Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Dosimetric Investigation of Modulation Capabilities of a Novel Rotating Gamma Ray System
Eldib A*, Chen L, Price RA, Ma CM
Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, PA, USA
Corresponding Author: Eldib A, Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, PA, USA; Email: [email protected]
Received Date: October 13, 2023
Publication Date: November 8, 2023
Citation: Eldib A, et al. (2023). Dosimetric Investigation of Modulation Capabilities of a Novel Rotating Gamma Ray System. Mathews J Cancer Sci. 8(3):47.
Copyright: Eldib A, et al. © (2023)
ABSTRACT
Background: Novel gamma systems with a ring type gantry capable of delivering oblique arcs have been developed recently. The expectation is that rotational systems not only reduce the number of sources utilized but can also introduce better shot modulation as compared to earlier gamma machines, which provides additional dosimetric benefits in the treatment planning process. Purpose: The aim of this work is to investigate the new optimization capabilities with a novel rotating gamma ray system (RGS). Methods: The CybeRay system is an RGS that rotates 360° in the axial direction and swings 35° in the superior direction. It includes 16 Co-60 sources focusing on the isocenter. A commercial treatment planning system was used for treatment planning with CybeRay and an in-house Monte Carlo based system was used for phantom studies. The various shot modulation options gained with this novel system were evaluated together with a simple method for dynamic dose rate delivery to overcome limitations of such rotating designs. Results: Shot modulation methodology has been evaluated in different phantoms using Monte Carlo simulations and an in-house developed graphical user interphase program. It demonstrated that one shot with weighted sectors can achieve the same coverage/conformity index as that obtained with multiple shots. This also resulted in a reduction in delivery time by 55% based on our results. The proper combination of available collimator cone sizes and various oblique beam angles allows RGS to shape the isodose lines effectively to match the target volume. Conclusion: The novel rotational system extended the gamma system capabilities in searching for the best treatment plans.
INTRODUCTION
The Gamma Knife system (Elekta Medical Systems, Stockholm, Sweden) has been very successful in stereotactic radiosurgery (SRS) [1]. The early designs used 4 collimators (helmets), and the user was required to manually change helmets. With the previous Gamma Knife models, there was no way of modulating the weight of the radiation beams and many research efforts have been directed toward finding solutions to obtain better sparing of critical structures [2-10]. In the more recent Perfexion Gamma Knife model [11], the collimator is located inside the Gamma Knife unit, and the Cobalt-60 sources are situated in 8 independently moveable sectors that slide over the collimator and are set in 1 of 4 positions corresponding to a 4, 8, or 16 mm collimator or a blocked setting. This allows for a hybrid shot where different collimator values can be used in different sectors when treating patients with lesions close to critical structures. Thus, the Perfexion model added a new feature that was not feasible with previous Gamma Knife models. However, modulation was still limited as it could only be done by blocking or changing the weight of only those 8 independently moveable sectors that housed the Cobalt-60 sources. The Perfexion model uses 192 sources and complete reloading of those sources remains a disadvantage for Gamma Knife machines.
Novel RGS machines have been developed with a ring type gantry [12,13]. The goal is to reduce some of the limitations and expand the work envelope when comparing to the former gamma systems. They provide a workspace much greater than that of the Gamma Knife. The ring gantry design used with the CybeRay system (OUR United RT Group, Xian, China) allows for both intra and extra-cranial stereotactic body radiation therapy (SBRT). In this system, one shot represents one full 360° rotation of the head comprising the Cobalt-60 sources. In addition, a planner can select a starting and ending angle and a shot will be delivered along this partial arc. This allows switching off any angles to avoid critical structures during shot delivery. Using a regular shot, the radiation output can be equal at each discrete gantry angle as the head is rotating at a fixed speed. This design allows for the modulation of the radiation output at each discrete angle. This can be achieved by changing the rotation speed and altering the time spent at each angle. The novel machine has rotational and swinging features that can extend the selective beam blocking abilities.
The schematic diagram in Figure 1 demonstrates how the head can be set to a swinging angle in the superior direction during patient treatment. Subsequently, the treatment head can rotate to deliver a full shot. The radiation beam will be in precession motion around an axis parallel to the treatment couch. This type of arc will be called, in our study, a non-coplanar arc, since the beam axis changes the plane as it rotates as compared to the coplanar arc where the beam axis is always on the same plane perpendicular to the treatment couch. The new rotating gamma design is expected to add more capabilities in some of the planning methods, in which a planner uses hybrid shots or the shot within shot technique [14].
