Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2023
Cognitive Evaluation and Health Changes in a Prison Unit in Santa Catarina
Keli Dias Feltrin1, Iara Pereira Fernandes1, Susane Raquel Périco Pavei2, Diogo Dominguini2,*
1Graduation in nursing, University of Southern Santa Catarina (UNESC), Criciúma, 88806-000, SC, Brazil
2Professor, Department of Health Sciences, University of Southern Santa Catarina (UNESC), Criciúma, 88806-000, SC, Brazil
*Corresponding author: Diogo Dominguini, Professor, Department of Health Sciences, University of Southern Santa Catarina (UNESC), Criciúma, 88806-000, SC, Brazil; Tel: +5548988157084; Email: [email protected]
Received Date: January 27, 2023
Publication Date: February 15, 2023
Citation: Feltrin KD, et al. (2023). Cognitive Evaluation and Health Changes in a Prison Unit in Santa Catarina. Mathews J Psychiatry Ment Health. 8(1):37.
Copyright: Feltrin KD, et al. © (2023).
ABSTRACT
In 2003, the Interministerial Ordinance No. 1,777 was created, which instituted the National Health Plan in the Penitentiary System, which was implemented through the participation of the Ministries of Health and Justice together with the National Council of Secretaries of Health, the National Council of Municipal Health Secretaries and the National Council for Criminal and Penitentiary Policy. In recent years, the growth of the prison population in Brazil has generated numerous debates, mainly focused on improving living conditions in the prison system. Thus, the present research had the general objective of evaluating cognition and health changes within a Prison Unit in Santa Catarina, verifying the importance of resocialization in the quality of life of people from this population. The Prison Unit has a very flexible population, housing, approximately, 1,000 male inmates, with a multiprofessional health team, in which it welcomes from the simplest toth to most complex diversities of complaints, with a wide variety of physical, psychological and mental. To obtain the data, a quantitative, exploratory and Field research was carried out, with 30 in mates between 18 and 30 years of age, according to inclusion criteria, applying three instruments for cognitive assessment, as well as health changes, including the Assist 2.0scale, BIS-11 scale, Addenbrooke's cognitive exam and the nursing consultation with the sociodemographic questionnaire. For statistical analyses, the statistical program Statistical Package for the Social Sciences was used, considering a significance level of 5% (p< 0.05).
Keywords: Mental health, Cognition, Assist 2.0 scale, Addenbrooke cognitive exam, BIS-11 scale
INTRODUCTION
According to the National Penitentiary Department (DEPEN), the Brazilian prison population reached the number of 820,689 in June 2021. Of these, 673,614 are in physical cells and 141,002 are under house arrest (SISDEPEN, 2021). The state of Santa Catarina has been considered a model for the country in the rehabilitation of prisoners, and in April 2019, DEPEN, through a technical note, recommended the work activity model and the system of the Santa Catarina Revolving Fund as a practice to be adopted in all states [1]. Work and education are security strategies in our prison units. It is scientifically proven that work and educational activities make units safer [2].
In 2003, Interministerial Ordinance n.º 1.777 was created, which instituted the National Health Plan in the Penitentiary System, developed to include the penitentiary population in the Unified Health System (SUS), aiming at giving these people the right to citizenship, taking effect from the perspective of human rights [3]. This population's access to health actions and services is legally defined by the Federal Constitution of 1988, by Law No. 8080 of 1990, which regulates the Unified Health System, by Law No. 8142 of 1990, which provides for participation of the community in the management of the Unified Health System, and by the Penal Execution Law n.º 7210 of 19843.
The model of mental health care in Brazil, currently, is based on community and territorial care, which aims to reduce hospitalizations and services in tertiary care, prioritizing primary care services. To guide issues regarding mental health care, the Ministry of Health material was released: “The SUS from A to Z”, which aimed to clarify for the Brazilian population some concepts about health policy [4].
Based on the National Policy for Comprehensive Health Care for Persons Deprived of Liberty in the Prison System (PNAISP), services and multidisciplinary primary care teams were defined, considering the characteristics of each prison unit. The nurse who is part of this team must have the attribution of a qualified look at issues of confinement and vulnerability, with the aim of not only observing the health status of these individuals, but also the biopsychosocial aspects [5].
