacional y Territorial); MGUS: Monoclonal Gammopathy of Undetermined Significance; RIPS: Individual Health Services Provision Records (Registro Individual de Prestación de Servicios); SEER: Surveillance, Epidemiology, and End Results; SMM: Smouldering Multiple Myeloma; SISPRO: Integrated Social Protection Information System (Sistema Integrado de Información de la Protección Social).
INTRODUCTION
Multiple myeloma (MM) is the second most frequent hematological malignancy, accounting for ∼1% of neoplastic diseases and 13% of hematologic cancers [1-3]. Nowadays is considered an incurable disease that progresses from a premalignant stage called monoclonal gammopathy of undetermined significance (MGUS) and a transitional stage named smouldering multiple myeloma (SMM) [3,4].
The worldwide incidence, prevalence, and mortality are well-known thanks to data reported by the International Agency for Research on Cancer (IARC), and by the GLOBOCAN World Cancer Observatory showing how over the last ten years, MM has caused an increasing number of deaths worldwide, however, the information on the epidemiology and disease burden of MM is limited, especially in the developing countries [5].
First-world countries have been reported to have much higher MM incidence and prevalence than first-world countries. Three high-incidence areas around the world are North America, Australia, and Western Europe, with incidences ranging from 3 to 6 per 100,000 inhabitants-years and the 5-year prevalence ranging from 7 to 14 per 100,000 population [3,6-8].
The data provided by Colombia to these reports come from the population cancer registries corresponding to 5 cities whose most up-to-date data are from 2020 [3,9,10]. National data can also be found in the base of the high-cost account [11]. Although there are indeed excellent sources of information, it is believed that there is a significant underreporting of the prevalence of the disease, which makes it necessary to optimize the information to achieve the establishment of programs oriented to work on better control of this type of hematological cancer [3,10,12]. The study M My Mind/MiMENTe (Mieloma Múltiple Epidemiología Nacional y territorial) is a collaborative effort to know the reality of the disease in terms of incidence, prevalence, and mortality in Colombia as a first step to control the disease even in the premalignant stages for the future wanting to position itself as a model for the control of MM in developing countries [3].
METHODS
MiMENTE (Mieloma Múltiple, Epidemiología Nacional y Territorial) is a multiphase study going through its first stage through a cross-sectional study in Colombia. The total population diagnosed with Multiple Myeloma (ICD Code 10 C900) during the 2008-2018 periods was included in the RIPS Individual Service Delivery Registry in Colombia. A comparison was made with the available data from GLOBOCAN (Global Cancer Observatory) and High-Cost Account. Records that had an unidentified diagnosis were excluded.
For this phase, a comparison is made of the data from the registries of the three entities described. Three frequency measures are established: Incidence, prevalence, and mortality, standardizing the latter using a direct method, making the Colombian population comparable with large countries such as the United States and Spain cataloged as countries of reference in the management and diagnosis of Multiple Myeloma. Variables such as ethnicity, age, place of origin, health regime, place of death will be studied in the future in later phases of the study [3].
MATERIALS AND METHODS
Study Population
During the years 2008 to 2018, the data were extracted from official databases for the Republic of Colombia using the ICD10: C900 codes. These data are present in the SISPRO (Sistema Integrado de Información de la Protección Social), which houses timely, sufficient, and standardized information for decision making in the health sector, centered on the citizen. It is made up of databases and information systems of the sector on supply and demand of health services, quality of services, insurance, financing, and social promotion. The information is collected through the RIPS (Individual Health Services Provision Records), defined as the set of minimum and basic data required by the General Health Social Security System for the management, regulation, and control processes. Patients who presented MM before January 1, 2009 were not taken [3,13].
Statistical Analysis
To obtain the prevalence and incidence of MM globally for Colombia, information was obtained from the RIPS through the SISPRO system as mentioned above. With the use of the ICD 10: sex, age group, and department of origin extracted C900 codes, information. Colombia has 32 departments with a total population of 48, 258,494 inhabitants. These figures are from official sources emanated by the National Department of Statistics (DANE) through the population and housing census conducted in 2018, which characterized and counted the people residing in Colombia. Its calculation was performed with the population with MM during the study period [3,13].