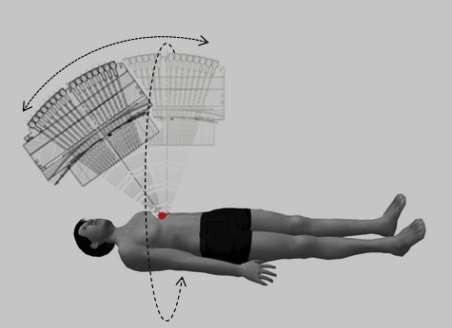
Figure 1: A schematic diagram of the machine head with a swinging angle in the superior direction.
In this work, we studied the intensity modulation of the shot delivery with the unique RGS design. We also investigated the dosimetric outcome from the use of the shot within shot technique with realistic patient plans. In the shot within shot technique, two shots having different collimator sizes are assigned the same stereotactic coordinates. The goal is to maintain the conformity of the isodose curves to the target volume. A commercial TPS (RT Pro, version 1.00.4557, Prowess, Concord, CA) was used for the treatment planning with the RGS system and an in-house Monte Carlo system was used for the phantom calculations.
MATERIAL AND METHODS
Shot Modulation
Beam weighting at different angles: In this system, intensity modulation is done by weighting the gamma beams at different angles. First, we calculated the dose distribution resulting from a regular shot delivered to a rectangular water phantom using an in-house Monte Carlo based system [15,16]. The isodose distribution is influenced by the shape of the phantom because the radiation beams traversing from the phantom surface to the isocenter will pass through different distances depending on its orientation. We then applied a weighting factor at each angular increment and, hence, reshaped the isodose lines. We compared the isodose distribution from the regular shot and the modulated arc shot in different phantoms. We repeated this study with a lung phantom where a regular shot was delivered at the phantom center and we calculated the resulting dose distribution. Then, we again applied a weighting factor at each angular increment such that beams would be depositing an equal dose at the shot isocenter despite the differences in the traversed path length.
We also tested this approach with different shaped targets drawn on a patient CT. The first studied target was oval shaped and the second target was C shaped. For both targets, optimization was conducted using RT Pro TPS utilizing regular shots with the goal of achieving conformal dose coverage. We then generated another plan using the modulated shot approach to evaluate its capability in achieving better conformity. In this approach, the sources can rotate in partial instead of full arcs and/or with different weighting of partial arc sectors (varying dose rate or rotation speed) to shape the isodose lines in accordance with the target shape.
Shot within Shot: First, a spherical phantom 15 cm in diameter and a cylindrical phantom 30 cm in diameter were modeled in the Prowess TPS. A shot is placed at the center of each phantom then a shot of a different size is placed at the same isocenter such that each shot is contributing half of the prescribed dose. We then observed the changes in the shape of the resulting isodose line and we measured the width of the 50% isodose line as seen in the transverse, sagittal and coronal views using a ruler tool from the TPS. We repeated the experiment superimposing beam shots with various beam weightings with and without swinging angles.
Treatment Planning
All RGS workspace and mechanical limits were incorporated in the RT Pro TPS to ensure the deliverability of the generated plans. The RT Pro TPS is equipped with an algorithm to optimize the shot coordinates arrangement inside the target. The algorithm works by searching for the best coverage and selectivity as defined by the equation below
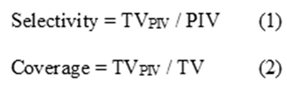
where TVPIV is the target volume covered by prescription isodose volume, TV is the target volume, and PIV is the prescription isodose volume. Each radiation shot delivers a specific dose based on the optimization results which are controlled by the gantry rotations/speed. The mechanical machine limitations controlled the lowest attainable gantry speed at 6min/rotation and the highest speed at 1min/rotation. These limits were incorporated in the TPS and were considered in the planning process. However, these limitations impose restrictions on the planning process. One method to improve plan optimization is to remove these limitations during the optimization process. Then, in order to solve the deliverability problem for shots that violate the gantry speed limits, we implemented a dynamic dose rate delivery approach shown schematically in Figure 2. For a shot of a large dose, we allowed the gantry to rotate with the lowest speed through multiple arcs.