The nurse's role is preventive in nature, where laboratory tests are collected and educational campaigns are carried out on the most common diseases in prisons. It is the responsibility of the nurse to plan care and implement vaccination policies,as well as control their periodicity; the planning of policies for the prevention and control of health promotion, within the scope of its competence; carrying out nursing consultations and requesting complementary exams; prescription of drugs within the legal provisions of the profession and other complementary norms, and may also hold periodic lectures in order to address issues related to diseases, signs and symptoms, possible complications and forms of prevention [6]. To evaluate cognition and health changes in inmates aged 18 to 30 years old in a Prison Unit in a city in the south of State of Santa Catarina.
METHOD
The research was carried out in a Prison Unit in Santa Catarina. The unit has approximately 1000 male inmates, and the research was authorized by the current director of the unit upon presentation of the project, with the signature and stamp of the letter of acceptance. According to the sample calculation, the survey was carried out with 30 male inmates, aged between 18 and 30 years old, who entered the prison unit between April 1, 2022 and July 1, 2022.
The application of the nursing consultation instrument carried out by the researchers, in which they were guided for data collection, was adapted and based on Elizabeth Hidelgard Peplau's nursing theory, which has a main focus on the study of interpersonal relationships. The theory can be applied to nursing care practice, meeting the precepts of the psychiatric reform. In addition, it addresses Peplau's Theory within mental health care, in order to promote social inclusion and rescue people's citizenship, reinserting these people into their families and society through the role of nurses [7].
This nursing theory is based on an interpersonal, interdisciplinary, community and family-related relationship, assuming that human growth and development and related actions are influenced by both the patient and the nurse. The patient is seen as a whole, addressing the biological, psychological, spiritual and sociological aspects. Peplau identifies four sequential phases in interpersonal relationships, including orientation, identification, exploration and resolution [7]. Soon after the nursing consultation, neuropsychiatric tests were Applied Addenbrooke Cognitive Examination, BIS-11 scale and Assist 2.0 scale. Subsequently, the data were interpreted and analyzed.
ADDENBROOKE COGNITIVE EXAMINATION
The revised version of the Addenbrooke Cognitive Examination (ACE-R) is an instrument with high sensitivity and specificity to detect mild stage dementia, consisting of a brief cognitive assessment test. It consists of five items that aim to assess the four main cognitive domains (orientation, memory, language and visuospatial function), with a maximum score of 30 points and a completion time of fifteen minutes [8].
BIS SCALE 11
The BIS-11 scale is a self-administered scale composed of 30 items related to manifestations of impulsivity, based on the theoretical model proposed by Ernst Barratt. The proband must analyze each of the items, considering their own behavior, and classify them according to a four-point Likert-type scale, namely: 1 = rarely or never; 2 = from time to time; 3 = often; 4 = almost always/always. Scale scores range from 30 to 120 points, and high scores indicate the presence of impulsive behaviors. In addition to a global score, the BIS-11 allows the calculation of partial scores referring to three subdomains of impulsivity, namely motor impulsivity (items 2, 3, 4, 16, 17, 19, 21, 22, 23, 25 and 30*), attentional (items 6, 5, 9*, 11, 20*, 24, 26, 28) and non-planning (items 1*, 7*, 8*, 10*, 12*, 13*, 14 , 15*, 18, 27, 29*) [9].
ASSIST SCALE 2.0
The questions on the Assist 2.0 scale address frequency of use, in life and in the last three months, problems related to use, concern about use by people close to the user, impairment in performing expected tasks, unsuccessful attempts to stop or reduce use, cravings, and injection use. Each answer corresponds to a score, which varies from 0 to 4, and the total sum can vary from 0 to 20 points. A score range from 0 to 3 is considered as indicative of occasional use, from 4 to 15 as indicative of abuse and above 16 as suggestive of dependence [10].
