Information Links
Related Conferences
Previous Issues Volume 10, Issue 2 - 2025
Autism and Focal Seizures Associated with Left Hemispheric Cortical Atrophy: A Novel Clinical Pattern
Aamir Jalal Al-Mosawi*
Advisor Doctor and Expert Trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq
*Corresponding Author: Aamir Jalal Al-Mosawi, Advisor Doctor and Expert Trainer, Baghdad Medical City and Iraqi Ministry of Health Baghdad, Iraq, Email: [email protected]
Received Date: October 16, 2025
Published Date: October 29, 2025
Citation: Al-Mosawi AJ. (2025). Autism and Focal Seizures Associated with Left Hemispheric Cortical Atrophy: A Novel Clinical Pattern. Mathews J Psychiatry Ment Health. 10(2):54.
Copyrights: Al-Mosawi AJ. (2025).
ABSTRACT
Background: Autism disorders are a very complicated and multifarious group of chronic disorders that are characterized by early impairment in social interaction and communication. The diagnosis of autism is clinical and is based on the presence of characteristic diagnostic manifestations resulting from impaired social interaction and communication, which cause the two major diagnostic features of autism: the lack of appropriate responsiveness to one's own name and the lack of eye contact. Poor speech development with difficulties in using and understanding language, and repetitive body movements including hand flapping, and spinning, or behavior patterns are important associated features of autism disorders. Autism disorder is a heterogeneous group of disorders that are typically considered a functional neurodevelopmental disorder without consistent radiological findings. Consequently, routine brain imaging is not widely recommended. For decades, autism disorders have been considered life-long disorders without curative therapies. Recently a new therapeutic approach aiming primarily at improving and curing the two major diagnostic features of autism which are poor responsiveness to their name and poor eye contact, has been increasingly used. Injectable cerebrolysin is the main therapeutic component in this new therapeutic approach. Patients and methods: A 6-year-old girl who initially presented with autism disorder features in early childhood, responded remarkably to a six-month course of injectable Cerebrolysin, but later regressed after treatment discontinuation and subsequently developed focal seizures. Results: A non-contrast CT brain scan revealed asymmetric cortical atrophy predominantly in the left posterior frontal and parietal lobes, particularly affecting the perisylvian region. The sulci appeared widened and the underlying white matter volume reduced. There were no calcifications or signs of progressive degenerative disease. Conclusion: This paper highlights a unique clinical entity where early childhood autism is associated with focal cortical atrophy and later development of epilepsy. The marked initial response to Cerebrolysin underscores the potential role of neurotrophic therapy in modulating neuroplasticity and improving functional outcomes even in patients with underlying structural abnormalities. The recurrence of symptoms and emergence of seizures following treatment cessation suggests a progressive or evolving neurological basis rather than a purely static neurodevelopmental disorder.
Keywords: Autism, Focal Epilepsy, Cortical Atrophy, New Clinical Entity.
INTRODUCTION
Autism disorders are a very complicated and multifarious group of chronic disorders that are characterized by early impairment in social interaction and communication.
The diagnosis of autism is clinical and is based on the presence of characteristic diagnostic manifestations resulting from impaired social interaction and communication, which cause the two major diagnostic features of autism: the lack of appropriate responsiveness to one's own name and the lack of eye contact. Poor speech development with difficulties in using and understanding language, and repetitive body movements including hand flapping, and spinning, or behavior patterns are important associated features of autism disorders.
The variation in speech and cognitive development results in the subtypes of autism. The mildest type of autism was the first to be reported in the medical literature, and is associated with acceptable speech and cognitive developments.
Autism disorders were first recognized by Grunya Efimovna, a Soviet pediatric psychiatrist in 1925, and she called these disorders autistic psychopathy.
In 1944, Hans Asperger, an Austrian physician, reported children having the mildest type of autism, which was first described by Grunya Efimovna in 1925.
However, in 1981, Lorna Wing called the mildest type of autism Asperger syndrome.
The type of autism generally considered the classic type is Kanner syndrome, named after Leo Kanner, who described this type in 1943.
Despite being associated with normal or high intelligence, it is associated with significant delay in speech development. Autism disorders have become increasingly known as pervasive developmental disorders, especially in the United Kingdom since the 1980s.
Asperger syndrome became a standard diagnosis in 1992 when it was included in the tenth edition of the World Health Organization's diagnostic manual, the ICD ten. In 1994, it was added to the fourth edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, the DSM.
