Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2022
Evaluation and Analysis of Colon Cancer in Kingdom of Bahrain: A Retrospective Study in a Tertiary Care Center
Safa Al Shaikh*, Aalaa S. Shubbar
Salmaniya Medical Complex, Manama, Bahrain
*Corresponding Author: Dr. Safa Al Shaikh, Salmaniya Medical Complex, Manama, Bahrain. Tel: + 97 339 345 050 E-mail: [email protected]
Received Date: May 25, 2022
Published Date: July 26, 2022
ABSTRACT
Objectives: To provide an analysis for colorectal (CRC) cases including the incidence, pathological and molecular features for all cases that are diagnosed in a main tertiary hospital in Bahrain for the last four years. This will help in provide statistics about the incidence of colorectal cancer in Bahrain, also it will help in reducing the mortality and improving the patient prognosis by proper screening and genetic testing. Design: A Retrospective study. Materials and Methods: Data from our lab information system (LIS) was collected and analyzed for all patients diagnosed with colon cancer in Salmaniya Medical Complex for the period 2016-2019 and stratified according to the clinical information, histopathology and molecular testing results. Results: Between January 2016 and December 2019, 172 patients were diagnosed with colorectal carcinoma, 93 (54%) were males and 79 (46%) were females. The median age at presentation was 60 years. The most common mutated genes were TP53, KRAS, and APC genes. Limitations: The study included colorectal cancer cases that were only diagnosed by histopathology in Salmaniya Medical Complex. Patients without diagnostic biopsy or excision were not included in this study. Conclusion: Colorectal cancer presents at a younger age in Bahraini population. Due to lack of colorectal screening, we have a higher proportion of advanced stage cancer at presentation.
Keywords: Colorectal cancer, incidence, screening.
INTRODUCTION
Colorectal cancer (CRC), a major health problem, is the second most common cancer in women and the third most common in men. The incidence and mortality rate are increasing over the years as it is the third most common cause of cancer death in the world [1-2]. In Bahrain, CRC incidence as well as the mortality rates is continuously rising over the last years. Nowadays, it is becoming the second most common cancer in men and women.
More than 50% of all CRCs are attributable to modifiable risk factors. Of the cancers that begin in the colorectal area, the majority (over 95%) are classified as adenocarcinomas. CRC starts with transformation of normal colorectal epithelium into a benign adenoma, and then progress through a stepwise accumulation of genetic aberrations into a subsequent carcinoma. It occurs anywhere in the colon. However, sigmoid colon and rectum are the commonest sites. The pathologists classified CRC into: well-differentiated, moderately differentiated and poorly differentiated. The staging system is important to determine the prognosis of cancer and the outcome. In early stages (T1 and T2), the tumor invades submucosa (T1) or invades muscularis propria (T2), while in late stages (T3 and T4), the tumor invades subserosa or into non peritonealized pericolic or perirectal tissues (T3) or the tumor directly invades other organs or structures and/ or perforates visceral peritoneum(T4). Also, it is important to determine the lymph node (N) status and to determine if there is metastasis or no. The last important parameter in staging system is the distal metastasis (M) to another organ [3].
CRC is a heterogeneous disease driven by multiple genetic and epigenetic abnormalities. The most common mutated genes are TP53, KRAS, and APC genes. About 65% of CRC cases are sporadic with no family history or apparent genetic predisposition [4,5,23].
In this study, we provide an overview of the current knowledge on incidence and pathological features of colon cancer in Bahrain, as well as on molecular and genetic features, which will help in decreasing mortality rate by proper and early screening.
MATERIALS AND METHODS
This is a retrospective descriptive study. The data were obtained from our lab information system and includes all patients with colorectal cancer that have specimens sent to pathology department at Salmaniya Medical Complex, between Jan, 2016 to Dec, 2019.
Information on sex, age at presentation, clinical presentation, and pathological features (type of specimen, location of tumor, type of cancer, grade, and stage) are all documented. Tumor molecular analyses done by DNA extraction from paraffin-embedded colon cancer tissue. We marked tumor areas on H&E slide, and dissected tumor tissue by a needle. PCR and Pyro sequencing spanning BRAF codon 600, and KRAS codons 12 and 13 were carried out in an overseas laboratory.
The data analyses were conducted using Microsoft Excel software 2013. Ethical approval was obtained from the Ethics Committee in Salmaniya Medical Complex.
RESULTS AND DISCUSSION
Incidence, age, and sex:
Worldwide, CRC is the third in the term of incidence, comprising of 10% of all cancer diagnoses and second in term of mortality (9.4%) [1].