To deliver a shot with a lower dose, shots were split into sectors with radiation beams turned off at equal intervals with the gantry rotating at maximum speed.
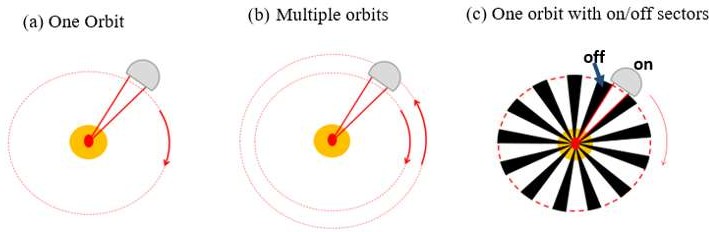
Figure 2: Schematic diagram to demonstrate the dynamic dose rate approach, a) Full rotation if the plan resulted in a shot within the machine limits, b) Multiple rotations at the same shot coordinate if a shot with a large dose is needed, c) Sectors turned off at equal intervals if a shot with a small dose is needed.
For example, assuming the dose rate at the center of a sphere phantom is 3.8 Gy/min for a full shot rotation and assuming the shot is to deliver a dose on the order of 24 Gy, this means that the gantry has to move with a speed equal to 6.3 min/rotation. This exceeds the machine limitation; however, by dividing the delivered dose between two orbits without adjusting the shot location, the dose distribution will not be altered and the gantry will only need half of the original speed to deliver the 24 Gy successfully. On the other hand, if a shot is to deliver a dose on the order of 3.7Gy, this means that the gantry has to move with a speed equal to 0.97 min/rotation. This is lower than the machine minimum attainable speed; however, the shot can still be delivered by adjusting the speed to 1 min/rotation and blocking small sectors during the gantry orbit; the dose distribution is not expected to be altered significantly as long as the blocked sectors are small and are at equal intervals. Even if one needs to use larger blocked sectors, the dosimetric change might still be favored if compared to having the shot completely undeliverable.
RESULTS
Shot modulation
Beam weighting at different angles: Figure 3.a. shows the isodose distribution resulting from one shot delivered at the center of a rectangular phantom by the full rotation of the RGS head. Elliptical isodose lines are seen due to the influence of the phantom shape as beams from the RGS head were traversing different distances at each incremental angle of the head rotation.
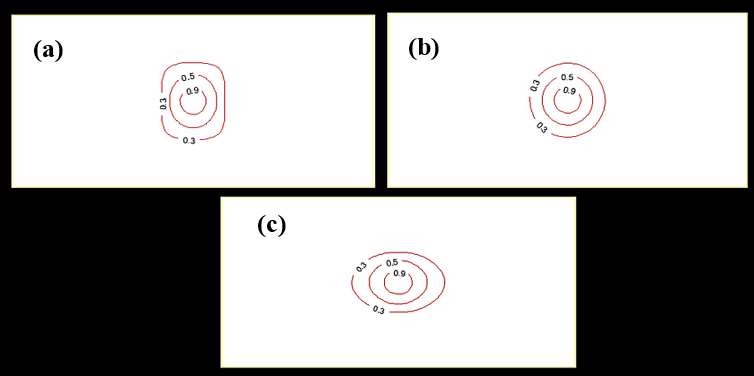
Figure 3: Isodose distribution of a single shot in rectangular phantom a) Unmodulated Full ARC shot b) Modulated to generate circular isodose lines c) Modulated to generate elliptical shaped isodose lines.
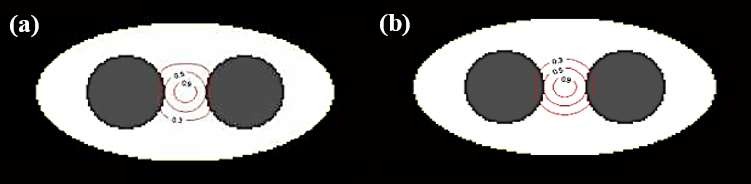
Figure 4: Isodose distribution of a single shot in lung phantom a) Unmodulated Full ARC shot b) Modulated to generate circular isodose lines.
