Information Links
Related Conferences
Previous Issues Volume 8, Issue 3 - 2023
Catatonia and Brain Tumor: Review and Illustrative Case Report
Thales Pimenta de Figueiredo1, Paulo Henrique Teixeira Prado2, Jadison Luiz Barbosa Junior3, Caio Hage Chahine Kubrusly4, Isabela Maria Seabra Leite5, Luiz Filipe Silva Codorino Couto6, Paulo Marcos Brasil Rocha7,*
1MD, Hospital das Clínicas da Universidade Federal de Minas Gerais (HC-UFMG), Brazil
2MD, Universidade Federal de Minas Gerais (UFMG), Brazil
3MD, Hospital das Clínicas da Universidade Federal de Minas Gerais (HC-UFMG), Brazil
4MD, Hospital das Clínicas da Universidade Federal de Minas Gerais (HC-UFMG), Brazil
5MD, Hospital das Clínicas da Universidade Federal de Minas Gerais (HC-UFMG), Brazil
6MD, Hospital das Clínicas da Universidade Federal de Minas Gerais (HC-UFMG), Brazil
7MD, Ph.D, Professor Adjunto, Departamento de Saúde Mental, Universidade Federal de Minas Gerais (UFMG), Brazil
*Corresponding author: Dr. Paulo Marcos Brasil Rocha, MD, Ph.D, Avenida Professor Alfredo Balena, 190, room 267/Belo Horizonte–MG, Brazil, Postal Code 30130-100, Tel: +55 0xx 31 99121-2064; Email: [email protected].
Received Date: August 31, 2023
Published Date: September 13, 2023
Citation: Rocha PMB, et al. (2023). Catatonia and Brain Tumor: Review and Illustrative Case Report. Mathews J Psychiatry Ment Health. 8(3):41.
Copyrights: Rocha PMB, et al. © (2023).
ABSTRACT
Case Report: This literature review is accompanied by an illustrative case of a woman diagnosed with a Stage IV invasive ductal breast carcinoma who evolved with a catatonic syndrome due to a metastatic brain tumor. Objective: It aims to forward the understanding of how catatonia emerges from organic brain tumoral lesions and how can it be treated properly. Methods: After reporting the above-mentioned case, we revised the scientific literature, searching for case reports and series of cases of patients with catatonic syndrome and brain tumors. We included articles in which patients were diagnosed with one or more tumoral brain lesions. Articles in which patients with paraneoplastic syndrome, anti-NMDA encephalitis, or other encephalitis and tumor in other regions (e.g., adrenal) were reported were excluded. When feasible, all PRISMA recommendations for systematic reviews were followed. Results: As result, we have found that although catatonic syndrome is a classical diagnostic construct in psychiatry, its pathophysiology can be very diverse even when caused by a brain tumor, as no single brain region can be associated with the syndrome. Moreover, patients do appear to respond very differently to treatments implemented. However, even though not always effective, treatment with benzodiazepines (e.g., lorazepam or diazepam) can be performed since it has been successfully used in various cases of secondary catatonia due to brain tumors, including ours. Conclusion: As far as we know, this is the first case report of a brain metastatic tumor, clinically evidenced by brain imaging, secondary to breast cancer that evolved with a catatonic syndrome ever published. The significant response to the use of benzodiazepines associated with other measures suggests some reliability of interventions such as these in patients with catatonic syndrome secondary to tumoral brain lesions.
Keywords: Brain Tumor, Brain Metastasis, Breast Cancer, Catatonia, Catatonic Syndrome.
INTRODUCTION
Brain tumors can arise from primary lesions originated in the brain itself from native cells of the central nervous system (CNS) or metastatic lesions derived from tumoral tissues outside the CNS which subsequently spread to involve the brain [1]. The most prevalent brain tumors are intracranial metastasis from systemic cancers, followed by meningiomas and gliomas, specifically glioblastoma [2]. During the course of their disease, 15–30% of the patients with cancer are diagnosed with brain metastasis, and autopsy series reveals up to 20–40% of patients with cancer will develop metastatic brain tumor [1,3].