In Bahrain, colorectal cancer is the second most common cancer following lung cancer in male and breast cancer in female, while in USA it is the fourth most common cancer [2, 22].
The age standardized ratio in Bahrain is between 13.4-18.8 per 100000, which is similar to KSA and lower than USA rate which is 25.2-32.1 per 100000 [2, 7, 8].
The number of cases is continued to rise over the past years and the incidence has been steadily rising worldwide. Between January 2016 and December 2019, a total of 172 CRC cases were recorded in I-SEHA registries. Of these cases, 93 men (54%) and 79 women (46%) were diagnosed with CRC. However, 506 cases were diagnosed between 1998- 2011, 35 cases were diagnosed in 2016, 52 cases were diagnosed in 2017, 50 cases were diagnosed in 2018, and 35 cases were diagnosed in 2019.
Over the period 2016-2019, the age at the time of presentation of CRC ranged from 27 to 86 years. The median age was around 60 years for men and 58 years for women.
In our institute, among the 172 CRC cases, the incidence rate was slightly higher for men (54%, n=93) than for women (46%, n=79). Worldwide, CRC is more common among men than women and it is 3-4 times more common in developed countries than developing countries [21].
In Saudi Arabia Over the period 1994–2010, the median age for the development of CRC was 60 years for men and 55 years for women which is almost similar to our result [8].
In USA the median age for CRC for men and women was 68 and 72 years, respectively, during 2004–2010 [6]. Furthermore, CRC is most frequently diagnosed among people aged 65–74 years, which account for 36% of cases according to a study which was conducted by Siegel [13].
In our study, for the male patients, around thirty two (34%) patients were diagnosed among the age group 55-64 years, followed by twenty nine (31 %) patients were diagnosed between the age group 65-74 years. Fourteen (15%) patients were diagnosed between the age group 45-54 years and ten (11%) patients were diagnosed at age less than 45 years.
For the female patients, thirty three patients (42%) were diagnosed in the age group of 55-64 years, fifteen (19%) were diagnosed between the age group 45-54 years, and eleven patients (14%) between the age group 65-74 years. About eleven (14%) patients were diagnosed at age below 45 years. For both genders, no cases were diagnosed at age younger than 20 years and only two cases were diagnosed after the age of 84 years (Table 1). Therefore, the Bahraini patients diagnosed at younger age.
Table 1. Colorectal cancer incidence by age and sex.
|
|
Total |
|
Female |
|
Male |
|
|
|
Percentage |
Number |
Percentage |
Number |
Percentage |
Number |
Age/year |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
<20 |
|
|
3 |
5 |
5 |
4 |
1 |
1 |
20-34 |
|
|
9.5 |
16 |
9 |
7 |
10 |
9 |
35-44 |
|
|
17 |
29 |
19 |
15 |
15 |
14 |
45-54 |
|
|
38 |
65 |
42 |
33 |
34 |
32 |
55-64 |
|
|
23 |
40 |
14 |
11 |
31 |
29 |
65-74 |
|
|
9 |
15 |
10 |
8 |
8 |
7 |
75-84 |
|
|
|
2 |
1 |
1 |
1 |
1 |
>84 |
|
|
|
172 |
|
79 |
|
93 |
|
Total |
Clinical manifestation:
The most common clinical manifestations of colorectal carcinoma include change in bowel habit, anemia and hematochezia [12]. In our study, per rectal bleeding and anemia were the presenting symptoms in twenty five (14.5%) patients. Twelve (7%) patients were presented with intestinal obstruction and constipation. Ten (6%) patients were presented with abdominal pain and distention, four (2%) patients were presented with rectal polyp and another two patients (1%) were presented with weight loss. Only one patient (0.5%) was presented with diarrhea. The majority (71%) of the patients have no medical history in our pathological records.
Site of distribution:
CRCs were classified according to the anatomic primary sites into: proximal colon, distal colon, and rectum. The tumor location in the colon has an impact on the survival rate. Patients with tumor at distal colon have 69 % 5‐year survival, which is higher than patients with proximal tumors, 65%. Proximal colon tumors are associated with a higher risk of death. Also the 5-year survival for colon cancer is 55 % while it is 44.3 for rectal cancer [8-10].
In our study, the most common site of colorectal tumor is distal colon, which account for sixty five (38%) patients followed by rectum in thirty eight patients (22%) and proximal colon in thirty five patients (20%). However, in thirty four patients (20%), the site of tumor were not mentioned in the report (Table 2). These results are different from the results found in a study done in USA where the proximal colon is the most common location of colon cancer [11] (Figure 1).