Children with autism disorder who have subnormal intelligence, but without significant mental retardation, are considered to have typical autism.
Considering, the inability to accurately determine the IQ of autistic children, the absence of significant mental retardation in such children is suggested by having acceptable adaptive behaviors, including eating with a spoon, bowel control, going to the bathroom, and other adaptive skills based on the child’s age.
Atypical autism includes autism associated with mental retardation and also regressive autism when patients acquire social and communication skills normally early in life, but lose them.
Making an accurate diagnosis of the type of autism is not an easy task. In 2013, the American Association of Psychiatry used the term autism spectrum disorder to represent all types of autism disorders. This term can be used, especially during referral, to avoid the embarrassment of sending a patient with an inaccurate diagnosis of the type of autism.
Therefore, the term autism spectrum disorder was first used in the 2013 edition of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, the DSM-5. The term autism spectrum disorder has been increasingly used interchangeably with pervasive developmental disorders.
A worth-mentioning older classification of autism disorders, the pervasive developmental disorders included three main types: Autism, Rett syndrome, and disintegrative childhood disorder, also called Heller syndrome.
Considering this classification and the rare syndromic types of autism, we can gain some understanding of how complex these disorders are.
Autism disorders are a heterogeneous group of disorders that are typically considered a functional neurodevelopmental disorder without consistent radiological findings. Consequently, routine brain imaging is not widely recommended [1-17].
A 2020 study reported that brain imaging abnormalities in patients with autism disorders include arachnoid cyst, agenesis of the corpus callosum, evidence of vasculitis (In Heller syndrome), and brain imaging abnormalities related to a coexisting condition such as cerebral palsy [18].
Traditional treatments for autism have predominantly focused on associated symptom management, including behavioral interventions and pharmacotherapy.
However, the quest for a cure has remained elusive until recent breakthroughs, which have shed light on promising avenues for intervention. Neuroleptics and other medications such as baclofen and ondansetron have been used with some benefit to control behavioral abnormalities and hyperactivity [1,2,5,7,10,11,15-17,19].
Risperidone is probably the most commonly used neuroleptic in the more severe forms because of the lack of extrapyramidal side effects. Children with autism disorders may also need speech therapy, social skill training, special education, which can be individualized, and behavioral psychotherapy.
For decades, autism disorders have been considered lifelong disorders without curative therapies, despite a variety of medications that have been tried, including pyridoxine, magnesium, thiamine, biotin, folic acid, and omega-three.
Autism curative therapies should target the core diagnostic features of autism including poor responsiveness to name and lack of eye contact.
During the previous decade, at least 19 patients have been reported in the literature including 18 patients from Iraq and one patient from Cuba have achieved cure of the major autistic diagnostic features with the use of a new therapeutic approach using individualized courses of intramuscular cerebrolysin as the curative agents [11,20,21].
During a comprehensive study spanning from December 2017 to November 2019, we observed 116 patients with various autism disorders at the Children Teaching Hospital of Baghdad Medical City. The patients’ age ranged from two years to 16 years. These 116 patients were reported in several publications. Clinical details of these patients and their treatments were included in a book translated into several languages.
All the patients had very poor speech development except the patients with Asperger syndrome. Most of the patients with a diagnosis other than Asperger syndrome were not saying any word, and few patients were saying a few words. Most patients were treated with a new therapeutic approach which included injectable cerebrolysin as the main therapeutic component. Marked improvement or disappearance of autistic features in these disorders has not been reported with any therapy before.
Our research unveiled a groundbreaking approach, as utilizing injectable cerebrolysin in the treatment of autism disorders was associated with a remarkable efficacy in ameliorating autistic features, leading to unprecedented levels of improvement in some cases.
The new treatment approach aimed primarily at improving the cardinal features of autistic disorders, which include impairment of social interaction, mostly manifested by poor responsiveness to their name, and infrequent engagement with others manifested by poor eye contact and infrequent looking at faces. It was not possible to follow all the patients regularly, nor was it possible to document details of the treatment and responses of all patients.
However, through meticulous documentation and follow-up, we observed significant enhancements in social interaction, communication skills, and behavioral patterns among patients undergoing this novel treatment regimen. Notably, the initial phase of our study documented the complete remission of autistic features in twelve patients, marking a pivotal milestone in autism research and clinical practice [11].