The global cancer project (GLOBOCAN 2012) reports breast cancer as the most common cancer in women, accounting for 25.1% of all cancers [4]. Furthermore, breast cancer is the second most common primary tumor responsible for the development of brain metastasis [5,6]. More than half of the patients will develop multiple metastasis [6]. Treatment consists of a multimodality approach using whole-brain radiation therapy, chemotherapy, biological therapies, hormonal therapies, and surgical resection [6,7]. Catatonic syndrome following breast cancer brain metastasis is a rare condition, but it has been reported once [8].
Catatonia is a neuropsychiatric syndrome characterized by abnormal movements and behaviors [9]. It manifests both as a primary psychiatric condition or secondary to a wide range of medical and neurological diseases [9-11]. Benzodiazepines and ECT are the most effective treatments for the catatonic syndrome known until now [12]. However, when secondary to a medical or neurological condition, catatonia must have its underlying cause treated properly [10]. Finally, some authors have argued that when catatonia is due to a neurologic condition, it may present a suboptimal response to conventional treatments [13]. Thus, the present article aims to report a rare case of secondary catatonia due to a metastatic brain tumor. Informed consent has been provided by the family members and by the patient herself. We further provide a literature review regarding previous studies of catatonia related to brain tumors.
CASE REPORT
Herein we would like to report the case of Mrs. G.A.S., a Brazilian 54-year-old woman diagnosed with a stage IV invasive ductal breast carcinoma. She completed a palliative chemotherapy program two months after the diagnosis and, one month later, due to a severe and persistent headache, a cranial nuclear magnetic resonance (NMR) found a left middle frontal gyrus metastatic focal nodular lesion (Figures 1&2). Thus, she was administered 16mg/day oral dexamethasone to manage brain swelling and, after twelve days, started fluctuating confusion and temporospatial disorientation. Three days after these clinical signs, she received two radiotherapy sessions, but her neuropsychiatric status deteriorated. She was progressively more confused, disoriented, and was presenting sleep-wake cycle disruption and psychomotor agitation episodes, which led the oncology outpatient team to refer the patient to the emergency department.
.png)
Figure 1. Axial Flair.
.png)
Figure 2. 3D Sagittal.
After hospital admission, Mrs. GAS was prescribed oral risperidone 1mg every 8 hours (q8H) for psychomotor agitation and oral dexamethasone 4mg q8H. Physical examination found no evidence of neurological focal deficit or infectious signs. Laboratory tests were normal, including complete blood count, hepatic and renal functions, C-reactive protein, VDRL, and serum potassium, sodium, calcium and B12 vitamin. Electroencephalogram equally showed no abnormalities. Liquor analysis found an unspecific increase in cerebrospinal fluid protein level. Cranial tomography showed the same lesion found in the previous NMR.
Three days after admission, liaison psychiatry evaluation identified cervical dystonia and found the patient to be still confused and disoriented, although psychomotor agitation remitted. Therefore, risperidone was discharged.
Three days after the first liaison psychiatric evaluation, Mrs. GAS manifested prominent catatonic signs, reaching a clinical score of 21 points as accessed by the Busch-Francis Catatonia Rating Scale (BFCRS). She exhibited immobility, mutism, staring, posturing, grimacing, mannerisms, rigidity, negativism, muscle resistance, perseveration, and ambitendency. There were no depressive symptoms, delusions, hallucinations, fever, or autonomic abnormality as well as conscious disturbances. Therefore, a diagnosis of Catatonic Disorder due to another medical condition was performed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-V) and a challenge benzodiazepine therapeutical test with 5mg intravenous diazepam showed rapid improvement of catatonic symptoms, with an after-test BFCRS of 9. Then, oral lorazepam 1mg q8H was prescribed and dexamethasone was reduced to 10mg/day.
In the following five days, lorazepam was gradually increased to 8mg/day and catatonic signs progressively decreased. Daily BFCRS score evolved as follows (in points): 21-9-8-5-1-0. Laboratory tests remained normal and autonomic abnormalities were absent. On the ninth day of lorazepam, the patient was discharged to outpatient follow-up care with a prescription of lorazepam 8mg/day and dexamethasone 8mg/day. Seven days after hospital discharge, BFCRS score remained 0 and the only complaint was sedation; lorazepam was then reduced to 6mg/day.
Past psychiatric history was unremarkable except for a mild depressive episode after the death of one of her sons successfully managed with fluoxetine 20mg/day for a six months interval. Apart from the breast cancer, there was no history of clinical comorbidities and substance abuse.