For the analysis of quantitative data, it was tabulated initially in Excel software. Data were analyzed using the SPSS statistical program, version 22. Variables were described using frequencies, means and standard deviations. Pearson's chi-square test was used to test the association between categorical variables. Ordinal variables were compared using the chi-square linear trend test. For cognitive tests, Addenbrooke's Cognitive Examination score, BIS Scale 11 and Assist Scale 2.0 were calculated. When comparing dichotomous variables with a quantitative variable, Student's t test was used. Results were considered significant when p<0.05.
The present study was submitted to the Research Ethics Committee (CEP) of the University of Extremo Sul Catarinense (UNESC). As soon as it was approved, the research began, following the ethical principles established in Resolution No. 466 of December 12, 2012, of the National Health Council (NHC).
DATA ANALYSIS
After approval of the research, data collection began, which aimed to assess cognition and health changes with 30 inmates aged 18 to 30 years old in a Prison Unit in Santa Catarina.
Among the prisoners included in the study, most have an average age of 26 years old, totaling 20% of those surveyed. However, the sample consists of an age group ranging from 18 years to 30 years old, consisting of 66.7% singles and 33.3% incomplete high school, as shown in Table 1.
Table 1: Sociodemographic characteristics of the sample.
|
Variables |
N |
% |
p |
|
Age |
0,328 |
||
|
21 |
1 |
3,3 |
|
|
22 |
3 |
10,0 |
|
|
23 |
2 |
6,7 |
|
|
25 |
3 |
10,0 |
|
|
26 |
6 |
20,0 |
|
|
27 |
3 |
10,0 |
|
|
28 |
4 |
13,3 |
|
|
Marital status |
|
|
0,023 |
|
Singe |
20 |
66,7 |
|
|
Married |
5 |
16,7 |
|
|
Separated |
1 |
3,3 |
|
|
Co-residing with parther |
1 |
3,3 |
|
|
Education level |
|
|
0,487 |
|
Lower than 4th grade |
2 |
6,7 |
|
|
Completed 4th grade |
2 |
6,7 |
|
|
Secondary level incomplete |
10 |
33,3 |
|
|
Secondary level |
7 |
23,3 |
|
|
University level |
1 |
3,3 |
|
|
Primary level |
4 |
13,3 |
|
According to the sociodemographic profile analyzed by Fovet T, et al. [21], 11 49.7% were people between 18 and 19 years old, 50.3% had secondary education and 43.7% were single. In research by Santos T, et al. [22] 12, 88.89% had incomplete primary education and 33.33% were separated.
Carvalho ML, et al. [13] demonstrated, through his studies, that 45.4% of the prisoners were single and 70.4% had incomplete elementary school. Saffi F. [14] states that 65% of the prisoners were young people aged up to 30 years, 58% had between the 5th and 8th grades of elementary school, 46.51% were single and 34.88% had no children.
Regarding the employment situation, 80% of the inmates are unemployed at the moment and 56.7% worked full time before their imprisonment. There are few studies showing the labor situation of inmates, making it necessary more research addressing this topic, knowing its benefits for mental health. According to research carried out by Fovet [11], 71.5% of the prison population were unemployed.
Bearing in mind that Santa Catarina is a model in terms of employment, the numbers analyzed show that most inmates are not working at the moment. Work helps in the physical and psychological maintenance of people, being an important factor in resocialization and introduction into society.
The type of visit with the highest adherence was the group visit (33.33%), which includes family members or partners who have a proven bond and who have no impediments to this, followed by video calls (30%), which are carried out through videoconferencing, allowing visual and sound contact between inmates and visitors. This tool can be used by the family member who is registered on the list of visits by the inmates, and this modality was implemented with the beginning of the pandemic in 2019 and maintained until today, facilitating contact with family members who live in distant cities. In addition, 16.66% receive an intimate visit, which is a right that the prisoner has to maintain intimate meetings on a regular basis with their spouse, whose legal justification lies in its importance in strengthening family relationships; and 20% do not receive any type of visit, either by their own will or because of abandonment by the family. According to Carvalho ML, et al. [23], 26.9% of the inmates received intimate visits in their study.