Subsequent observations have reinforced the transformative potential of this innovative therapy, illustrating tangible improvements in the quality of life for individuals with autism and their families. Treatment was also associated with initiation of speech and improvement of repetitive behaviors [11-15].
Therefore, we have been using this new therapeutic approach as the standard approach for the treatment of autism disorders in our clinical practice. We have been trying to document our clinical practice through scientific publications as possible [12-15]. It was possible to document cure of the major autistic features in the thirteenth patient. He had an autosomal recessive autism with mental retardation, and his younger brother was one of the first 12 documents patients who cured from the major autistic features [16,17].
The first book which described the cure of the autistic features [2] was included in Bookauthority’s lists of best books of all time [22]. Therefore, we have been consulted about the treatment of autism from many countries in the world including the United Kingdom, Canada, United Arab of Emirate, Tunisia, Palestine, India, and Pakistan, and many of the international cases have been reported [21,23-27].
While these results are indeed promising, it is essential to acknowledge the ongoing challenges in autism treatment. Achieving a cure represents only the first step; sustained rehabilitation and support are imperative to address lingering cognitive, behavioral, and social difficulties.
Long-term follow-up studies have underscored the importance of continued intervention and support to optimize outcomes for individuals with autism. Despite achieving remission of autistic features, patients may continue to encounter challenges in learning and behavior that necessitate tailored interventions and ongoing therapeutic support [16,17,20].
Cerebrolysin is a mixture of free amino acids (85%) and 15% biologically active low molecular weight amino acid sequences which include low molecular weight neuro-peptides (Brain-derived neurotrophic factor, glial cell line-derived neurotrophic factor, nerve growth factor, ciliary neurotrophic factor.
Cerebrolysin has been used safely with benefit in a variety of neuro-psychiatric disorders including idiopathic mental retardation, cerebral palsy, brain atrophy, myelomeningocele, pediatric juvenile spinal muscular atrophy, pediatric Charcot Marie Tooth disease, kernicterus, and agenesis of corpus callosum with colpocephaly [28-38].
Recently, the novel association of autism with congenital non-syndromic cavum septum pellucidum has been reported [39].
This paper describes a new clinical entity characterized by the association of autism disorder features in early childhood, responded remarkably to a six-month course of injectable cerebrolysin, but later regressed after treatment discontinuation and subsequently developed focal seizures that was attributed to focal cortical atrophy.
PATIENTS AND METHODS
At about the age of two and half years, the girl received the diagnosis of autism. She had poor speech development and the two major diagnostic features of autism. At the clinic, she was not responding to her name, had no eye contact (Figure-1A).
She received intramuscular cerebrolysin 2.5 ml every third day in the morning (Ten doses monthly) for five months, and 3 ml every third day in the morning (Ten doses monthly) during the sixth month. She was also receiving oral risperidone 1mg at night to control hyperactivity. After cure of major autistic features at about the age of three years, she was saying less 20 words, and she was having echolalia sometimes.
Therefore, oral piracetam 400 mg once daily in the morning, and oral citicoline 200 mg daily in the morning were prescribed to improve cognitive skills and speech development. Oral risperidone was continued.
At about the age of 4 years, in addition to the cure of autism, she experienced an improvement in speech development and cognitive skills. At the clinic, she was responding to her name and had good eye contact. She accepted to take a pen to draw something she likes (Figure-1B, C, D, E).
Thereafter, the parents were not keen in bringing her for regular follow-up, but early during the year 2005, the girl was seen and there was recurrence of the main autistic features. She was not showing good response to name nor acceptable eye contact. Further course of cerebrolysin were recommended, but the parents thought that girl was fine and responsive to them and that was attributed to the period of cure of the autistic features during which the parents become familiar to the girl.
During May, 2025, at about the age of six years, her autistic features returned, and within few weeks she presented with new-onset seizures. Electroencephalography demonstrated focal epileptiform activity.

Figure-1A. At the clinic, the girl was not responding to her name, had no eye contact.

Figure-1B. After cure of autism, at the clinic, she was responding to her name and had good eye contact.
Figure-1C. After cure of autism, at the clinic, she accepted to take a pen to draw something she likes.
Figure-1D. After cure of autism, at the clinic, she accepted to take a pen to draw something she likes.
Figure-1E. After cure of autism, at the clinic, she accepted to take a pen to draw something she likes.