METHODS
We have conducted a revision using the words “catatonia” AND “brain tumor” in the following database: PubMed, APA PsycNET, SciELO, and BIREME. When feasible, all PRISMA recommendations for systematic reviews were followed. The data search was performed in July 2021 in the article's titles and abstracts. All the articles were screened and selected by one of the authors. Afterward, all the other authors revised the list of the selected articles. No divergence emerged from this process.
All case reports and series of cases of patients suffering from a catatonic syndrome due to one or more tumoral brain lesions were included, as long as they were written in English, Spanish or Portuguese. Articles written in other languages were excluded. Furthermore, those articles presetting patients with paraneoplastic syndrome, anti-NMDA encephalitis or another encephalitis, and tumor in other regions (e.g., adrenal) were also excluded.
The data from the articles were collected by all the authors. The collection was done independently. The articles were randomly attributed to having their information collected by one of the authors. Then, we extracted information concerning the patient's age, the histological type of the tumor, the brain region affected by the tumor, the clinical features displayed by the patients as well as the treatment used in each case and its outcome (Table 1). No other information was systematically collected.
RESULTS
As a result of our selection criteria, we have retrieved thirty articles. Other articles considered relevant, regardless of being found in the primary reference or other sources, were also included. Of all these, only eight were in accordance with our inclusion and exclusion criteria. All of these were fully and carefully read (Diagram 1).
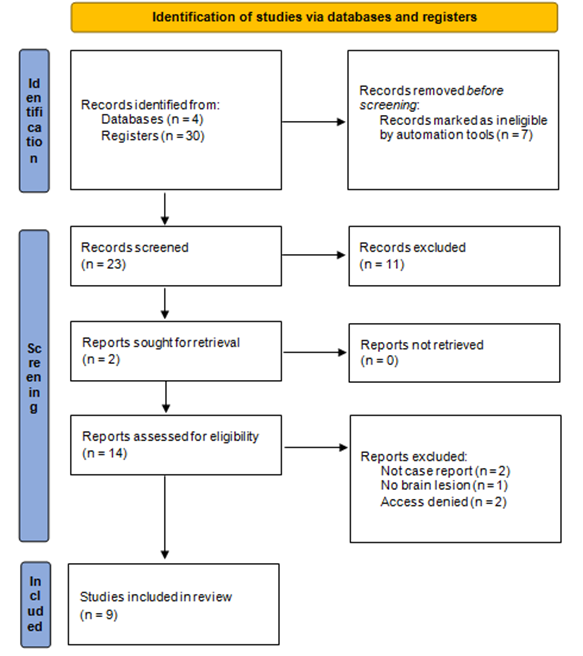
Diagram 1. Identification of studies via databases and registers.
Table 1. The clinical features displayed by the patients as well as the treatment used in each case and its outcome.
|
Age |
Histological |
Brain Region |
Clinical Features |
Treatment |
Outcome |
|
|
Cambruzzi et al. [14] |
56-year-old |
Gliosarcoma |
Left frontal lobe |
Catatonia and apathy |
Surgical resection |
Not reported |
|
Massengale et al. [15] |
53-year-old |
Craniopharyngioma |
Suprasellar extending into the sella and superiorly into the region of the hypothalamus |
Cognitive decline, refusal to speak or to take food or liquids by mouth and paranoid ideation. Bush-Francis of 9 points |
Lorazepam 1mg intramuscular and surgical resection |
No response to lorazepam and great response to surgical resection: Bush- Francis of 0 points |
|
Villantoy-Echegaray et al. [16] |
58-year-old |
Suggestive tuberculous granuloma + related edema |
Left parietal lobe |
Catatonic syndrome |
Corticotherapy (cerebral edema treatment) |
Catatonia improvement |
|
Arora, M., &Praharaj, S. K. [17] |
45-year-old |
Butterfly glioma |
Corpus callosum with extension into adjacent medial frontal cortex and lateral ventricles |
Organic catatonic syndrome |
Lorazepam 6mg and, afterwards, neurosurgery |
No response with lorazepam and death afterwards |
|
Sheline, Y. I., & Miller, M. B. [18] |
32-year-old |
Microadenoma |
Pituitary gland |
Stopped eating and talking, and remained motion- less |
Desipramine 200mg per day, as well as 30 mg per day of thiothixene and 40mg per day of diazepam |
No response with desipramine and great response to thiothixene and diazepam |
|
Kathy Waller, AllaBorik& Connie Choi [8] |
42-year-old |
Cytology on CSF was positive for adenocarcinoma malignant cells |