RESULTS
Between 2009 and 2018 (10 years), 26,356 MM diagnoses were found throughout the national territory of Colombia. The departments where there was the largest casuistry of patients with the diagnosis of MM were Cundinamarca, Valle del Cauca, Antioquia, Santander, Bolívar, and Atlántico Figure 1.
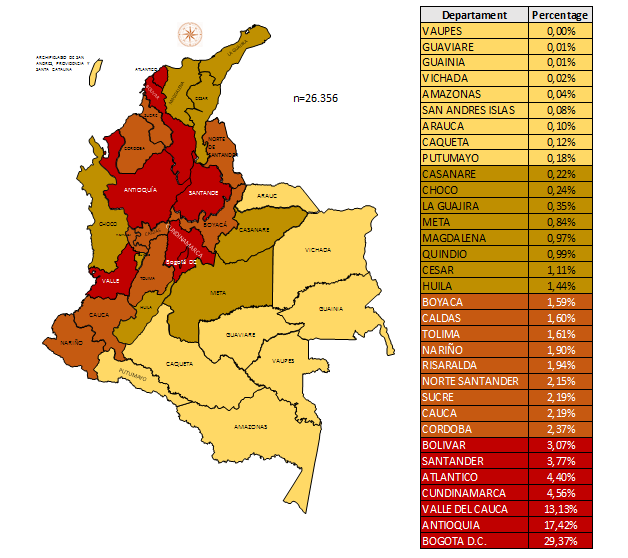
Figure 1. Total patients with Multiple Myeloma diagnosis attended in Colombia per department.
The most up-to-date data from IARC and GLOBOCAN correspond to the year 2018. A comparison was made of our data with those reported in this last registry for Colombia in addition to the high-cost account. Comparative data were developed with the population of the United States, standardizing this population, and it was also compared with the data reported for Spain. The prevalence of the disease is higher in Colombia than reported by GLOBOCAN, IARC and High-cost drug account Table 1.
Table 1. Comparison of Colombian MM incidence, prevalence and mortality x 100.000 inhabitants in 2018 with other reference population for the same year.
|
Variable |
RIPS data Colombia |
GLOBOCAN Colombia |
High cost drugs registry Colombia |
World wide |
E.E.U.U. |
Spain |
|
Incidence |
1.79 |
2.3 |
- |
1.7 |
4.1 |
2.8 |
|
Prevalence |
8.97 |
5.1 |
5.88 |
4.9 |
11.3 |
7.3 |
|
Age standardized Mortality |
1.39 |
1.4 |
- |
1.1 |
1.8 |
1.4 |
The standardized incidence for Colombia in 2018 was 1.79 (CI 1.76-1.81) inhabitants-year, and the prevalence was 8.97 (CI 8.94-8.99). The number of prevalent cases per year varied from 1138 in 2009 to 4474 cases in 2018—Figure 2.
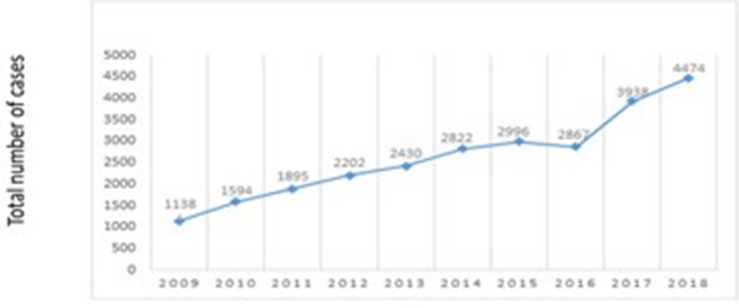
Figure 2. Total number of prevalent cases of MM per year in Colombia between 2009-2018.
When the prevalence is analyzed by region, it is higher in the Andean region Figure 3.