RESULTS
A non-contrast CT brain scan (Figure-2) revealed asymmetric cortical atrophy predominantly in the left posterior frontal and parietal lobes, particularly affecting the perisylvian region. The sulci appeared widened and the underlying white matter volume reduced. There were no calcifications or signs of progressive degenerative disease.
Main brain CT-scan findings Abnormal Findings:
1. Asymmetry of Cortical and White Matter Volumes (Suggestive of Focal Cortical Atrophy)
There is evident left cerebral hemisphere volume loss, especially in the left posterior frontal and parietal lobes, as seen by widened sulci and dilated cortical subarachnoid spaces.
The left lateral ventricle appears slightly enlarged compared to the right (ex-vacuo dilatation), which supports underlying parenchymal volume loss on the left side. This asymmetry is subtle but clear across multiple slices.
2. Subtle Cortical Dysgenesis or Malacia
In the affected left hemisphere, particularly the posterior regions, there appears to be poor differentiation between the gray and white matter, which may reflect focal cortical dysplasia or encephalomalacia. This pattern matches well with focal seizure onset zones in pediatric epileptics.
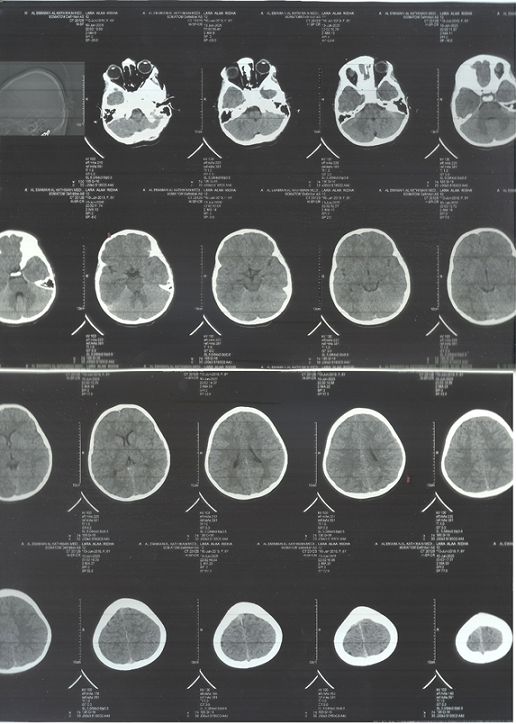
Figure-2A
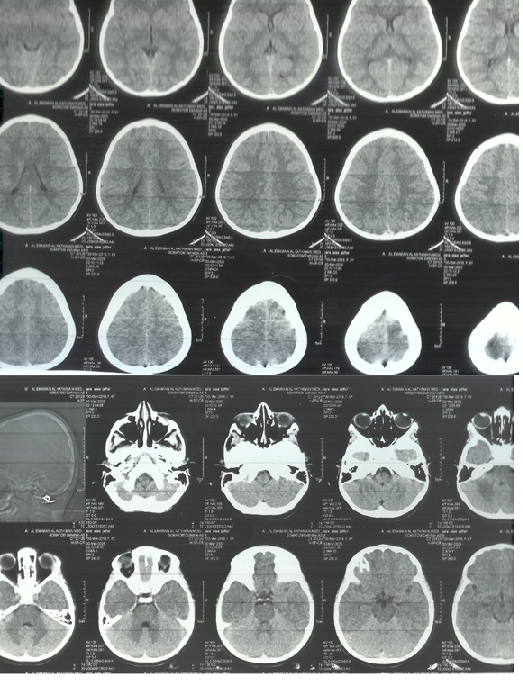
Figure-2B
DISCUSSION
Autism is usually diagnosed without imaging findings. The presence of focal cortical atrophy and subsequent focal epilepsy in the same patient is rare and compelling.
Brain imaging revealed left-sided cortical atrophy, particularly involving the perisylvian and temporoparietal regions.
The left posterior frontal-parietal cortical atrophy, visible on CT, is in a region crucial for language, social cognition, and motor planning. This could explain the patient’s autistic features.
The perisylvian region refers to the brain areas around the Sylvian fissure, especially:
Posterior inferior frontal gyrus (Broca’s area). Superior temporal gyrus (Wernicke’s area). Inferior parietal lobule (supramarginal and angular gyri).
This region, especially on the left side, is critical for language processing, social communication, and higher-order cognitive functions such as:
Language comprehension and expression. Pragmatic speech. Social interaction. Reading, writing, and symbolic thinking.