There is difference in sub-site distribution by sex and age. Thus, the higher proportion of proximal tumors found more in women compared with men (25% vs 16%, respectively). However, rectal tumor is more in men. The young male is more commonly present with distal, while young female present with proximal and distal at same rate. The elderly male (above 65 years) present usually with rectal (Figure 2). It differs than USA, where rectal tumor is more common in men and women younger than 50 years [13].
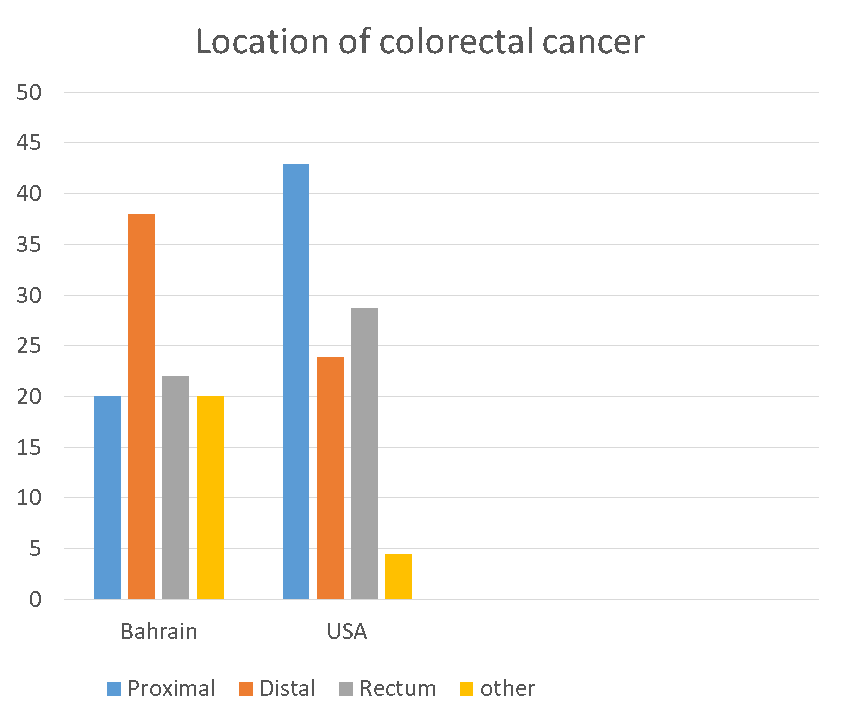
Figure 1. Colorectal cancer location in Bahrain compared to United State.
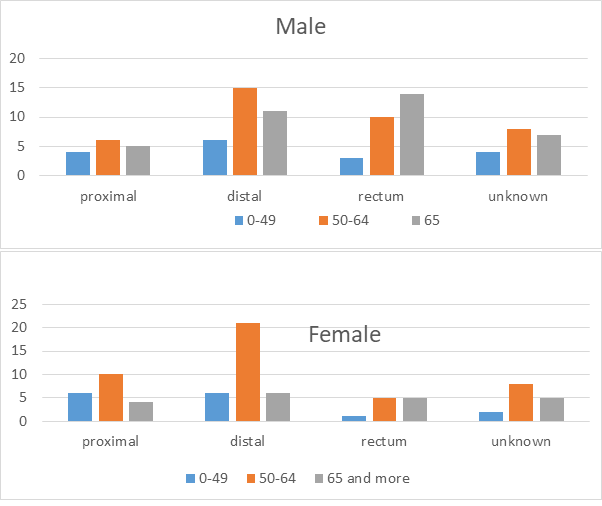
Figure 2. Distribution of colorectal cancer location according to the age and sex.
Table 2. Colorectal cancer incidence rate according to the sub site.
|
Site |
Total |
% |
Male |
% |
Female |
c |
|
Proximal |
35 |
20 |
15 |
16 |
20 |
25 |
|
Distal |
65 |
38 |
32 |
34 |
33 |
42 |
|
Rectum |
38 |
22 |
27 |
29 |
11 |
14 |
|
Unknown |
34 |
20 |
19 |
21 |
15 |
19 |
|
Total |
172 |
100 |
93 |
100 |
79 |
100 |
Grade of cancer:
Adenocarcinoma is the most common type of colon cancer in Bahrain, which is similar to the international data [12]. In our study, one hundred forty five (83%) patients were diagnosed as moderately differentiated adenocarcinoma, while five (3%) and ten (6%) patients were diagnosed as well differentiated and poorly differentiated adenocarcinoma, respectively. Adenocarcinoma, NOS was diagnosed in thirteen (7%) cases.