The rising rate of incarceration has a negative impact on the concomitantly growing population of children and young people who are relatives of inmates. The incarceration rate in the United States has more than quadrupled since the 1970 and has led to the United States of America having the highest incarceration rate and largest prison population in the world, with disproportionate increases found among racial and ethnic minority groups [15]. According to Saffi F. [14], 40% of prisoners have at least one family member who has already been through the prison system.
This expansion in incarceration is particularly devastating for the more than 2 million children and young relatives of family members of those incarcerated, with children more likely to experience greater lifetime risks, including an increased likelihood of behavioral health problems. , such as mental health impairment and substance abuse [15].
A significant number of children have parents, caregivers and family with a history of incarceration in the United States, creating the potential for an ever-growing population at high life-course risk [15].
The present research showed that among the interviewees, more than half of the inmates (60%) were related to someone who had already been in prison, including a brother or sister (20%); father, mother, stepfather and uncle (16.66%); cousin (13.33%) and brother-in-law (3.33%), reinforcing the citations of the authors above regarding the idea that this population is more vulnerable, prone to health problems and substance abuse, as they are influenced by the lifestyle of family members and the environment in which they live.
A significant number of children have parents, caregivers and family with a history of incarceration in the United States, creating the potential for an ever-growing population at high life-course risk [15].
Carvalho ML, et al. [13], in one of his studies, demonstrates that 42% of the main criminal articles were theft, being strongly associated with the male gender, followed by 35% by drug trafficking, with these being 1.21 times more likely to consume drugs before imprisonment.
This research brings differentiated data, where 56.7% of the inmates are serving a sentence for drug trafficking, which are classified as drug trafficking (selling, buying, producing, storing, transporting, importing, exporting, offering or delivering for consumption), even if for free, among other conducts, being a major national problem, driving other crimes; 16.6% serve a sentence for homicide, which is the act of killing a person, either voluntarily or involuntarily; followed by 13.3% for armed robbery, subtracting a movable object belonging to themselves or others, through serious threat or violence to the person; and 13.3% for theft, subtracting someone else's mobile object for themselves or someone else.
Some study findings demonstrate worsening of depressive symptoms and life satisfaction during incarceration. In addition, detainees placed in solitary confinement suffer greatly, and such confinement has serious short- and long-term repercussions. For example, inmates in solitary confinement in the New York City prison system were 6.27 times more likely to have potentially fatal self-harm (including hanging and poison ingestion) than those not placed in solitary confinement [16].
Overall, physical and psychological well-being worsens for prisoners, while mortality decreases [16]. According to research data by Santos T, et al. [12], 44.44% of the inmates had not yet been judged and, therefore, did not have their length of imprisonment defined. According to Saffi F. [14], the average length of imprisonment for 44.19% of prisoners was between 05 and 10 years.
However, most research on inmate mental health, while acknowledging the high prevalence of mental health problems in correctional populations, has not tested whether mental health changes as a result of incarceration [16].
The present research demonstrated that 23.3% of the inmates have been imprisoned for 5 to 10 years, 20% for 3 to 4 years, 16.7% for 1 to 2 years, 16.7% have not yet been tried, 13, 3% over 10 years, 6.7% up to 3 months and 3.3% from 04 months to 11 months, as shown in Table 1. With 46.6% having already been submitted to isolation as a safety measure or for health reasons, 33.3% were isolated in a disciplinary cell, and in this environment the inmate cannot sunbathe or have contact with other inmates, also losing the right to visit; 10% in a collective cell, where all the members of the cell stay, allowing sunbathing and visits via video call, and 3.3% in an intimate cell, used as isolation during a pandemic for prisoners with health problems.
The research shows that 33.3% of the inmates considered themselves quite physically active before their imprisonment, 46.7% consider their physical activity moderate in the last four weeks, and 60% consider this daily routine. It is known that physical activity is directly related to improved quality of life and considerably reduces the risk of developing physical and psychological illnesses.
When researching the leisure item, it was found that 36% use the patio as recreational time, 29% play football, 18% cite the library, 11% prefer sunbathing, 3% radio and another 3% did not present moments of leisure. Leisure is associated with improved quality of life and health promotion, favoring socialization. It is worth noting that this modality is not mandatory, but it is the right of inmates.