The focal cortical atrophy noted in the left perisylvian and temporoparietal cortex suggests a congenital or early-acquired static lesion, such as focal cortical dysplasia or sequela of perinatal injury. These regions are critical for language and social cognition, and their dysfunction could underlie both autistic and epileptic manifestations.
This progression strengthens the argument for an organic, evolving neurological process rather than a static neurodevelopmental disorder.
The patient's response to Cerebrolysin, a neurotrophic peptide preparation, indicates preserved neuroplasticity and supports the hypothesis that targeted neurorestorative therapy may offer functional benefits in patients with autism associated with structural brain abnormalities.
Although Landau-Kleffner syndrome was considered, the presence of a clear structural lesion on imaging and early onset of autism before seizures argues against this diagnosis.
Importantly, this case supports the recommendation that neuroimaging be considered in children with autism, especially those who present with regression, seizures, or other focal neurological signs. Early identification of structural lesions may allow for more tailored therapeutic interventions and closer monitoring of neurological evolution.
CONCLUSION
This paper highlights a unique clinical entity where early childhood autism is associated with focal cortical atrophy and later development of epilepsy. The marked initial response to Cerebrolysin underscores the potential role of neurotrophic therapy in modulating neuroplasticity and improving functional outcomes even in patients with underlying structural abnormalities. The recurrence of symptoms and emergence of seizures following treatment cessation suggests a progressive or evolving neurological basis rather than a purely static neurodevelopmental disorder.
ACKNOWLEDGEMENT
The author would to express his gratitude for the parents of the patient who accepted publishing their photos.
Some figures were previously published, and the author has their copyright.
CONFLICT OF INTEREST
None.
REFERENCES
- Al-Mosawi AJ. (2019). Pervasive developmental disorders in Iraqi Children. Journal of Psychiatry Research Reviews & Reports. 1(1):1-8.
- Al-Mosawi AJ. (2019). The pattern of pervasive developmental disorders in Iraqi children. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-3-330-05029-7.
- Al-Mosawi AJ. (2018). Pediatric psychiatry: An accredited training course. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-86510-9.
- Al-Mosawi AJ. (2020). Case studies in pediatric psychiatry: An approach to deep learning. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-620-2-52071-3.
- Al-Mosawi AJ. (2018). A new therapeutic approach for pervasive developmental disorders. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-3-659-86602-9.
- Al-Mosawi AJ. (2018). Asperger syndrome and regressive autism.1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-82643-8.
- Al-Mosawi AJ. (2019). New therapies for Rett syndrome. J Bio Innov. 8(3):301-307.
- Al-Mosawi AJ. (2019). Childhood dementia: Heller syndrome. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-3-330-04944-4.
- Al-Mosawi AJ. (2019). Heller syndrome in two Iraqi children. Clin Res Trials. 5:1-3.
- Al-Mosawi AJ. (2019). The use of cerebrolysin and citicoline in autism and Asperger syndrome. J Bio Innov. 8(1):99-108.
- Al-Mosawi AJ. (2020). Cure of Autistic Disorders: Mission Impossible is Possible in an Illustrated Pioneering Experience. SunKrist Journal of Psychiatry and Mental Health. 1(1):1-20.
- Al-Mosawi AJ. (2021). Atypical Autism Associated with Elevated Gonadotrophin and Precious Puberty: A Very Rare Association or a New Clinical Syndrome? Biomedical Journal of Scientific & Technical Research. 33(2):25686-25689.
- Al-Mosawi AJ. (2022). Catatonia: A Rare Manifestation of Autism. MedPress Psychiatry and Behavioral Sciences. 1(1):1-4.
- Al-Mosawi AJ. (2022). The association of autism with self-injurious behaviors: An educational article. Journal of Clinical Trails and Bioavailability Research. 1(1):1-7.
- Al-Mosawi AJ. (2023). Autism with Severe Mental Retardation: A Therapeutic Challenge and Expert Opinion. Archives in Neurology & Neuroscience. 15(2):1-5.
- Al-Mosawi AJ. (2021). Autosomal Recessive Autism: Cure of the Major Autistic Features. Scholars International Journal of Anatomy and Physiology. 4(8):120-126.
- Al-Mosawi AJ. (2022). Atypical Genetic Autism: Cure of the Major Autistic Features and the Need for Cognitive Improvement and Rehabilitation. MedPress Psychiatry and Behavioral Sciences. 1(1):1-4.