By applying a weighting factor at each incremental sector angle, circular isodose lines were obtained as shown in Fig. 3.b. Another modulation is demonstrated in Fig. 3.c where elliptically shaped isodose lines were generated with the major axis flipped 90 degrees as compared to the isodose lines in Fig. 3.a. Fig. 4 shows another example of intensity modulation that was done for a lung phantom to generate more circularly shaped isodose lines. By modulating the weight of the arc sectors, better control can be obtained on the target coverage (i.e., isodose line shapes).
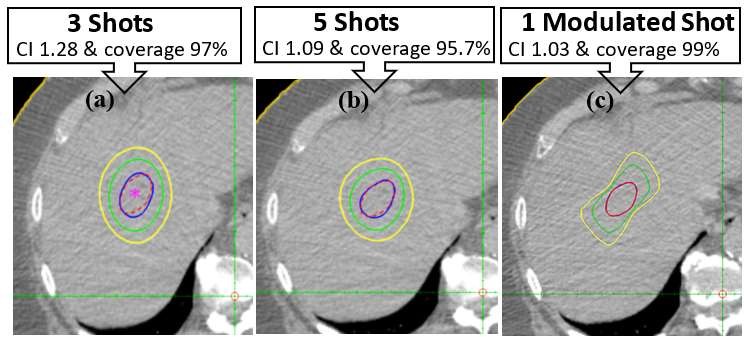
Figure 5: RGS plans with different shot numbers as compared to single modulated shot a) Isodose distribution from 3 shot plan, b) Isodose distribution from 5 shots plan, c) Isodose distribution from one single modulated shot plan.
For our first target drawn on a patient CT, a plan was generated using RT Pro TPS optimization as shown in Fig. 5. The number of shots was limited to 3 during the optimization. The resulting plan showed 97% coverage and a 1.28 conformity index. We reran the optimization after increasing the shot numbers to 5 shots. The resulting plan showed better conformity being on the order of 1.09 with a slight reduction in coverage being on the order of 95.7%. On the other hand, using modulated arc sectors with only one shot, a plan was generated with 1.03 CI and 99% coverage. Thus, one shot with weighted sectors can achieve the same coverage/conformity index as that obtained with multiple shots. This also resulted in a considerable reduction in delivery time by 55%. Our second studied target was a C shaped target. A plan was generated using regular shots and, as can be seen in Fig. 6.a, it is challenging to contour the isodose lines around this irregularly shaped target. Subsequently, another plan was created using modulated shot delivery having a combination of full and partial arcs. Figure 6.b shows better conformal isodose distribution with the use of this approach.
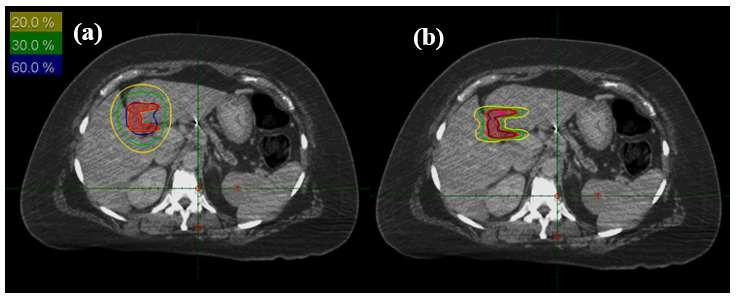
Figure 6: RGS plans using regular shots as compared to modulated shots a) Isodose distribution for a plan using regular shots, b) Isodose distribution for a plan using modulated shots.