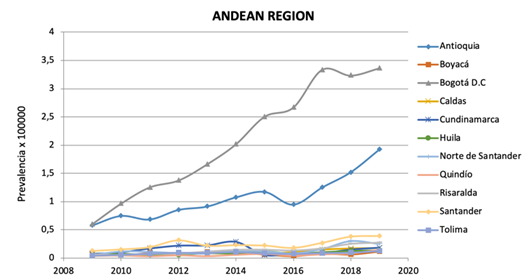
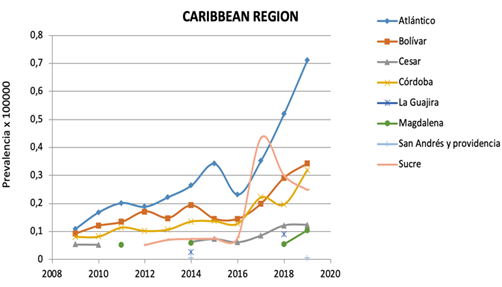
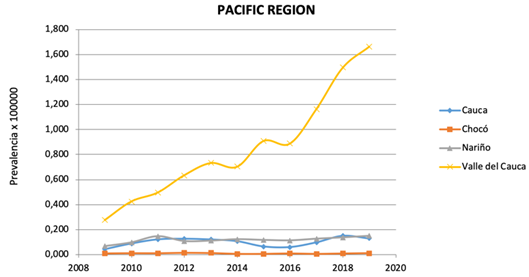
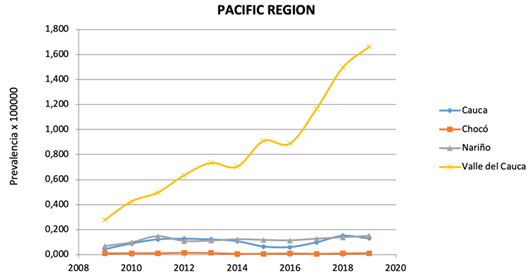
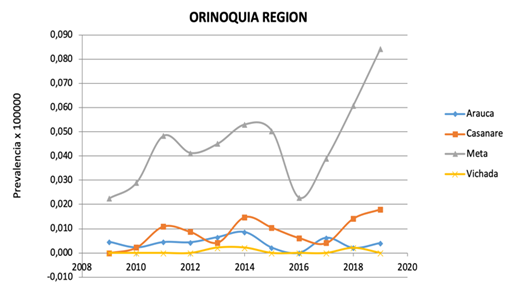
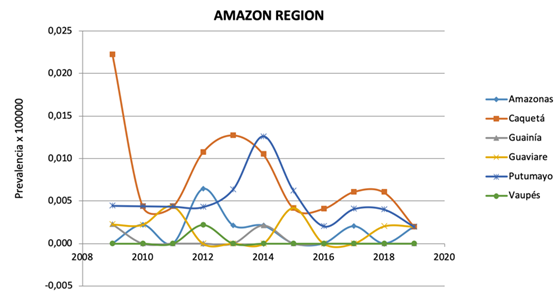
Figure 3. Adjusted prevalence of MM by regions in Colombia.
Mortality
During this entire period, 5481 deaths were found, 20.80%—Figure 4. The age-standardized mortality rate for Colombia is 1,39x100,000 inhabitants/year (CI 1.36-1.41) (Adjusted with the population of the United States).
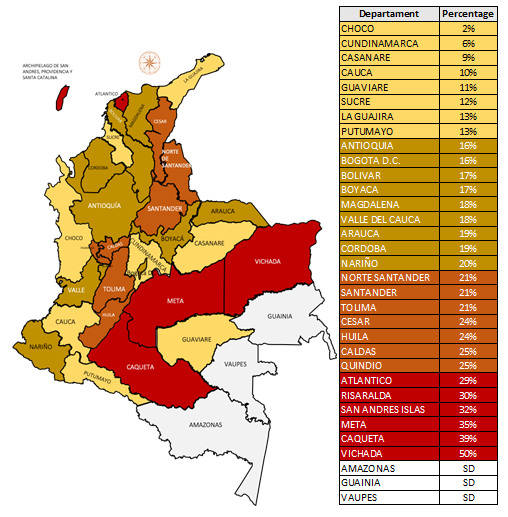
Figure 4. Total deaths in Multiple Myeloma diagnosis patients per departamento in Colombia per between 2009 to 2018.