- Al-Mosawi AJ. (2020). Brain Imaging Abnormalities in Autism Disorders. Journal of Clinical Research in Radiology. 3(2):1-3.
- Al-Mosawi AJ. (2015). The use of ondansetron in psychiatry: An educational article and expert opinion. Journal of Drug Delivery and Therapeutics. 3(8):1-2.
- Al-Mosawi AJ. (2024). Advancements in Autism Curative Treatment: A Groundbreaking Therapeutic Approach. International Journal of Clinical Epidemiology. 3(4):1-10.
- Al-Mosawi AJ. (2024). A Patient from Cuba with Classic Autism and the Recommended Evidence-Based Treatment: An Educational Article and Expert Opinion. International Journal of Clinical Reports and Studies. 3(2):1-6.
- Al-Mosawi AJ. Books of Aamir Jalal Al-Mosawi included in Bookauthority’s list of Best Books of All Time on December 15, 2021. DOI: 10.13140/RG.2.2.12396.90240.
- Al-Mosawi AJ. (2022). Cerebral Palsy and Autism Associated with Periventricular White Matter Hyperintensity on Brain Magnetic Resonance Imaging: A New Disorder and Its Treatment. MedPress Psychiatry and Behavioral Sciences. 1(1):1-4.
- Al-Mosawi AJ. (2022). Treatment of Williams syndrome: Evidence-based medicine and expert opinion. Biomedical and Biotechnological Sciences. 1(2):1-3.
- Al-Mosawi AJ. (2022). Treatment of a girl from Tunisia with typical autism: Evidence-based medicine and expert opinion. Biomedical and Biotechnological Sciences. 1(2):1-5.
- Al-Mosawi AJ. (2022). A girl from Pakistan with atypical autism: Expert opinion and a therapeutic recommendation. World Journal of Radiology and Imaging. 1(1):38-41.
- Al-Mosawi AJ. (2023). A Case of Atypical Autism with Mental Retardation in an Adult from Canada: An Educational Article and Expert Opinion. Journal of Brain and Neurological Disorders. 6(4):1-5.
- Al-Mosawi AJ. (2020). Clinical uses of Cerebrolysin in Pediatric Neuropsychiatry. Science World Journal of Pharmaceutical Sciences. 1(1):1-4.
- Al-Mosawi AJ. (2019). New medical therapies for the treatment of myelomeningocele. Surgical Medicine Open Access Journal. 2(4):1-4.
- Al-Mosawi AJ. (2018). A novel therapy for pediatric juvenile spinal muscular atrophy.1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-89719-3.
- Al-Mosawi AJ. (2020). The use of cerebrolysin in pediatric Wohlfart Kugelberg Welander syndrome. MOJ Clinical & Medical Case Reports. 10(1):20-23.
- Al-Mosawi AJ. (2018). A novel therapy for pediatric Charcot Marie Tooth disease. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-8-39043-5.
- Al-Mosawi AJ. (2020). The use of Cerebrolysin in Pediatric Charcot Marie Tooth Disease. Journal of Neurologi Cal Research and Therapy. 3(2):17-21.
- Al-Mosawi AJ. (2018). A novel therapeutic approach for the neurological complications of kernicterus. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-98425-1.
- Al-Mosawi AJ. (2019). The novel use of cerebrolysin and citicoline in the treatment of kernicterus. Online Journal of Neurology and Brain Disorders. 3(1):208-212.
- Al-Mosawi AJ. (2020). New Therapies for the Treatment of Ataxic Cerebral Palsy Caused by Kernicterus. EC Clinical and Medical Case Reports. 3(4):26-31.
- Al-Mosawi AJ. (2019). Agenesis of corpus callosum with colpocephaly: A novel therapy. 1st ed. Saarbrücken, Germany: LAP Lambert Academic Publishing. ISBN: 978-613-9-45076-3.
- Al-Mosawi AJ. (2020). The use of piracetam and cerebrolysin in the treatment of agenesis of corpus callosum with colpocephaly. EC clinical and medical case reports. 3(1):01-05.
- Al-Mosawi AJ. (2024). The novel association of autism with congenital non-syndromic cavum septum pellucidum and its significance: An educational article and expert opinion. Biomedical Studies and Clinical Evaluations. 1(1):1-4.