The BIS-11 scale was classified as shown in Graph 1, with three classifications: motor impulsivity, attentional impulsivity and unplanned impulsivity, and according to research data, the highest index is that of unplanned impulsivity. Respondents were classified with 53.33% for unplanned impulsivity, 40% for motor impulsivity and 6.66% for people with attentional impulsivity.
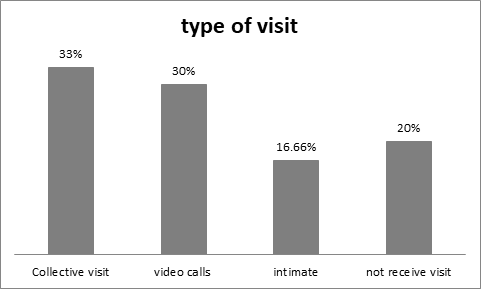
Figure 1: Type of visit received by the sample.
Fonte: author’s research (2022).
It is thought that impulsivity and seizures underlie violent behavior. Impulsivity is related to decreased cognitive control, increased risk and behavioral disinhibition, such as drug addiction [17].
Recent advances in understanding the neurocircuitry of impulsivity and compulsivity have led to the idea that many behaviors that are not considered right, such as committing crimes, share these two dimensions (impulsivity and compulsivity). Impulsive and compulsive disorders, including aggression and therefore the commission of crimes, are caused in part by inefficient processing of information in executive functions. Impulsive and compulsive behaviors are both characterized by the inability to inhibit or delay the behavior, which is related to the prefrontal cortex. Compulsive behavior seems to be associated with increased frontal lobe activity, while impulsive behavior may be associated with reduced activity in this region [17].
Through the application of the Assist scale, it was possible to assess which were the most used psychoactive substances among the sample, in addition to allowing the detection of their abuse/dependence.
Graph 2 shows that alcohol was the most used substance among the sample, totaling 63.33%, followed by marijuana (56.67%), tobacco derivatives (46.66%), cocaine/crack (30%), amphetamines/ecstasy (13.33%), inhalants (13.33%), hallucinogens (13.33%) and others (3.33%).
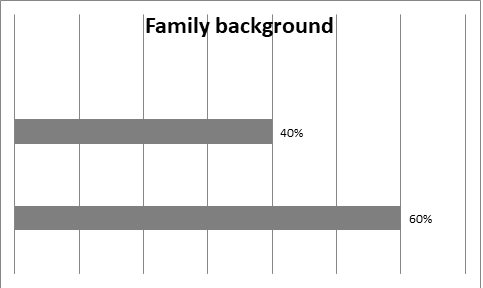
Figure 2: Family members in a situation of reclusion according to the sample.
Fonte: author’s research (2022).
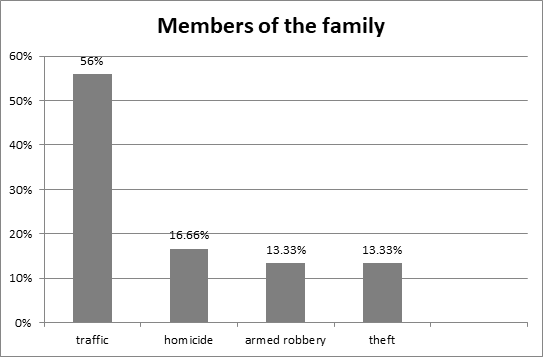
Figure 3: Kinship of family members with a history of imprisinment.
Fonte: author’s research (2022).
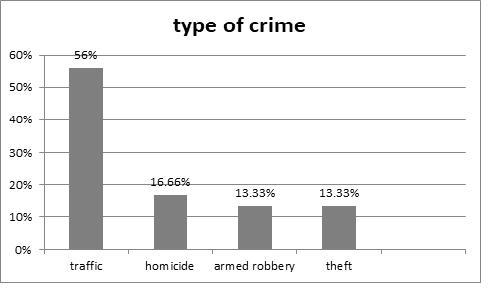
Figure 4: Types of crimes committed by the sample.