DISCUSSION
Information from the US Surveillance, Epidemiology, and End Results (SEER) registry estimate 32,000 new cases of MM and 13,000 deaths from MM annually in the US. This is associated with an annual incidence of roughly 7 per 100,000 men and women per year [14].
Similar data has been shown by other sources like GLOBOCAN, primarily based in population-based registries [15-17].
In this national study, we illustrate three main conclusions about the epidemiology of MM in Colombia.
First, in 2018, the estimated prevalence was higher than those reported by GLOBOCAN and high-cost account [7,11]. The incidence was comparable but lower than the one reported from United States of America, and it seems that the mortality is also comparable [7]. Of note, one study regarding Latin American MM epidemiology showed an incidence of 4.2 and 12.8 per 100,000 inhabitants for men and women, respectively, in the group of patients over 60-year-old [18].
Second, from 2009 to 2018, an essential increase in the prevalence of MM was noted, which contrasts with data coming from other sources but is consistent with data from other latitudes. This could be related to better access to diagnosis and the increasing number of hematology and oncology units. The number of prevalent cases from 2009 was 1138 and increased to 4474 in 2018. Consequently, MM will be one of the cancers in focus in those constrained-resources countries from medical and economic perspectives.
Third, the highest prevalence is restricted to regions where hematology-oncology units are dedicated to this kind of disease. However, it is supposed that in regions like the Pacific region, there is more African American population with a known higher risk of developing MM and higher mortality risk [19].
This study has several strengths. M My MIND study is a large, nationally representative sample of the Colombian population, ensuring incidence and prevalence estimation. It allowed us to provide the overall estimation of both rates and explore the possibility of going further in the understanding of the behaviour of this disease in our country.
This study also has several limitations. First, the various missing proportion of diagnosis-related variables could have affected the estimates. Secondly, the RIPS database did not have detailed information regarding biopsies, laboratory data, tumour stage, and cause of death. The extracted patients with MM were generally diagnosed cases in all national territories. It precluded the possibility to confirm unknown MM cases from laboratory tests [20].
CONCLUSION
This is the first report of the MiMENTe study that shows the incidence, prevalence, and mortality of patients with multiple myeloma in Colombia during the 2008-2018, period. The prevalence of the disease is higher than that reported by other national registries, but the incidence and mortality are comparable with national, regional, and global information. Regional disparities in patient characteristics reflect differences in these variables. The regions with the highest incidence were those belonging to the Andean region, in which most people can easily have access to hemato-oncology centers. The highest prevalence was confirmed in Bogotá and Antioquia, and the highest mortality was observed in the Orinoco region. Prospective studies are necessary to elucidate this behaviour of MM in our country.
DECLARATION
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
CONSENT TO PUBLISH
Not applicable.
AVAILABILITY OF DATA AND MATERIALS
The datasets analysed during the current study are not publicly available due are national database but are available from corresponding author, Humberto Martinez- Cordero [email protected]. on reasonable request.
COMPETING INTERESTS
All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
AUTHOR'S CONTRIBUTIONS
Humberto Martinez Cordero: study conception and design. Alexandra Porras and Alejandro Rico acquisition, analysis, or interpretation of data. Humberto Martinez Cordero of the manuscript. Alexandra Porras and Alejandro Rico statistical analysis. GRIMMCO GRHEMUB MEMBERS: supervision.
ACKNOWLEDGEMENTS
Thanks to our collaborators who provided the data used in this work.
REFERENCES
- Costa LJ, Brill IK, Omel J, Godby K, Kumar SK, Brown EE. (2017). Recent trends in multiple myeloma incidence and survival by age, race, and ethnicity in the United States. Blood Adv. 1(4):282-287.
- Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Melton LJ 3rd. (2004). Incidence of multiple myeloma in Olmsted County, Minnesota: Trend over 6 decades. Cancer. 101(11):2667-2674.