No evidence of brain tumor in CT or RNM, however cytology on CSF was positive for adenocarcinoma malignant cells |
Altered consciousness, mutism, unresponsive to commands, echolalia, alternation from stupor to agitation, waxy flexibility and other symptoms |
No response with benzodiazepines or valproic acid (patient with bipolar disorder). Bilateral electroconvulsive therapy during three days |
Fully recovered from the catatonic syndrome. Sustained remission during a three months follow-up |
|
Anouchka Franssen & Pascal Sienaert [19] |
57-year-old |
Temporal glioblastoma |
Temporal lobe |
State of self-neglect, staring gaze, flattened facial expression, echolalia, increased motor activity, catalepsy and other catatonic symptoms |
Lorazepam 1mg four times a day |
Gradual improvement, with disinhibited behaviors, aggressive outburst and other symptoms thereafter |
|
Miratul M. K. Muquit, et al. [20] |
21-year-old |
Grade IV astrocytoma |
Right frontal lobe |
Socially withdrawn and apathetic |
Fluphenazine 50mg IM weekly |
Neuroleptic malignant syndrome |
|
Neuman E. Et al. [21] |
24-year-old |
Low-grade astrocytoma |
Peduncular subthalamic |
Apragmatism, mutism and imobility |
L-dopa and bromocriptine |
No response to levodopa and good response after bromocriptine |
|
Neuman E. Et al. [21] |
15-year-old |
High-grade astrocytoma |
Thalamic tumor |
Negativism, mutism, NMS and anterograde amnesic |
Intraventricular drain |
Death soon after discovered |
|
Neuman E. Et al. [21] |
23-year-old |
Pilocytic grade 3 astrocytoma |
Revolving third ventricle |
Anxiety, agitation and incoherent speech followed by apragmatism and indiference |
Ventricle shunt, haloperidol and radiotherapy |
Incomplete neurological and psychological improvement but satisfactory |
|
Neuman E. Et al. [21] |
19-year-old |
Craniopharyngioma |
Retrochiasmatic |
Memory deficiency, indifference, akinetic mutism and apragmatism. Afterwards, catatonic syndrome |
Surgical excision |
Spectacular and definitive neuropsychiatric improvement |
|
Neuman E. Et al. [21] |
49-year-old |
Glioblastoma |
Thalamopeduncular |
Inertia and apragmatism |
Thalamopeduncular radiotherapy and chemoterapy |
Significant improvement of psychiatric symptoms followed by death |
|
Neuman E. Et al. [21] |
24 |
Unknown TVH |
Not related |
Akinesia, mutism and avoiding contact |
Intraventricle shunt neuroleptics and brief radiotherapy |
Totally ineffective. Death in 6 months |
Cambruzzi et al. (2014) published a case report in which a 56-year-old man presented apathy and catatonia due to a gliosarcoma (GS) affecting the left frontal lobe, with midline shift [14]. Her lesion was successfully resected. The authors did not inform whether the catatonia has resolved with the resection or not.
Massengale et al. (2009) wrote a case report of a 53-year-old man who evolved with cognitive decline and with a refusal to speak or to take food or liquids by mouth [15]. A Bush-Francis Catatonia rating scale was applied and revealed a score of 9 points. A trial of lorazepam for presumed catatonia was initiated but did not result in any neurologic improvement. A magnetic resonance imaging study of the brain revealed a cystic suprasellar mass extending into the sellar and superiorly into the region of the hypothalamus. When this lesion was then resected, the diagnosis of craniopharyngioma was given to the patient. Postoperatively, the patient's alertness improved, and he was able to follow simple verbal commands. A retrospective review of his clinical status on postoperative day 4 suggests a Bush-Francis Catatonia rating scale score of 0 points.