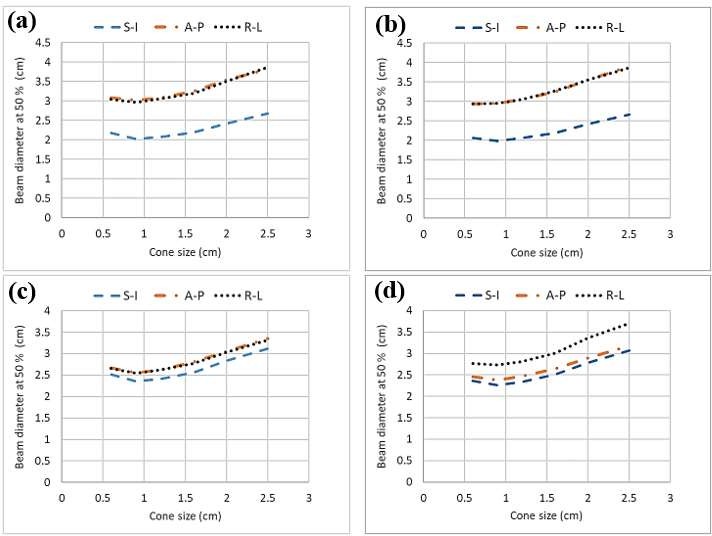
Shot within shot: It was shown that the width of the prescription isodose diameter can be changed at sub-millimeter increments depending on the superimposed cone sizes. For example, a shot delivery of 50% from a 2.5cm cone and 50% from a 0.6 cm cone on the same isocenter resulted in a 0.6 cm change in diameter in the superior-inferior direction. The swinging angle increased the shot diameter for the 2.5 cm cone in the superior-inferior direction by 0.4 cm. Superimposing a shot generated by a 2.5 cm cone with shots generated with other cone sizes on the same isocenter showed a linear relation when the beam diameter was plotted versus the additive cone size. Figure 7.a and 7.b show results with a zero swinging angle with the two phantoms and Fig. 7.c and 7.d show the same calculation, however, after using a 35 degree swinging angle. Other plans were also generated using a 2.5 cm cone superimposed with a 2 cm cone using different weighting percentages with and without a swinging angle. We plotted our results in Fig. 8 for the two phantoms. Figures 7 and 8 demonstrated that shot within shot plus a swinging angle can provide more abilities in shaping the isodose lines to improve target coverage and normal tissue sparing.
|
|
Figure 7: RGS results for superposition of a 2.5 cm cone with different cone sizes ranging from 0.6 to 2 cm and with zero and a 35 degree swinging angle, a) 15cm diameter spherical phantom and zero swinging angle, b) 30 cm diameter cylindrical phantom and zero swinging angle, c) 15cm diameter spherical phantom and 35 degree swinging angle d) 30cm diameter cylindrical phantom and 35 degree swinging angle.
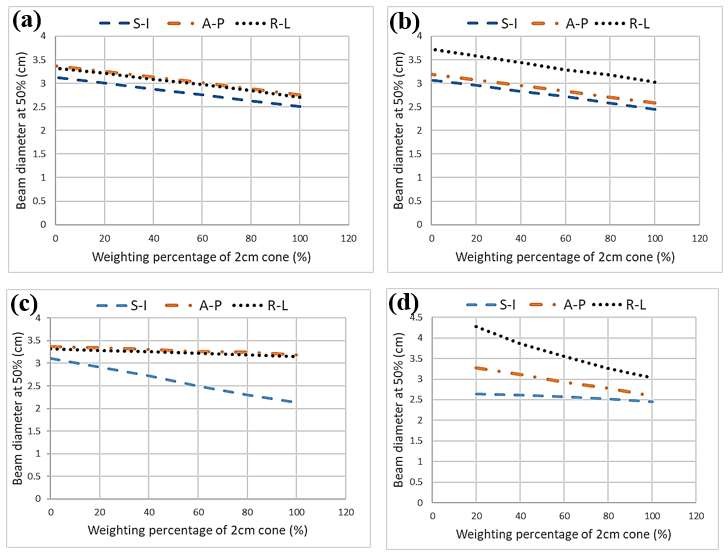
Figure 8: RGS results for superposition of 2.5cm cone with 2 cm cone size with different weighting percentages with zero and 35 degree swinging angles, a) 15cm diameter spherical phantom and zero swinging angle, b) 30cm diameter cylindrical phantom and zero swinging angle, c) 15cm diameter spherical phantom and 35 degree swinging angle d) 30cm diameter cylindrical phantom and 35 degree swinging angle.
Treatment planning
The dynamic dose rate approach with arc sector modulation was used in the treatment planning of a spine case and was helpful in tailoring the isodose lines to avoid exceeding the spinal dose limit constraints as proposed by Timmerman [17]. This can be clearly seen in Fig. 9 showing an axial view of the isodose distribution from the three modalities.
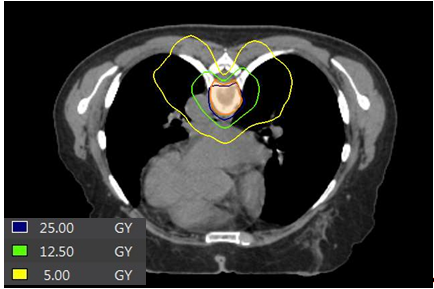
Figure 9: A spine case planned using the dynamic dose rate approach with arc-sector modulation.