Stages of cancer:
According to the latest TNM pathological staging, forty seven (27%) patients were diagnosed at stage T3(tumor invades subserosa or non peritonlized per colic or perirectal fat), twenty one (12%) patients were diagnosed at stage T4(tumor that perforates visceral peritoneum or directly invades other organs or structure), seventeen 17(10%) patients were diagnosed at stage T2(tumor invades muscular is mucosa), while only six (4%) patients were diagnosed at stage T1(tumor invades sub mucosa). Eighty one (47%) patients the pathological stage was not mentioned in the pathological report. Forty eight (28%) patients showed no lymph node metastasis at the time of diagnosis. However, nineteen (11%) patients presented with N1 and twenty one (12%) patients presented with N2. Four 4 (2%) patients presented initially with distant metastasis (M1).
Genetic:
Studies showed that genetic predisposition is a risk factor for developing colorectal cancer. The risk depends on which type of gene mutation. Alterations in the RAS-RAF-MAP2K (MEK)-MAPK signaling pathway is major drivers in CRC.
BRAF V600E mutation is associated with proximal tumor location, microsatellite instability (MSI), and significantly worse patient survival in most studies. BRAF status may predict chemotherapy response and response to PDL-1 therapy [12].
Codon 12 and 13 KRAS mutations, p53 mutations in exons 5 to 8, and MSI were also determined.
In our study, the V600E BRAF mutation was detected in 3.5% (6 out of 172), KRAS in 27% (46 out of 172), NRAS in 2% (3 out of 172), TP53 in 16% (28 out of 172), PIK3CA in 2% (3 out of 172), and PTEN mutation 1% (2 out of 172) of all CRC.
Around 15% of colorectal cancer show MSI [12]. In our study, 100 (58%) cases showed no MSI, preserved protein. While 19(11%) patient loss. 53 (31%) patient unknown. Around 15% of colorectal cancer show MSI.
In one study they found the tumor tends to have a better stage-adjusted prognosis when compared with MSS tumors, and appears to be resistant to treatment with 5-fluorouracil. 14
RAS mutation is detected in 49(28%) patients, 46 (27%) patients with KRAS mutation and the remaining 3 (2%) patients with NRAS mutation. RAS mutant in 40-50% of all colorectal cancer cases [12,15] and the KRAS detected in 40% of cancer.
The Anti EGFR is ineffective in patients with RAs mutation. So the American Society for Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN) have recommended mutation analysis of the KRAS gene for candidate patients who will receive anti-EGFR therapies [16].
BRAF in 6(3%) patients. It is mutant in around 10% of colorectal cancer [17,12]. The established predictive applicability is that the Anti-EGFR will be ineffective in mutant BRAF. Also in MSI status, it may predict response to chemotherapy. In one study they found.
BRAF wild-type MSI-H tumors have the best prognosis, whereas BRAF-mutated MSS tumors are associated with the worst outcome. BRAF-mutated MSI-H tumors and BRAF wild-type MSS tumors are intermediate in terms of prognosis [17-19].
TP53 in 28(16%) patients. PIK3CA (2%) in 3 patients. PTEN in 2(2%) patients.-MSI in around 11% which is almost similar to one study 19 MSI tumors account for ~15% of colorectal
Limitations:
This was a retrospective study of 4 years duration with a relatively low number of patients.
CRC screening:
The incidence of colorectal cancer continued to rise during the past years. CRC incidence and mortality reflect the uptake of CRC screening. Screening is recommended to begin by age of 40 years in individuals at elevated risk because of family history in a first-degree relative. It is slightly more in men than women and it is occur at a younger age when compared with other countries. The mortality and morbidity can be prevented by increasing screening at a younger age.
CONCLUSION
We should pay more attention to the etiological prevention of colorectal cancer in Bahrain. In addition, only about 19% of the cases of CRC were in patients under 45 years old, which suggested that CRC prevention and control should focus on people more than 45 years old. Therefore, in Bahrain, people aged more than 45 years should be getting screened for colorectal cancer. Genetics studies played important role in the prevention, treatment, and improving patient outcomes.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
FUNDING/SUPPORT DISCLOSURE
No financial support was received in the production of this Manuscript.
REFERENCES
- Sung H, Ferlay J, Siegel ML, Laversanne M, Soerjomataram I, et al. (2021) Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Cancer journal for clinician. 71(3):145-164.
- Al Awadhi MA, Abulfateh NM, Abu-Hassan F, Majida Ahmed Fikree, Janahi E, et al. (2016). Cancer Incidence and Mortality in the Kingdom of Bahrain Statistics and Trends. Bah Med Bull; 38(1):30-34.