Vilantoy et al. (2019) published a case report of a 58-year-old man with no previous pathological history, presenting with catatonic syndrome starting one-week before [16]. Neuroimaging exams showed a tumor in the left parietal region with intense surrounding edema, suggestive of tuberculous granuloma. The edema was resolved with the use of corticosteroids, which led to the disappearance of the catatonia. Unlike other reports in which the catatonic syndrome resolved with the excision of the tumor mass, in this case, the treatment of cerebral edema completely resolved the catatonia.
Arora, M., & Praharaj, SK (2007) published a case report in which a 45-year-old man, with no previous pathological history, started to exhibit for three months, increased urinary frequency, followed by forgetfulness, crying spells, decreased socialization, and hallucinatory behavior for one month and refusal to eat, maintenance of awkward postures and urinary incontinence for one week [17]. Physical examination revealed bilateral stiffness and sharp reflexes, and blurring of the nasal margin of the optic discs was suggestive of early papilledema. In the mental state exam, he was uncooperative, mute, had psychological pillow posture, mismatched, and negativism. He was diagnosed with organic catatonic syndrome. His catatonic symptoms did not improve with lorazepam 6mg per day. CT without contrast of the brain revealed a large butterfly glioma involving the knee and corpus callosum, extending into the adjacent medial frontal cortex and lateral ventricles. He was referred to the neurosurgery department, where he eventually died.
Sheline, Y. I. et al. (1986) reported a case of a 32-year-old woman with a history of catatonic schizophrenia for three years who was admitted to the inpatient service after she stopped eating and talking and remained still [18]. On admission, she did not answer questions, looked straight ahead, and remained seated or standing wherever she was led. Furthermore, there was no spontaneous oral ingestion. However, a CT scan showed a minimally convex pituitary with a lower low density suspected of microadenoma. Alongside the possibility of a major depressive disorder, a six-week trial with desipramine was started, reaching a daily dose of 200 mg. During week’s four to six, the patient was treated with 30 mg per day of thiothixene for catatonic schizophrenia. By the time desipramine was stopped, she had not improved. It was decided to start a study with diazepam. On the second day of treatment, with 30mg of diazepam, the patient improves. From that moment on, she started to speak fluently and participate in social activities. Throughout her treatment with diazepam, she continued to take 30 mg per day of thiothixene. A follow-up evaluation, fifteen months after starting diazepam at a dose of 40mg per day, revealed that she still has auditory hallucinations and delusions of satanic possession. However, catatonic symptoms such as mutism, immobility, and catalepsy did not return.
Kathy Waller, Alla Borik & Connie Choi (2000) wrote about a 42-year-old bipolar woman that presented a sudden onset of word-finding difficulty and lapses in concentration during conversations [8]. During her hospitalization, she increasingly became catatonic. Altered consciousness, mutism, unresponsive to commands, echolalia, and alternation from stupor to agitation, and waxy flexibility were some of the symptoms found in her case. Brain imaging revealed no brain tumor, however, cytology was collected during neurosurgery done to treat some new subdural hematomas over the convexities from the vertex to the temporal regions bilaterally developed during her hospitalization (and not found in her admission CT) found adenocarcinoma malignant cells. No improvement was seen with the use of benzodiazepines or valproic acid. Three bilateral ECT treatments within three days were done. Thereafter, the catatonic syndrome achieved full remission, which was still present during a three-month follow-up.
Anouchka Franssen & Pascal Sienaert (2018) published a case report of a 57-year-old man with no previous psychiatric history, presenting with a depressive episode with catatonic syndrome [19]. Neuroimaging exams showed a tumor in the right temporal lobe with uncal herniation and a mass effect. The catatonic syndrome was treated with the use of lorazepam 4mg per day, which led to the disappearance of the catatonia. However, thereafter the patient evolved with disinhibited behavior, with sexual acts, sudden aggressive outbursts, and endless discussions about rules and regulations on the ward. Neurosurgical resection of the entire tumor was successful. The follow-up has shown that the patient could resume work 5 months after the operation.
Muquit et al. (2001) wrote about a healthy 21-year-old Afro-Caribbean man that became increasingly socially withdrawn and apathetic. Psychiatric assessment noted a reduction of spontaneous speech and poor eye contact and absence of previous hallucinations or delusions [20]. He stood motionless for long periods without spontaneous movement. After a diagnosis of schizophrenic catatonia, fluphenazine (50mg IM weekly) was started but they had to stop it after five weeks because of a neuroleptic malignant syndrome. After two months, the patient developed progressive left-side weakness and focal neurological deficit, with Fisher's sign associated. MR showed alteration on the white matter of the right hemisphere and CSF raised protein that otherwise was normal. After right frontal lobe biopsy, grade IV astrocytoma was found.