Fonte: author’s research (2022).
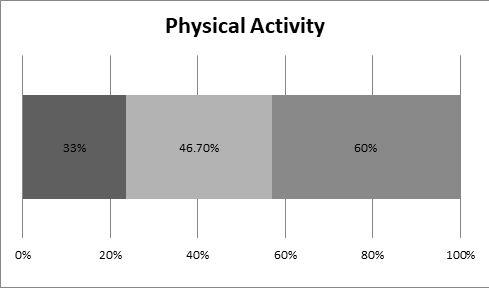
Figura 5: Rate of performance of physical activity by the sample
Fonte: author’s research (2022).
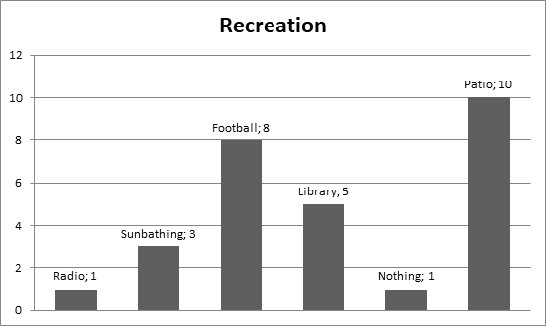
Figure 6: Moments of leisure performed by the sample.
Fonte: author’s research (2022).
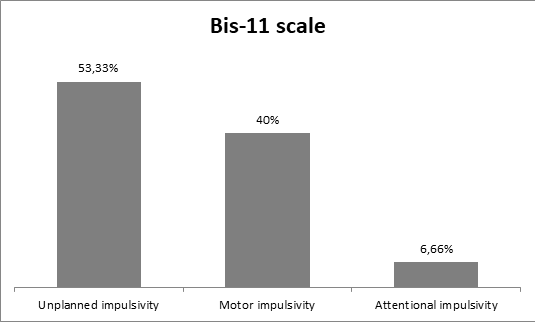
Figure 7: Bis-11 scale according with the sample answers.
Fonte: author’s research (2022).
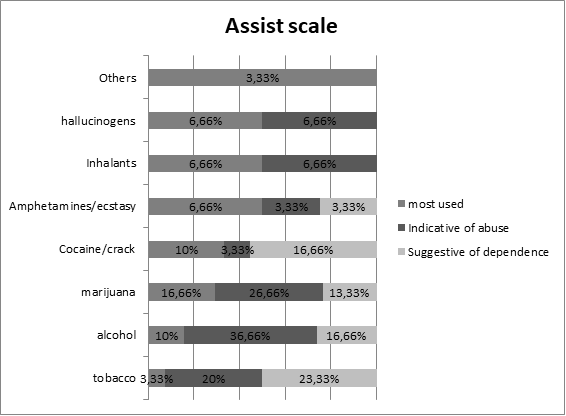
Figura 8: Assist scale according with the sample answers.
Fonte: author’s research (2022).
The substance most suggestive of dependence was tobacco (23.33%), followed by alcohol (16.66%) and cocaine/crack (16.66%), marijuana (13.33%) and amphetamines/ecstasy (3.33%). Indicative of first substance abuse was alcohol (36.66%), marijuana (26.66%), tobacco derivatives (20%), inhalants and hallucinogens (6.66%) and amphetamines/ecstasy (3.33 %).
According to research by Fovet T, et al. [18], substance use is higher in the prison population than in the general population (alcohol: 62.1% vs. 56.4%, p = 0.007; cannabis: 45.6% vs. 13.9%). Anxiety and concomitant mood disorders were particularly more frequent in prison than in the general population [18].
Regarding the main drugs used before imprisonment, 74.3% of the inmates answered alcohol, followed by 61.8% marijuana. When asked about the main drugs used in prison, 57.4% answered none, 27.7% marijuana, 18.8% cocaine, 18.5% tranquilizers and 9.7% alcohol [13]. In addition, 88.37% have already used illicit drugs, the most used being cocaine, marijuana and solvents [14].