- Martinez-Cordero H, Zapata Malagon J, Cubillos Osorio L, Rico Mendoza A, Porras Ramírez A, Ospina Idarraga J, et al. (2020). Multiple Myeloma Mortality Incidence Prevalence of Disease-Mmy Mind Study. Blood. 136(Supplement 1):10-11.
- van Nieuwenhuijzen N, Spaan I, Raymakers R, Peperzak V. (2018). From MGUS to Multiple Myeloma, a Paradigm for Clonal Evolution of Premalignant Cells. Cancer Res. 78(10):2449-2456.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 68(6):394-424.
- Cowan AJ, Allen C, Barac A, Basaleem H, Bensenor I, Curado MP, et al. (2018). Global Burden of Multiple Myeloma: A Systematic Analysis for the Global Burden of Disease Study 2016. JAMA Oncol. 4(9):1221-1227.
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. (2019). GLOBOCAN 2018, Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11. Lyon: International Agency for Research on Cancer. Available online at: http://globocan.iarc.fr (accessed March 28, 2019).
- Teras LR, DeSantis CE, Cerhan JR, Morton LM, Jemal A, Flowers CR. (2016). 2016 US lymphoid malignancy statistics by World Health Organization subtypes. CA Cancer J Clin. 66(6):443-459.
- Hernández Vargas JA, Ramírez Barbosa PX, Valbuena-Garcia AM, Acuña-Merchán LA, González-Diaz JA, Lopes G. (2021). National Cancer Information System within the Framework of Health Insurance in Colombia: A Real-World Data Approach to Evaluate Access to Cancer Care. JCO Glob Oncol. 7:1329-1340.
- Cransac A, Aho S, Chretien ML, Giroud M, Caillot D, Boulin M. (2019). Adherence to immunomodulatory drugs in patients with multiple myeloma. PLoS One. 14(3):e0214446.
- https://cuentadealtocosto.org/site/wpcontent/uploads/2021/11/CAC.Co_2021_11_3_Libro_Sit_cancer2020_v5.pdf
- Bray F, Znaor A, Cueva P, et al. (2014). Planning and Developing Population-Based Cancer Registration in Low- or Middle-Income Settings. Lyon (FR): International Agency for Research on Cancer. (IARC Technical Report, No. 43.) Chapter 6, Making the population-based cancer registry heard–reporting the results. Available from: https://www.ncbi.nlm.nih.gov/books/NBK566959/
- Wang S, Xu L, Feng J, Liu Y, Liu L, Wang J, et al. (2020). Prevalence and Incidence of Multiple Myeloma in Urban Area in China: A National Population-Based Analysis. Front Oncol. 9:1513.
- SEER Stat Fact Sheets: Kidney and Renal Pelvis. Available at: http://seer.cancer.gov/statfacts/html/kidrp.html
- Phekoo KJ, Schey SA, Richards MA, Bevan DH, Bell S, Gillett D, Møller H; Consultant Haematologists, South Thames Haematology Specialist Committee. (2004). A population study to define the incidence and survival of multiple myeloma in a National Health Service Region in UK. Br J Haematol. 127(3):299-304.
- Sant M, Allemani C, Tereanu C, De Angelis R, Capocaccia R, Visser O, HAEMACARE Working Group. (2010). Incidence of hematologic malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood. 116(19):3724-3734.
- Smith A, Howell D, Patmore R, Jack A, Roman E. (2011). Incidence of haematological malignancy by sub-type: a report from the Haematological Malignancy Research Network. Br J Cancer. 105(11):1684-1692.
- Curado MP, Oliveira MM, Silva DRM, Souza DLB. (2018). Epidemiology of multiple myeloma in 17 Latin American countries: an update. Cancer Med. 7(5):2101-2108.
- Waxman AJ, Mink PJ, Devesa SS, Anderson WF, Weiss BM, Kristinsson SY, et al. (2010). Racial disparities in incidence and outcome in multiple myeloma: a population-based study. Blood. 116(25):5501-5506.
- Pardo C, Bravo LE, Uribe C, Lopez G, Yepez MC, Navarro E, et al. (2014). Comprehensive assessment of population-based cancer registries: an experience in Colombia. J Registry Manag. 41(3):128-134.