Neuman et al. (1996), published a review article about six patients with catatonia and subthalamic mesencephalic tumors with hydrocephalus involving ventricles [21]. They traced parallels between neurological clinical and psychiatric signs. Neuronal circuits similar to those involving Parkinson's disease and dopamine neurotransmitters were associated with intracranial pressure variations. Afterward clinical and laboratory data on schizophrenia concur to suggest that organic etiology could be a causal factor in psychiatric disorders.
DISCUSSION
Our revision points out the fact that, although catatonic syndrome is a classical diagnostic construct in psychiatry, its pathophysiology can be very diverse even when caused by a brain tumor. There was no single brain region associated with the syndrome. On the other hand, patients responded very differently to the treatments implemented. We were unable to find a fixed response pattern from which we could hypothesize a predictor of good or poor response to benzodiazepines. However, despite that, benzodiazepines were the therapeutic approach most used, presumably because of their good response in another clinical context (primary catatonia). Still, the response to benzodiazepines was heterogeneous. When feasible, neurosurgery was also frequently recorded as one of the therapeutic options. At the same time, addressing brain swelling with the use of steroids can also be considered as well as other drugs (e.g., bromocriptine or L-dopa) not as classically used in primary catatonia as benzodiazepines. Finally, electroconvulsive therapy (ECT) should always be remembered, especially when other approaches have failed to achieve the expected response or in severe cases of catatonia. In fact, ECT was the therapeutic approach in only one of the cases accessed. However, an impressive response with only three-day sessions was reported.
Our study has some limitations that should be taken into account. First, the available data regarding this topic is mainly derived from case reports. Second, the heterogeneity of the available studies causes difficulties in the comparison between them. For example, some cases did not access clinical response with a clinical scale such as BFCRS. Concurrently, as a rare condition such as secondary catatonia, clinical studies with an experimental design are very difficult to be carried out.
As far as we know, this is the first case report of a brain metastatic tumor, clinically evidenced by brain imaging, secondary to breast cancer that evolved with a catatonic syndrome ever published. This case shows that brain metastasis secondary to breast cancer may course with a catatonic syndrome. Previous evidence suggests secondary catatonia accounts for as much as 20-50% of all cases [22,23]. Therefore, although classically related to primary psychiatric disorders, this case highlights the need for medical staff to always look for organic causes of catatonic symptoms.
Taken together, this case report, along with the previous literature, contributes to the understanding of the catatonic syndrome secondary to a brain tumor, pointing out that this syndrome can be very heterogeneous regarding its etiology, physiopathology, and treatment response. No single cerebral region or structure can be unequivocally and exclusively related with catatonia as well as no single histological brain tumor subtype. There is currently a lack of good quality evidence to drive optimal treatment decision-making. Still, even though not always effective, treatment with benzodiazepines (e.g., lorazepam or diazepam) can be performed since it has been successfully used in other cases of secondary catatonia due to brain tumor, including ours [23]. When appropriate, other biological therapies such as drugs related to the dopaminergic neurotransmission (e.g., bromocriptine) or electroconvulsive therapy may be tried [22].
CONCLUSION
This case report is remarkable because it describes catatonia due to metastatic brain tumor related to the most common cancer in women which, in turn, is the second major cause of metastatic brain tumoral lesions. In accordance with previous data, this case report shows that, when secondary to a medical or neurological condition, catatonia must have its underlying primary medical cause treated properly (e.g., surgical excision, radiotherapy, or treatment of the brain edema), as many patients have clinically improved from this approach, including the one described in this case report. Further longitudinal studies with larger samples sizes addressing treatment response and other relevant clinical features are necessary to better guide therapeutic decisions while managing secondary catatonia due to a medical condition.
FUNDING
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
DISCLOSURE
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
ACKNOWLEDGEMENTS
We would like to thank the Hospital das Clínicas da UFMG for all the support given to us during our research.
REFERENCES
- Patchell R. (2003). The management of brain metastases. Cancer Treat Rev. 29(6):533-540.