Researchers speculate that the protective effects of current incarceration for this group may be driven by decreased risk of death from violence or accidents, reduced access to illicit drugs and alcohol, and improved access to health care, although these mechanisms remain to be debated [16].
The ACE-R tool showed results indicative of cognitive deficits in 23.33% of the individuals. Thus, 76.67% of the participants were able to reach the established score for this instrument. The average of the total value obtained in the ACE-R was 75.47 points, with a minimum of 54 points and a maximum of 88 points, with a cut-off score of 69 points (Table 2).
Table 2: Sociodemographic based in incarcerated characteristics of the sample.
|
Variables |
n |
% |
P |
|
Isolation in incarceration |
|
|
0,234 |
|
None |
16 |
53,3 |
|
|
Disciplinary cell |
10 |
33,3 |
|
|
Collective cell |
3 |
10,0 |
|
|
Inmate cell |
1 |
3,3 |
|
|
Time of incarceration |
|
|
0,471 |
|
0 a 3 months |
2 |
6,7 |
|
|
4 a 11 months |
1 |
3,3 |
|
|
1 a 2 years |
5 |
16,7 |
|
|
3 a 4 years |
6 |
20,0 |
|
|
5 a 10 years |
7 |
23,3 |
|
|
More than 10 years |
4 |
13,3 |
|
|
Don’t know |
5 |
16,7 |
|
César KG, et al. [19] comments that to distinguish the normal cognitive level from dementia, a cutoff point of 64 points was established (91% sensitivity and 76% specificity) and to differentiate the normal cognitive level from cognitive decline without dementia the best cutoff point was 69 points (73% sensitivity and 65% specificity). Cutoff points varied according to education.
FINAL CONSIDERATION
The research brought expected results and some that surprised us due to behavioral preconceptions regarding inmates. We conclude that the population with the highest incidence in prisons belongs to the age group between 18 and 30 years old, who are single men with incomplete high school education, and that 57% of these are serving a criminal article for drug trafficking, followed by articles such as armed robbery, robbery and homicide.
One of the impacts of confinement demonstrates a classification of impulsivity in 3 major behavioral proportions. The ranking shows “lack of planning”, who do not think about the future and live in the present moment; second appears “motor impulsivity”, which demonstrates the inhibition of responses inconsistent with the context and, finally, “attentional impulsivity”, which is related to quick decision-making.
Another point observed, no less important, was the abuse of psychoactive substances in a disorderly and influenced way before, during and after imprisonment. Questions about health changes show that the vast majority (64%) have already had contact with some type of drug, with alcohol being the most used, followed by marijuana.
Another item indicative of a greater proportion in the application of the Assist scale brings alcohol (36.66%) as the main “indicator of abuse”; another topic on the scale suggestive of dependence brings tobacco derivatives (23.33%), followed by alcohol and cocaine (16.66%). Occasional use, not very unnoticed or uncommon, brings the use of marijuana (16.66%) and other illicit drugs (6.69%).
In the cognitive assessment, surprising data showed that, among those surveyed, 76.67% did not present cognitive impairment or cognition decline. It was found that the housing change did not cause behavioral and functional changes by the results found. The confirmation of all these alterations and changes are poorly studied and with very few publications.
Within the context of the penitentiary system, it is observed that the nurse plays a fundamental role, however, often restricted, due to the organization of the system.
What is observed in practice is that the performance of this professional has increasingly implied the improvement of health care in the prison environment, since the nurse is able to adapt, provide resoluteness and allow full access to the locked into the health system.
In fact, due to the small sample, the study has a certain limitation, however it will serve to direct new public policies aimed at mental health. The nurse is the professional able to provide resolutive, continuous and qualified comprehensive assistance to the health needs of the prison population, in addition to contributing to the control of the most affected diseases in this environment, defining and implementing actions and services in accordance with the principles and guidelines of the SUS.
REFERENCIES
- Governo De Santa Catarina. (2022). Santa Catarina sedia reunião do Consej e SAP realiza mostra laboral do sistema prisional.
- Lima L. (2019). Sucesso da política de ressocialização no sistema prisional catarinense é destaque de audiência pública.