CONCLUSION
The non-coplanar multiple source arrangement of the rotating gamma ray systems could improve the searching abilities in treatment plan optimization to provide superior dose distributions for SRS and SBRT applications.
ACKNOWLEDGMENT
We would like to express our thanks to Jason Li, PhD from OUR United RT Group, Xian, China for his support during conduction of this research project. We would also like to thank Binh Nguyen, PhD from Prowess Inc., Concord, CA, USA for his technical support and assistance during the treatment planning process using the RT PRO TPS.
REFERENCES
- FM K. (2010). The physics of radiation therapy. Lippincott Williams & Wilkins.
- Flickinger JC, Maitz A, Kalend A, Lunsford LD, Wu A. (1990). Treatment volume shaping with selective beam blocking using the Leksell gamma unit. Int J Radiat Oncol Biol Phys. 19(3):783-789.
- Luo L, Shu H, Yu W, Yan Y, Bao X, Fu Y. (1999). Optimizing computerized treatment planning for the Gamma Knife by source culling. Int J Radiat Oncol Biol Phys. 45(5):1339-1346.
- Ove R, Popple R. (2003). Sequential annealing-gradient Gamma-Knife radiosurgery optimization. Phys Med Biol. 48(14):2071-2080.
- Régis J, Hamdi H, Loundou A, Merly L, Castillo L, Balossier A, et al. (2021). Clinical evaluation of a real-time inverse planning for Gamma Knife radiosurgery by convex optimization: a prospective comparative trial in a series of vestibular schwannoma patients. Acta neurochirurgica. 163(4):981- 989.
- Sjolund J, Riad S, Hennix M, Nordstrom H. (2019). A linear programming approach to inverse planning in Gamma Knife radiosurgery. Med Phys. 46(4):1533-1544.
- Tian Y, Wang HD, Xu YJ, Yan Hui, Song Y, Men K, et al. (2016). Comparison of dosimetric characteristics between stationary and rotational gamma ray stereotactic radiosurgery systems based on Monte Carlo simulation. Biomed Phys Eng Expr. 2(4).
- Wu QJ, Bourland JD. (1999). Morphology-guided radiosurgery treatment planning and optimization for multiple isocenters. Med Phys. 26(10):2151-2160.
- Wu QJ, Chankong V, Jitprapaikulsarn S, et al. (2003). Real-time inverse planning for Gamma Knife radiosurgery. Med Phys. 30(11):2988-2995.
- Zhang P, Wu J, Dean D, Xing L, Xue J, Maciunas R, et al. (2003). Plug pattern optimization for gamma knife radiosurgery treatment planning. Int J Radiat Oncol Biol Phys. 55(2):420-427.
- Petti PL, Larson DA, Kunwar S. (2008). Use of hybrid shots in planning Perfexion Gamma Knife treatments for lesions close to critical structures. J Neurosurg. 109:34-40.
- Mora G, Chibani O, Eldib A, Li J, Ma CM. (2015). Monte Carlo study for the design of a Novel Gamma - Tomo SBRT System. Ifmbe Proc. 51:358-363.
- Eldib A, Chibani O, Mora G, Wang B, Li S, Miyamoto C, et al. (2016). Dosimetric Evaluation of Non-Coplanar Arc Therapy Using a Novel Rotating Gamma Ray System. Med Phy. 43(6):3613-3613.
- Bank MI, Timmerman R. (2002). Superimposition of beams to vary shot size in gamma knife stereotactic radiosurgery. J Appl Clin Med Phys. 3(1):19-25.
- Li J, Ma CM. (2002). MCBEAM: A Monte Carlo tool to simulate medical accelerators. Medical physics. 29(6):1230-1230.
- Ma CM, Li JS, Pawlicki T, Jiang SB, Deng J, Lee MC, et al. (2002). CSIM: A Monte Carlo dose verification tool for radiation therapy treatment planning and beam delivery. Med Phy. 29(6):1316-1316.
- Timmerman RD. (2008). An overview of hypofractionation and introduction to this issue of Seminars in Radiation Oncology. Semin Radiat Oncol. 18(4):215-222.