- McFaline-Figueroa J, Lee E. (2018). Brain Tumors. Am J Med. 131(8):874-882.
- Hatiboglu M, Akdur K, Sawaya R. (2018). Neurosurgical management of patients with brain metastasis. Neurosurg Rev. 43(2):483-495.
- Ghoncheh M, Pournamdar Z, Salehiniya H. (2016). Incidence and Mortality and Epidemiology of Breast Cancer in the World. Asian Pac J Cancer Prev. 17(sup3):43-46.
- Yeh R, Yu J, Chu C, Ho C, Kao H, Liao G et al. (2014). Distinct MR Imaging Features of Triple-Negative Breast Cancer with Brain Metastasis. J Neuroimaging. 25(3):474-481.
- Rostami R, Mittal S, Rostami P, Tavassoli F, Jabbari B. (2016). Brain metastasis in breast cancer: a comprehensive literature review. J Neurooncol. 127(3):407-414.
- Bailleux C, Eberst L, Bachelot T. (2020). Treatment strategies for breast cancer brain metastases. Br J Cancer. 124(1):142-155.
- Waller K, Borik A, Choi C. (2000). Breast Cancer, Bipolar Disorder, Catatonia, and Life-Preserving Electroconvulsive Therapy. Psychosomatics. 41(5):442-445.
- Rasmussen SA, Mazurek MF, Rosebush PI. (2016). Catatonia: Our current understanding of its diagnosis, treatment and pathophysiology. WJP. 6(4):391-398.
- Ahuja N. (2000). Organic Catatonia: A Review. Indian J Psychiatry. 42(4):327-346.
- Posada J, Mahan N, Abdel Meguid A. (2021). Catatonia as a Presenting Symptom of Isolated Neurosarcoidosis in a Woman with Schizophrenia. J Acad Consult Liaison Psychiatry. 62(5):546-550.
- Pelzer A, van der Heijden F, den Boer E. (2018). Systematic review of catatonia treatment. Neuropsychiatric Disease and Treatment. 14:317-326.
- Fishman D, Beach S, Quinn D, Roy D. (2017). Special Interest Group-sponsored Updates in Psychosomatics (SIG-UPs): Understanding the Pathophysiology of Catatonia Through Associated Neurological Insults (Neuropsychiatry SIG). Psychosomatics. 58(1):90-91.
- Cambruzzi E, Pegas K. (2014). Osseous metaplasia in gliosarcoma: an unusual histologic finding. Case report. Journal Brasileiro de Patologia e Medicina Laboratorial. 50(2):159-164.
- Massengale J, Tafti B, Large L, Skirboll S. (2009). Reversal of Preoperative Catatonic State by Surgical Resection of an Adult-onset Craniopharyngioma. Cogn Behav Neurol. 22(1):67-71.
- Villantoy-Echegaray A, Changana-Arroyo A, Cruzado L. (2019). Catatonía secundaria a edema cerebral. Psiquiatría Biológica. 26(2):56-59.
- Arora M, Praharaj SK. (2007). Butterfly glioma of corpus callosum presenting as catatonia. World J Biol Psychiatry. 8(1):54-55.
- Sheline YI, Miller MB. (1986). Catatonia relieved by oral diazepam in a patient with a pituitary microadenoma. Psychosomatics. 27(12):860-862.
- Franssen A, Sienaert P. (2019). Temporal glioblastoma presenting as catatonia. BMJ Case Rep. 12(3):e224017.
- Muqit MMK, Rakshi JS, Shakir RA, Larner AJ. (2001). Catatonia or abulia? A difficult differential diagnosis. Mov Disord. 16(2):360-362.
- Neuman E, Rancurel G, Lecrubier Y, Fohanno D, Boller F. (1996). Schizophreniform Catatonia on 6 Cases Secondary to Hydrocephalus with Subthalamic Mesencephalic Tumor Associated with Hypodopaminergia. Neuropsychobiology. 34(2):76-81.
- Oldham MA. (2018). The Probability That Catatonia in the Hospital has a Medical Cause and the Relative Proportions of Its Causes: A Systematic Review. Psychosomatics. 59(4):333-340.
- Smith JH, Smith VD, Philbrick KL, Kumar N. (2012). Catatonic Disorder Due to a General Medical or Psychiatric Condition. JNP. 24(2):198-207.