- Brasil. (2003). Portaria Interministerial MS/MJ n. 1.777, de 09 de setembro de 2003. Aprova o Plano Nacional de Saúde no Sistema Penitenciário. Brasília, 2003.
- Lima FG, siciliani CC, Drehmer lBR. (2012). O perfil atual da saúde mental na atenção primária brasileira. Comunicação em Ciências da Saúde. 24:143-148.
- Carvalho SA. (2018). A saúde no sistema prisional brasileiro: uma revisão integrativa. Monografia (Bacharelado em Enfermagem) – Universidade de Brasília. Brasília:32.
- Cofen. (2011). Conselho Federal de Enfermagem. A atuação da Enfermagem na assistência à saúde da população carcerária.
- Cardoso TVM, Oliveira RMP, Loyola CMD. (2006). Um entendimento linear sobre a teoria de Peplau e os princípios da reforma psiquiátrica brasileira. Escola Anna Nery. 10:718-724.
- Miranda DC. (2018). Mini-addenbrooke’scognitiveexamination (M-ACE) como instrumento de avaliação cognitiva breve no comprometimento cognitivo leve e doença de Alzheimer leve. Dissertação (Mestrado em Ciências) – Universidade de São Paulo.São Paulo:91.
- Malloy-diniz lF, Mattos P, Leite WB, Abreu N, Coutinho G, de Paula JJ, Tavares H, Vasconcelos, AG, Fuentes D. (2010). Tradução e adaptação cultural da BarrattImpulsivenessScale (BIS-11) para aplicação em adultos brasileiros. Jornal Brasileiro Psiquiatria. 59:99-105.
- Henrique IFS, Micheli D, Lacerda RB, Lacerda LA, Formigoni MLOS. (2004). Validação da versão brasileira do teste de triagem do envolvimento com álcool, cigarro e outras substâncias. Revista da Associação Médica Brasileira. 50: 199-206.
- Fovet T, Plancke L, Amariei A, Benradia I, Carton Fsya, Kyheng M, Tasniere G, Amad A, Danel T, Thomas P, Roelandt J. (2020). Mental disorders on admission to jail: a study of prevalence and a comparison with a Community sample in the north of France. Eu Psychiatry. 63:1-7.
- Santos T, Saccol M. (2015). Perfil sociodemográfico dos presidiários homicidas de joaçaba, SC e sua relação com o crime.Unoesc & Ciência – ACBS. 6:105-114.
- Carvalho ML, Valente JG, Assis SG, Vasconcelos AGG. (2006). Perfil dos internos no sistema prisional do Rio de Janeiro: especificidades de gênero no processo de exclusão social. Ciência & Saúde Coletiva. 11:461-470.
- Saffi F. (2009). Avaliação de terapia cognitiva-comportamental para prevenção de reincidência penitenciária. Dissertação (Mestrado em Psiquiatria) - Faculdade de Medicina, Universidade de São Paulo. São Paulo.
- Fleming CM, Nurius PS. (2019). Incarceration and adversity histories: modeling life course pathway saffecting behavior al health. Am J Orthopsychiatry. 90:312-323.
- Wildeman C, Wang E. (2017). Mass incarceration, public health, and widening inequality in the USA. America: Equity and Quality in Health. Lancet. 389:1464-1474.
- López-Torrecillas F, Castillo-Fernández E, Ramírez-Uclés I, Martín I. (2021). Impulsivity and Compulsivity and Their Relationship with Non-Adherence to Treatment in the Prison Population. Int J Environ Res. Public Health. 1:1-10.
- Fovet T, Wathelet M, Benbouriche M, Benradia I, Roelandt Jl, Thomas P, et al. (2022). Substance Use, Substance Use Disorders, and Co-Occurring Psychiatric Disorders in Recently Incarcerated Men: A Comparison with the General Population. Eur Addict Res. 1:368-376.
- César KG, Yassuda MS, Porto FHG, Brucki SMD, Nitrini R. (2017). Addenbrooke's cognitive examination-revised: normative and accuracy data for seniors with heterogeneous educational level in brazil. Int Psychogeriatr. 29:1345-1353.