- American Joint Committee on Cancer. AJCC Cancer Staging Manua, Eighth Edition. https://cancerstaging.org/references-tools/deskreferences/Documents/AJCC%20Cancer%20Staging%20Form%20Supplement.pdf.
- Nguyen HT, Duong HQ. (2018).The molecular characteristics of colorectal cancer: Implications for diagnosis and therapy. Oncol Lett. 16(1): 9–18.
- Markow M, Chen W, Frankel WL. (2017). Immunohistochemical Pitfalls: Common Mistakes in the Evaluation of Lynch Syndrome. Surg Pathol Clin. 10(4):977-1007.
- National cancer institute, surveillance, epidemiology and end result program. Cancer stat facts: colorectal cancer. https://seer.cancer.gov/statfacts/html/colorect.html.
- Rawla P, Sunkara T, Barsouk A. (2019). Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 14(2):89–103.
- Alsanea N, Abduljabbar AS, Alhomoud S, Ashari LH, Hibbert D, et al. (2015). Colorectal cancer in Saudi Arabia: incidence, survival, demographics and implications for national policies. Ann Saudi Med. 35(3): 196–202.
- Surveillance, Epidemiology, and End Results (SEER) Program (seer.cancer.gov). (2016). SEER*Stat Database: Incidence‐SEER 18 Regs Research Data with Delay‐Adjustment, Malignant Only, Nov. 2015 Sub (2000‐2013) <Katrina/Rita Population Adjustment>‐Linked To County Attributes‐Total US, 1969‐2014 Counties. Bethesda, MD: National Cancer Institute, Department of Cancer Control and Population Sciences, Surveillance Research Program, Surveillance Systems Branch.
- Petrelli F, Tomasello G, Borgonovo K, Ghidini M, Turati L, et l. (2017). Prognostic Survival Associated With Left-Sided vs Right-Sided Colon Cancer: A Systematic Review and Meta-analysis. JAMA Oncol. 3(2):211-219.
- Ansa BE, Coughlin SS, Alema-Mensah E and Smith SA. (2018). Evaluation of Colorectal Cancer Incidence Trends in the United States (2000–2014). J Clin Med. 7(2):22.
- Hamilton SR, Aaltonen LA. (2000). World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Digestive System. Lyon.
- Siegel RL, Miller KD, Fedewa SA, Ahnen DJ, Meester RGS, et al. (2017). Colorectal Cancer Statistics. CA Cancer J Clin. 67(3):177–193.
- Sinicrope FA, Sargent DJ. (2012). Molecular Pathways:Microsatellite Instability in Colorectal Cancer: Prognostic,Predictive, and Therapeutic Implications. Clin Cancer Res. 18(6):1506-1512.
- Wang HL, Lopategui J, Amin MB, Patterson SD. (2010). KRAS MutationTesting in Human Cancers: The Pathologist’s Role in the Era of Personalized Medicine. Adv Anat Pathol. 17(1):23-32.
- Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH et al. (2009). American Society of Clinical Oncology Provisional Clinical Opinion: Testing for KRAS Gene Mutations in Patients With Metastatic Colorectal Carcinoma to Predict Response to Anti–Epidermal Growth Factor Receptor Monoclonal Antibody Therapy. Journal of clinical oncology. 27(12):2091-2096.
- Samowitz WS, Sweeney C, Herrick J, Albertsen H, Levin TR, et al. (2005). Poor survival associated with the BRAF V600E mutation in microsatellite-stable colon cancers. Cancer Res. 65(14):6063-6069.
- Ogino S, Shima K, Meyerhardt JA, McCleary NJ, Ng K, et al. (2012). Predictive and prognostic roles of BRAF mutation in stage III colon cancer: results from intergroup trial CALGB 89803. Clin Cancer Res. 18(3):890-900.
- Fleming M, Ravula S, Tatishchev SF and Wang HL. (2012). Colorectal Carcinoma: Pathologic Aspects. J Gastrointest Oncol. 3 (3):153-173.
- Siegel R, Miller K, Jemal A. (2017).Colorectal Cancer Facts & Figures 2017-2019. American Cancer Society, Inc. No. 861717.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 68(6):394-424.
- National cancer institute. Cancer Stat Facts: Colorectal Cancer. https://seer.cancer.gov/statfacts/html/colorect.html.
- Randall Burt. (2007) Inheritance of colorectal cancer Burt R: Inheritance of colorectal cancer. Drug Discov Today Dis Mech. 4(4):293–300.